
Abstract
There is a prevalence of work-related musculoskeletal disorders (WRMSDs) associated with the work of radiologic professionals, especially those doing sonographic examinations. This may be due to the fact that their daily work tasks expose them to the physical risk factors associated with WRMSDs. The purpose of this study was to examine whether radiologic professionals’ knowledge and work practices changed after receiving an educational multimedia tutorial on ergonomics. After multimedia training on ergonomics and safe body mechanics designed by occupational therapy providers, participants reported that their awareness and their work practices improved.
Introduction
Because of the high prevalence of musculoskeletal injury in radiologic professionals, extensive research exists that identifies the risk factors that contribute to the development of these injuries.1–8 However, there are very few studies that have proposed ergonomic solutions to problematic scanning techniques and repetitive tasks required of radiologic professionals. A second gap in the current body of knowledge is research measuring any changes that take place after radiologic professionals receive education about ergonomic work techniques. For purposes of this study, radiologic professionals will refer to health care workers using diagnostic imaging services involving (1) x-rays, (2) radiation, or (3) non-ionizing radiologic imaging techniques used for diagnosis and treatment, specifically medical sonographers and radiologic technologists.
As of 2010, there were an estimated 53 700 medical sonographers 9 and 219 900 radiologic technologists 10 employed in the United States. Studies show that between 80% and 90% of these medical sonographers and between 67% and 83% of radiologic technologists report suffering from some type of pain or discomfort while performing work-related tasks.1,2,5–7,11,12 This number is alarming since it has been shown that only a small percentage of radiologic professionals who experience occupation-related pain report their pain in their workplace and seek treatment.4,13
This particular type of pain or discomfort reported by radiologic professionals while performing work-related tasks is referred to as a work-related musculoskeletal disorder (WRMSD), the term used with similar work categories. Work-related musculoskeletal disorders are defined as work-related “injuries and illnesses involving sprains/strains, joint inflammation, low-back pain, and nerve compression syndromes.”11,12 The biomechanical job requirements of many radiologic professionals, such as repetitive motion, static postures, and awkward body positioning, have been shown to contribute to the high prevalence of musculoskeletal injury or pain.2,4,14,15 These types of injuries often cause pain to be localized in the neck, upper back, shoulders, wrists, and hands.3,4,12 Furthermore, it has been reported that individuals performing jobs with higher exposure to this type of biomechanical stress report a higher percentage of pain, injury, loss of work, and disability than individuals who work with lower exposure to biomechanical stress.13,14
Radiologic imaging for medical diagnosis has increased significantly as the technology has improved. It has been reported that in order to meet work productivity standards, a radiologic professional will perform 6 to 10 sonography examinations per day, typically with few breaks between scans, a behavior that has been shown to be a risk factor for a WRMSD.
4
Other studies have also reported that performing 100 or more sonographic examinations per month has a positive relationship with WRMSDs.16,17 The high prevalence of injury and symptoms can lead to a decrease in employee performance and can be very expensive for the facilities involved.18,19 The literature shows that
an injured sonographer can cost an employer over a half million dollars each year through various means, such as: 1) loss of revenue – $52,000 per year chargeable revenue per injured sonographer, 2) workers’ compensation – $32,000 per injury per year, 3) replacement staff – $60,000–$80,000 per year, and 4) medical bills – $20,000 per year (does not include surgical treatment).
19
Accompanied by the implications of the multiple negative effects for the employers involved, an increased incidence and prevalence of WRMSDs leads to many negative effects for the radiologic professional as well. These include a decreased quality of life, an impingement on the ability to complete personal and professional tasks, increased health care costs, increased missed days at work, and possibly even involuntarily leaving their profession prior to retirement age. 7
Literature Review
There is minimal empirical research evidence regarding sonographic-specific ergonomic techniques that can be put into practical use in an attempt to reduce the risk of WRMSDs. When interviewed, sonography professionals and researchers have described and discussed ergonomic scanning techniques that can be applied while performing abdominal and transvaginal examinations. 20 Information from other work provided a foundation for the ergonomic techniques outlined in the multimedia tutorial used by participants in this research study. The remaining research studies investigating specific WRMSDs in sonographers have focused on describing the prevalence of WRMSDs, identifying and describing unsafe scanning postures, proposing general solutions to the issues, and discussing the effectiveness of implementing general ergonomic techniques. A survey study by Evans et al 12 in 2009 analyzed the responses of 3000 practicing sonographers regarding their experiences with musculoskeletal pain and scanning. Results found that 90% of the sonographers were scanning in pain. The most common painful locations have been shoulder, neck, wrist, upper back, hands, and feet. Primary aggravating factors included applying pressure on the transducer, sustained abduction of the arm, and twisting the neck and back.
Previous research has obtained objective information from sonographers during the performance of scans to identify specific techniques, postures, and positions that contribute to the development of musculoskeletal injury.21,22 These studies concluded that the major physical risk factors include (a) large shoulder abduction angle, (b) high force required to keep the transducer on each patient, (c) reaching across patients, (d) twisting the torso and neck, (e) non-neutral wrist positions, (f) excessive and repetitive force with transducer, and (g) twisting and pushing motions of the wrist. They demonstrated the need for sonographers to spend a large amount of time in non-neutral positions, frequently moving arm joints to maneuver the transducer and using large grip forces on the transducer to successfully complete examinations. Furthermore, they found that most sonographers performed many different types of scans, which required using a unique position and technique for each type of scan in order to obtain a clear image. Conclusions drawn from this research suggested that to reduce WRMSDS, specific risk factors and ergonomic solutions must be identified for each type of scan. 22
A study by Roll et al 23 collected observational data using the Rapid Upper Limb Assessment (RULA), a tool that produces a score from 0 to 7 indicating the degree of exposure to physical risk. Their results determined that the participants noted a RULA score of 0.67 at the beginning of the day and a score of 2.38 at the end of the day, indicating that pain increased throughout each participant’s workday. Sonographers were assessed using the RULA with five specific types of examinations: upper extremity venous, transvaginal pelvic, transabdominal obstetric, carotid duplex, and lower extremity venous. The RULA scores for each of the examinations fell between 3.11 and 5.00, indicating that the positions used for these examinations may be harmful and further investigation is warranted. The authors investigated the two highest scoring scans further—the upper extremity venous and transvaginal pelvic examinations, each receiving a RULA score of 5. While performing the upper extremity venous duplex scan, the sonographer was usually positioned on the right side of the patient. The sonographer would then need to reach across the patient to scan the left upper extremity, placing the sonographer’s arm in a large abduction angle while bending at the trunk and neck. While performing a transvaginal scan, a long transducer needs to be inserted and maneuvered at various angles to obtain all the images. This necessitates the sonographer repetitively bending the wrist into extreme angles.
Another study by Village and Trask 24 quantified the postural and muscular loads during arm abduction, shoulder external rotation, neck rotation, and unsupported shoulder postures as well as the amount of force used while holding the transducer. Their results determined that, on average, sonographers spent 68% of their time with arm abduction greater than 30 degrees, 63% of the time with shoulder external rotation greater than 30 degrees, and 37% of the time with the neck rotated greater than 20 degrees. These measurements demonstrate that sonographers spend a great amount of time in static, unsupported, and non-neutral positions. Furthermore, the sonographers in the study held the transducer with an average grip force of 4 kg, with peak forces measuring around 27.6 kg. Prior studies have shown that pinch grips (where the finger and thumb are pressing together) greater than 0.9 kg and gross grasp (fist motion) greater than 4.5 kg are risk factors for developing musculoskeletal injury at the hand and wrist. This study concluded that the risk factors are consistent with the demand on neck and upper extremity muscles, which is common with WRMDs, and symptoms reported by many sonographers in studies conducted in both the United States and Canada.
Ergonomic Scanning Techniques
To date, there has been only one research study that proposed scan-specific and detailed practice guidelines for the prevention of musculoskeletal disorders for radiologic professionals. The authors proposed rules for best practice, which illustrated recommended positions and those to avoid. Ergonomic techniques and postures were described only for abdominal sonographic scans and transvaginal sonographic scans. 25
For abdominal scans, it was recommended that sonographers (a) keep their neck straight by positioning their head directly in front of the monitor, (b) do not pass the probe cable around the back of the neck, (c) use a chair with adjustable height, (d) keep the lower back firmly supported on the chair’s backrest, (e) keep the trunk straight in line with the axis of the screen, (f) position the patient as close as possible to the operator, (g) place the scanning arm on top of the patient, (h) hold the transducer with a palmar grip, (i) keep the wrist in a neutral position, and (j) keep the hips, knees, and ankles at a 90 degree angle.
For transvaginal scans, it was recommended that sonographers (a) sit between the legs of the patient, (b) move the control panel down to the patient’s feet if possible, (c) position the screen over the patient, and (d) keep the elbow angled at 90 degrees.
General Recommendations for Workplace Improvements
Several studies have investigated the work practices of individual sonographers and sonography departments as a whole in order to create general recommendations for workplace improvements and to develop preventive strategies that can be used to address the high prevalence of WRMSDs. Muir et al 7 recommended that worksites should have access to a principal treatment provider (PTP)—a health care professional who is knowledgeable about musculoskeletal injury, understands radiologic work demands, is able to identify unsafe scanning techniques, and can recommend safe scanning techniques. The PTP should regularly assess work sites, perhaps as frequently as once or twice a month, to identify safe and unsafe work practices and to reinforce previously learned material. It was further recommended that diagnostic medical sonographers receive educational workshops that provide information about musculoskeletal injuries, physical fitness programs, general safe scanning techniques, and scan-specific techniques.
Gibbs and Edwards 26 have reported a study that identified 22 sonographers who were actively practicing sonography without experiencing symptoms of musculoskeletal discomfort. Their findings indicated that participating sonographers believed that they avoided WRMSDs as a result of postural adjustments, with no special equipment used. Participants rated job satisfaction and general happiness as high. Several participants emphasized that they must be aware of potential problems, take actions to solve problems, and take frequent breaks. From this information, the authors concluded that the development and avoidance of musculoskeletal injury are multifaceted. The most important theme revealed by the data was that sonographers should take responsibility for their practice and perform scans while maintaining constant awareness of the position and technique they are using.
A second study by Gibbs and Young 27 described the immediate and long-term benefits that took place after sonographers received education about methods to reduce WRMSDs. The education included participants attending a workshop where they acquire knowledge about specific methods they could use in the performance of scans while using the principles of ergonomics and a progressive musculoskeletal relaxation technique. The participants then responded to surveys immediately after the completion of the workshop and again after 10 weeks. Common remarks immediately after the workshop indicated that participants felt the educational opportunity to be helpful, they believed that they would be able to apply what they learned to practice, and they were aware of the changes made to their scanning position after instruction about ergonomics. Common remarks after the 10-week follow-up included that they felt they had an increased awareness about the potential problems and importance of taking preventive action, and they also felt that they needed reinforcement about the principles they had learned. After the data were collected and analyzed, the researchers determined that the workshop in ergonomics and the relaxation technique was a success due to the fact that the majority of participants had adapted the principles they had learned into their work practices. The researchers concluded that sonographers could benefit from receiving education on ergonomics and the Alexander relaxation technique because this education could play a significant role in the attempt to decrease WRMSDs.
Euler and Meadows 28 described the positive changes that took place after diagnostic medical sonographers implemented ergonomic guidelines into their scanning techniques over a 10-year period. The researchers obtained data on the incidence, treatment cost, and lost work time due to musculoskeletal injury before and after they incorporated ergonomic techniques into their practice. It was determined that before ergonomic interventions were adapted, injuries resulted in $22 000 of treatment costs and 191 hours of lost work time. After the department implemented ergonomic interventions, the cost of treatment for musculoskeletal injuries significantly decreased, the amount of work hours lost due to WRMSD significantly decreased, and the department experienced a decreased rate of injury reports. The authors concluded that implementing ergonomic guidelines eliminated sonographer musculoskeletal injury while decreasing organizational cost and lost productive hours.
Multimedia in Education
As of the last census in 2011, 71.7% of American households reported accessing the Internet in the home. 29 Use of the Internet as a tool to provide multimedia education has been a feasible method for individuals to access material at their own leisure. In addition, multimedia used in education has been shown to have statistically significant improvement in retention when information is organized by facts that are connected by underlying relationships.30–34 The ability to make these connections can facilitate greater ability to make correct inferences about new situations that may arise. It has also been shown that audio narration, video clips, interactive models, and animations facilitated higher knowledge and satisfaction for students. 34
Because of the high prevalence of musculoskeletal disorders, this research project was primarily developed to provide practicing radiologic professionals an educational multimedia tutorial on proper ergonomic scanning procedures, as well as to help identify a strategy to help learn ergonomic procedures that these health care workers may be able to implement in their current practice. Multimedia in this context is defined as using computers to present text, graphics, video, animation, and sound in an integrated way. 35
For the purpose of this research, an educational multimedia tutorial was created and incorporated both static pictures and narrated scenarios designed to educate radiologic professionals on risk factors and preventive techniques for WRMSDs. In addition to the multimedia educational tutorial, a pretest questionnaire and posttest questionnaire were designed to answer the following research questions: (1) To what extent are radiologic professionals aware of the physical risk factors that contribute to work-related musculoskeletal disorder? (2) To what extent are radiologic professionals aware of strategies to prevent WRMSDs? and (3) After receiving a multimedia tutorial on reducing the physical risk factors of WRMSDs, do radiologic professionals change their work behaviors to incorporate the strategies?
Once identifying whether radiologic professionals’ knowledge and work practices reliably changed after being exposed to an educational multimedia tutorial, the goal was to determine if educating these same participants about proper ergonomic scanning procedures is an effective method to decrease the prevalence of WRMDs. The ultimate goal of an effective intervention is to decrease career-ending injuries through decreased symptomology. This in turn may lead to an increased efficiency in the workplace and career longevity, as well as to a decrease in financial resources that employers must allocate to factors such as absenteeism and workers’ compensation.
Methods
Research Design
The research team developed a pretest and posttest to gather baseline data on participants, including demographic information, years working in the field, level of pain, practice patterns, and knowledge of what causes musculoskeletal pain. After completing the pretest, the participants automatically were redirected to a multimedia presentation concerning common musculoskeletal injuries among radiologic professionals and important information on preventing WRMSDs.
A posttest was administered to determine whether the radiologic professionals retained knowledge of proper work safety habits and ergonomics as described in the multimedia tutorial. The pretest and posttest were piloted with individuals who would not be participating in the study. The study, including these instruments, was approved prior to initiation by the local institutional review board (IRB); the IRB waived the informed consent requirement due to the minimal risk involved in the study. The pretest and posttest were made available via secure, private web links through Survey Monkey. Two co-investigators had access to the survey and response data. The multimedia tutorial, via automatic redirect to a private, secure YouTube video, was made available to those who had completed the pretest. Only one investigator had access to post, edit, and/or remove the tutorial.
Study Participants
The supervisors of radiography and sonography departments from two acute care hospitals and the faculty of an academic sonography program were approached to assist in recruiting study participants. The inclusionary criteria were radiographic professionals who are engaged with repetitive job tasks, awkward postures, and mechanical stress on upper extremities, with sonographers being the focus. Students of radiography and sonography and minors were excluded from participating in this study. For recruitment, potential participants were sent the research project information statement via an email attachment.
The survey included a demographic section to gather information on gender, years of professional experience, and age. A Likert-type visual analog scale question regarding the level of pain that the participant experienced during work-related activities was also included. Participants were asked to complete a short answer question regarding common musculoskeletal injuries among radiologic professionals. The final short answer question related to which work practices increase the likelihood of WRMSDs. After completing the pretest, participants viewed an approximate 10-minute multimedia tutorial at a secure site at www.youtube.com. This tutorial was created by occupational therapy graduate students and piloted, along with the pretest and posttest, by other graduate students to ensure ease of access across a variety of platforms (e.g., personal computer and various mobile electronic devices).
Four to 6 weeks after completing the pretest and viewing the multimedia presentation, participants were provided with an email link to the posttest and given 2 weeks to complete the test. The posttest was identical to the pretest with the addition of questions about whether participants have changed work practices after viewing the tutorial. Data collection occurred over a 6-week period during October and November 2013. To promote participant confidentiality and anonymity, participant names were not on the survey but were coded numerically. Embedded YouTube analytics were used to verify that the tutorial was viewed at least once after each completed pretest.
Results
Demographics
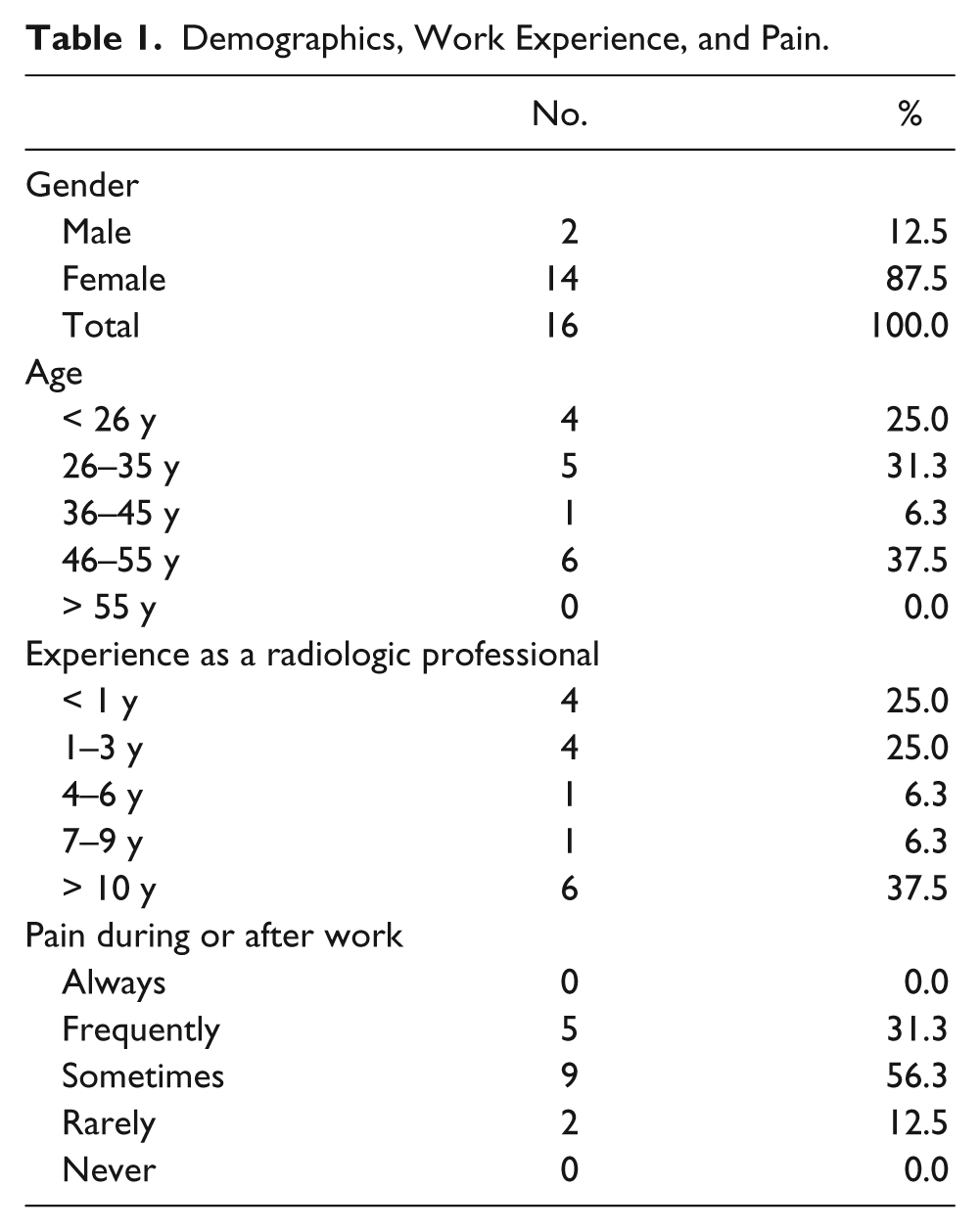
There was a potential of 25 radiologic professionals from the Sidney and Lois Eskenazi Hospital (formerly Wishard Hospital) and Indiana University School of Medicine (IUSOM) Division of Sonography who could have participated in the study. All were invited to participate, and 16 chose to participate in this study (64%). Fourteen (87.5%) of the participants were female and 2 (12.5%) were male. At the time of the posttest completion, 4 (25%) of the participants were age 25 years or younger, 5 (31.3%) were between the ages of 26 and 35 years, 1 (6.3%) was between 36 and 45 years old, and the remaining 6 (37.5%) were between the ages of 46 and 55 years (Table 1).
Demographics, Work Experience, and Pain.
Work Characteristics
Four (25%) study participants had less than 1 year of experience as a radiologic professional, four (25%) had 1 to 3 years of experience, one (6.3%) had 4 to 6 years of experience, one (6.3%) had 7 to 9 years of experience, and six (37.5%) had more than 10 years of experience. When asked how often they experienced pain during or after the work day, zero participants responded, “always,” five (31.3%) responded, “frequently,” nine (56.3%) responded, “sometimes,” two (12.5%) responded, “rarely,” and zero responded, “never” (Table 1).
Awareness and Prevention of WRMSD
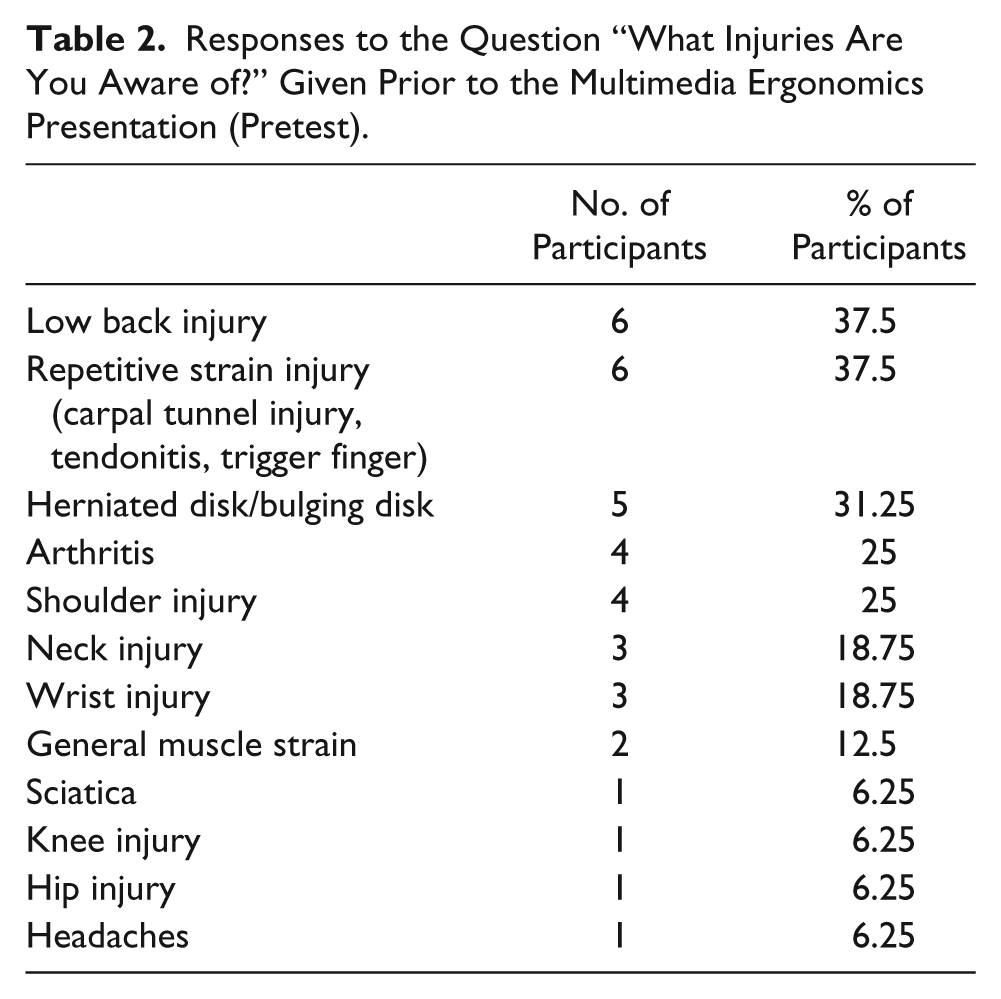
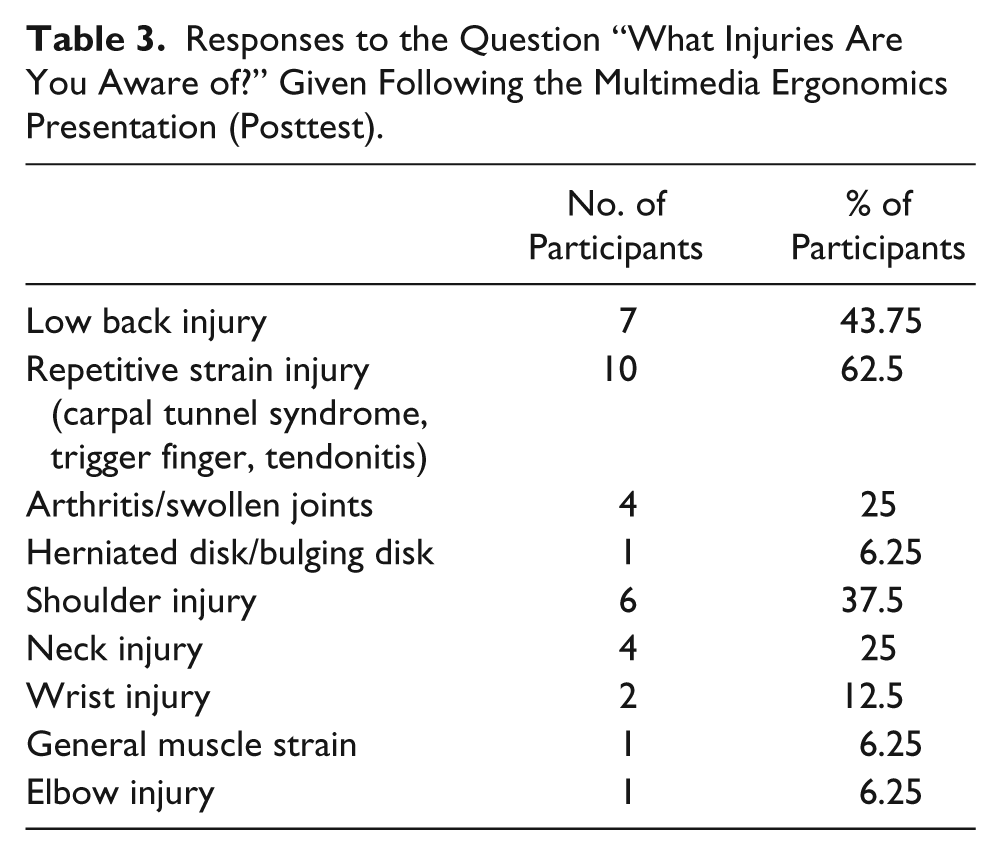
All 16 study participants completed the pretest and posttest; 15 (93.7%) answered, “yes,” when asked if they were aware of common musculoskeletal disorders that can occur among radiologic professionals, and one (6.3%) answered, “no.” Participants were also given an open-ended question within the survey tool asking them to “name the injuries that may occur due to improper body mechanics or work practices.” The answers were placed into 12 categories in the pretest: lower back injury, repetitive strain injury, herniated disk, arthritis, shoulder injury, neck injury, wrist injury, general muscle strain, sciatica, knee injury, hip injury, and headaches (Table 2). The answers on the posttest were placed into 9 categories: low back injury, repetitive strain injury, herniated disk, arthritis, shoulder injury, neck injury, wrist injury, elbow injury, and general muscle strain. Some of the participants listed one injury, whereas others listed several (Table 3).
Responses to the Question “What Injuries Are You Aware of?” Given Prior to the Multimedia Ergonomics Presentation (Pretest).
Responses to the Question “What Injuries Are You Aware of?” Given Following the Multimedia Ergonomics Presentation (Posttest).
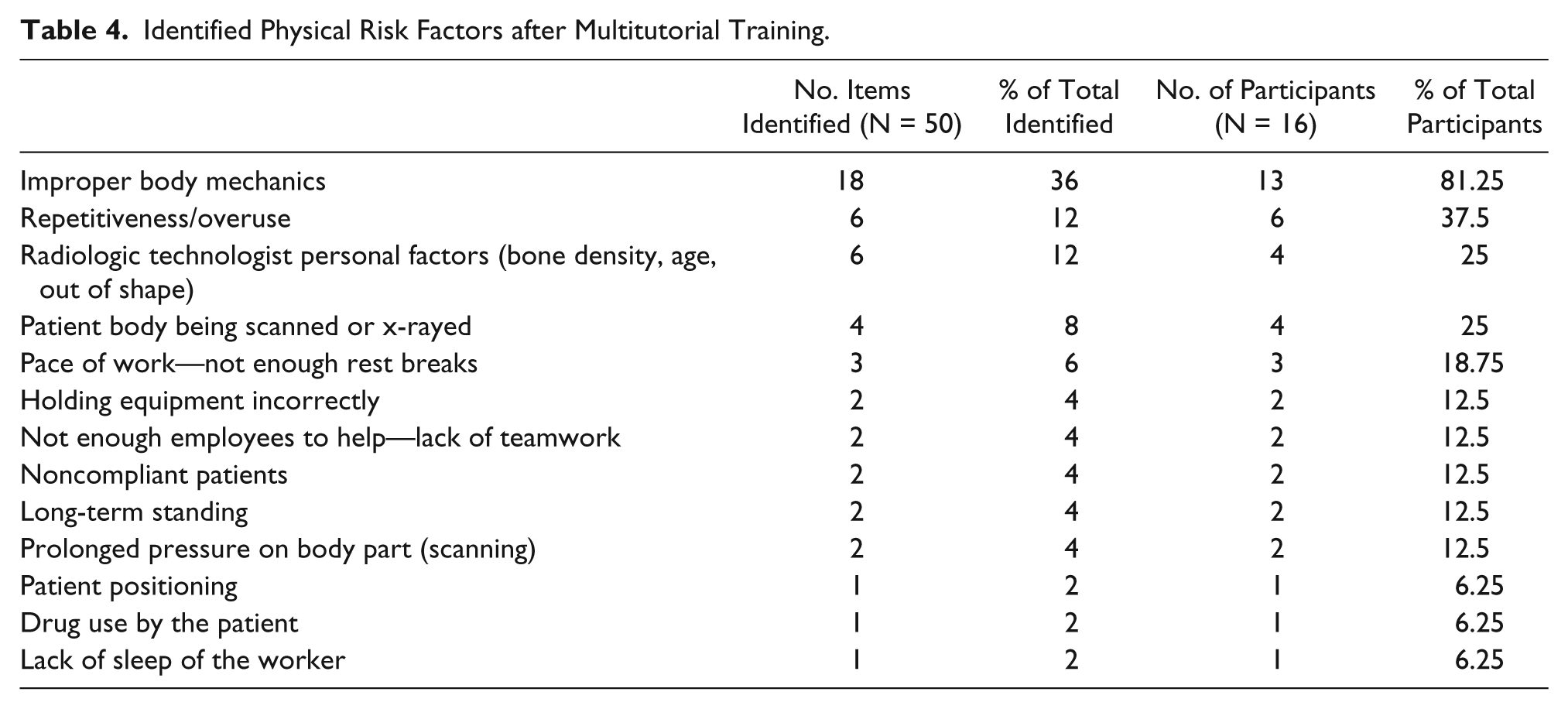
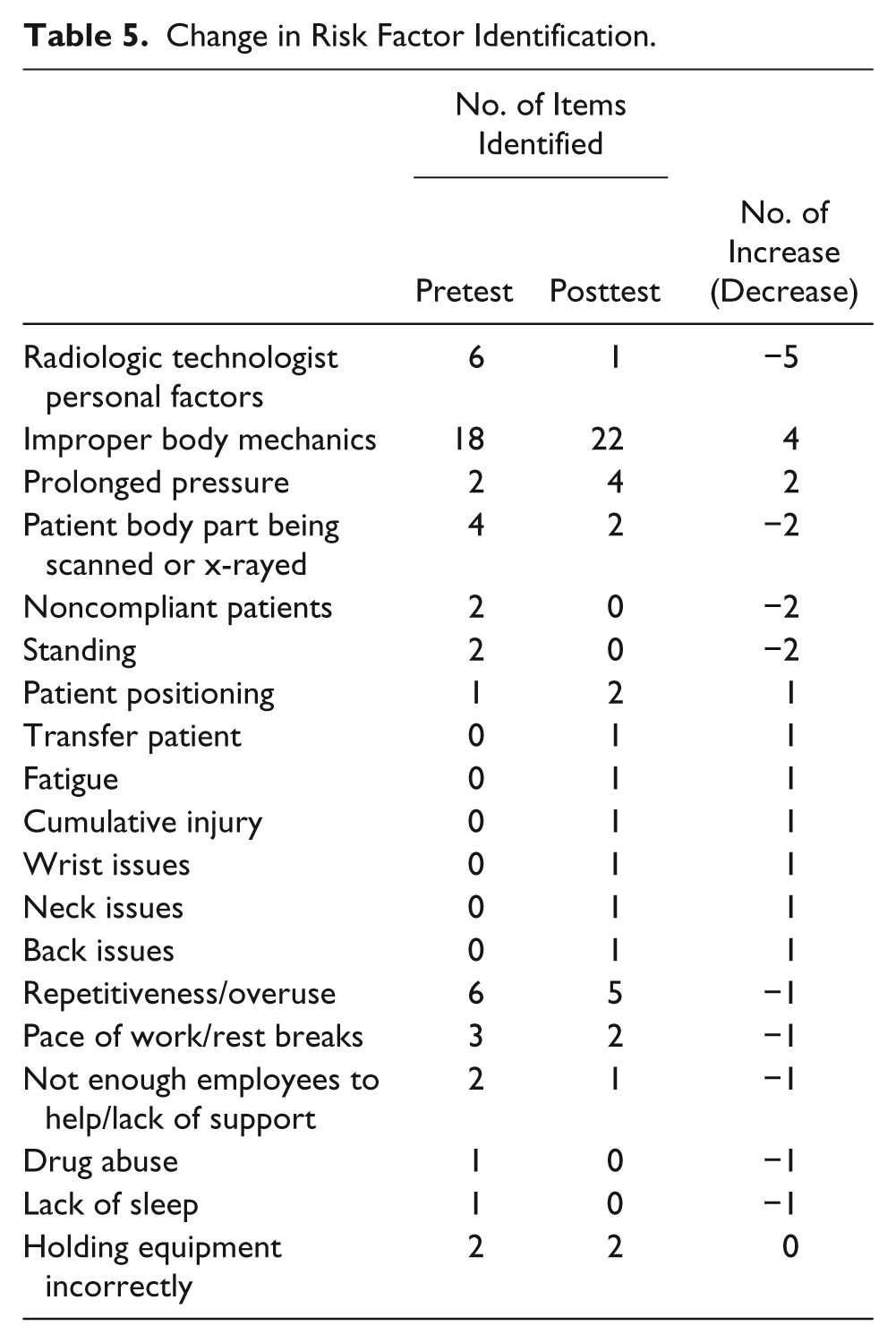
On the posttest survey, item 6 asked participants to identify three physical risk factors contributing to WRMDs. Thirteen common themes were identified by the participants (Table 4). Table 5 shows the numerical change in the number of times WRMSD risk factor themes were identified from pretest to posttest, with improper body mechanics—a major content theme of the web-based tutorial—showing the most increase in identification on the posttest.
Identified Physical Risk Factors after Multitutorial Training.
Change in Risk Factor Identification.
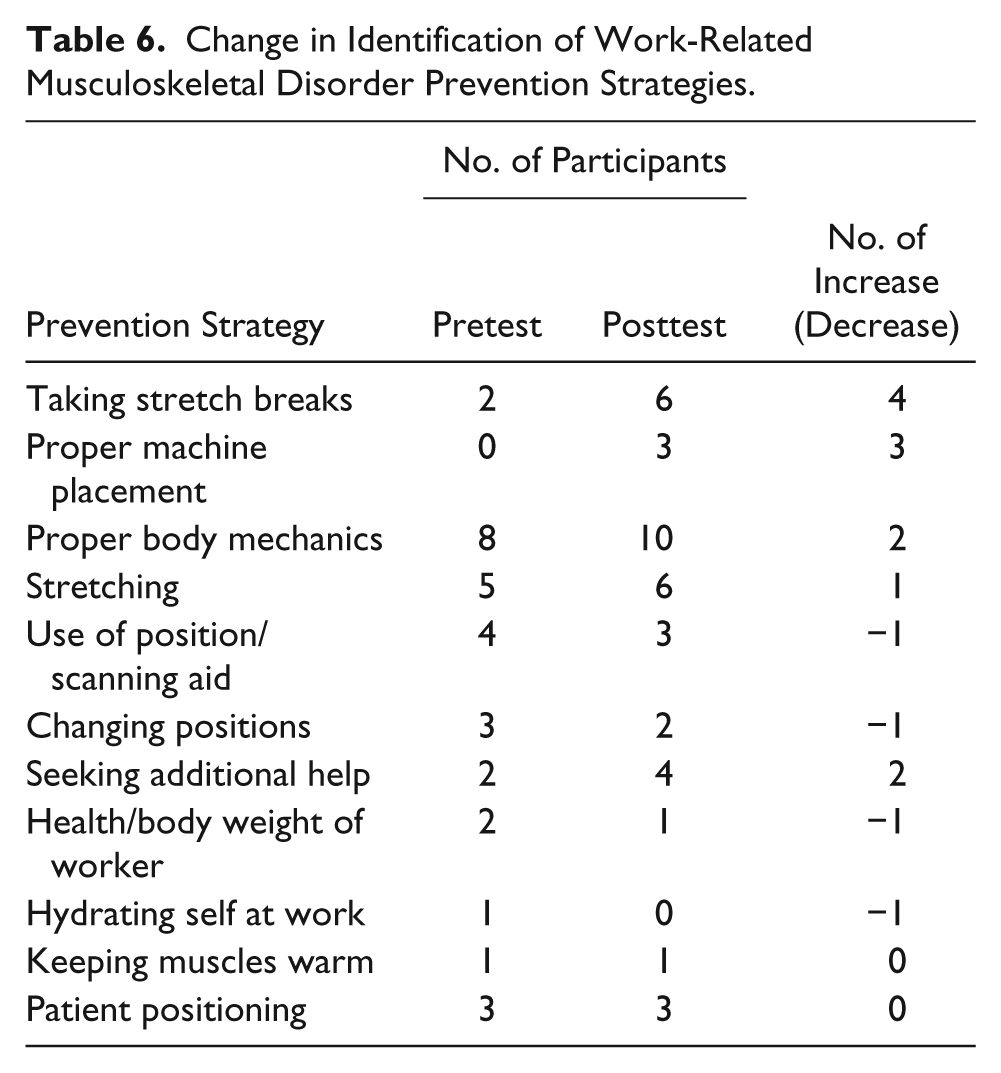
Approximately 94% of all participants shared that they were now aware of the influence of WRMDs and methods of prevention. One participant reported not being aware. Item 7 on both the pretest survey and the posttest survey asked for the strategies that radiologic professionals could take in the workplace to reduce the risk for musculoskeletal disorders. Table 6 shows the change in identifying prevention strategies after the training. Taking stretch breaks and proper machine placement were identified three times more frequently in the posttest than in the pretest.
Change in Identification of Work-Related Musculoskeletal Disorder Prevention Strategies.
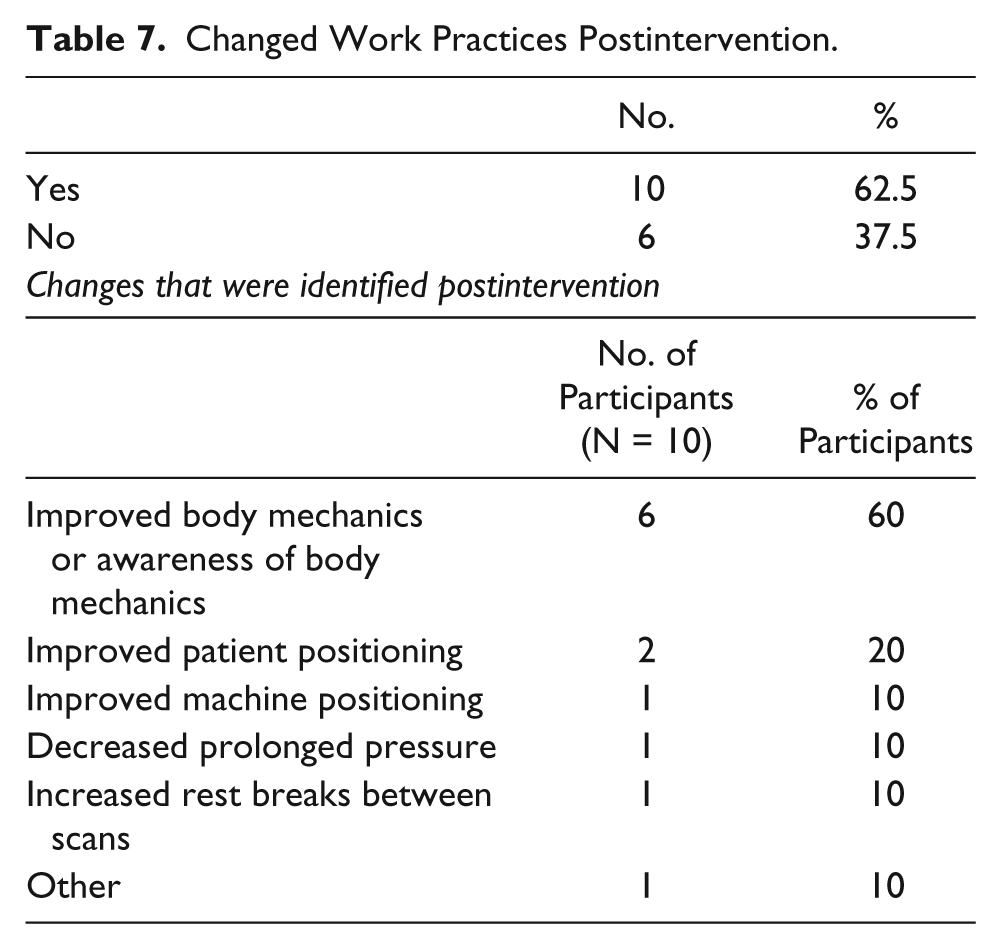
When asked on the posttest whether they changed their work practices, 10 (62.5%) of the 16 radiologic professionals who participated in this study responded, “yes,” and 6 (37.5%) responded, “no” (Table 7). Of the 10 radiologic professionals who answered, “yes,” when asked if they had changed any of their work practices since viewing the online ergonomics tutorial, 6 (60%) reported improved proper body mechanics or awareness of body mechanics, 2 (20%) reported improved patient positioning, 1 (10%) reported improved machine positioning, 1 (10%) reported decreased prolonged pressure, 1 (10%) reported increased rest breaks between scans, and 1 response (10%) fell into the “other” category. Those who did not change their work practices did not indicate why they did not change. Of note, 55% of the sonographers in this study had not received any formal ergonomic training until this study. That fact, coupled with the findings from this study, has led to a conclusion that this widespread problem in the radiography/sonography profession requires significant further attention.
Changed Work Practices Postintervention.
Discussion
This study was designed to determine if viewing a multimedia presentation would change radiologic professionals’ knowledge and/or work practices in response to safe scanning techniques, with hopes of reducing the incidence and prevalence of musculoskeletal injury. The research questions were evaluated by analyzing participant data collected in the pretest survey, intervention, and posttest survey, which included demographics, work experience, pain levels, and a change in knowledge of safe work practices.
The majority (87.5%) of the study participants reported that they experienced musculoskeletal pain either “frequently” or “sometimes” during or after their workday while practicing as a radiologic professional/sonographer. This figure is consistent with the results of comparable studies that have determined that approximately 80% to 90% of radiologic professionals are experiencing pain while at work or at home.1,2,5–7,12,15,36 Furthermore, 100% of the study participants reported experiencing musculoskeletal pain during or after their workday at some point in their careers. This may suggest that the study participants’ pain could possibly be caused by their work practices and assuming improper ergonomic positions.
The results of the first survey indicated that participants were already aware of basic physical risk factors that can contribute to the development and exacerbation of musculoskeletal injury. These results were not surprising due to the fact that specific physical risk factors have been extensively described and detailed for the past decade. Although it is important to provide radiologic professionals with reminders of the physical risk factors, this has not been enough. Organizations might want to consider providing training in proper body mechanics on an annual or other recurring basis, emphasizing the ergonomic strategies and in some fashion demonstrating these strategies. After the participants viewed the multimedia tutorial and completed the posttest, their responses changed to include injuries that were discussed in the multimedia tutorial and exclude injuries that were not discussed, indicating that learning had occurred. These results show that providing radiologic professionals with a multimedia presentation as a method of education can increase knowledge and awareness about the types of injuries that can occur within the profession.
The results of the initial survey indicated that the vast majority of participants (93.7%) stated that they were already aware of a wide variety of general ergonomic techniques they could incorporate into practice to remain safe from injury. After participants viewed the multimedia tutorial and were again asked about ergonomic techniques, they were more likely to include specific safe scanning techniques addressed in the tutorial and not always including some of the strategies they identified on the pre-test. From these results, it can be concluded that the multimedia tutorial did have an effect on the radiologic professional’s knowledge and awareness about specific types of ergonomic scanning techniques. Furthermore, after the participants viewed the multimedia tutorial, the majority (62.5%) reported that they did change their work practice to incorporate more ergonomic scanning strategies. Specific changes to work practices that were reported included improved body mechanics, improved patient positioning, improved machine positioning, decreased prolonged pressure, and increased rest breaks between scans. That these changes took place after viewing the multimedia tutorial implies that there is room for radiologic professionals, especially sonographers, to increase their awareness of scan-specific ergonomic techniques as well as the frequency with which they put these techniques into practice. It is plausible that radiologic professionals have room to improve their awareness and practice, because guidelines for the proper performance of these scans were only recently created. Therefore, providing education about scan-specific ergonomic techniques could be one method used to facilitate the decrease in incidence and prevalence of musculoskeletal injury.
Practice, Education, and Research Implications
The results indicate that a multimedia presentation on safe ergonomic principles while performing radiologic examinations with a transducer does bring about positive short-term benefits to radiologic professionals’ work practices. Using this type of educational multimedia presentation allows for learning by the radiologic professionals at a time and/or place most convenient for the practitioners. They are able to quickly access the current knowledge of the material available in the literature. The practitioner is able to view the presentation repeatedly and can also pause the presentation to view a scanning technique for a longer period of time to facilitate learning.
Given the inherent physical risk factors that many radiologic professionals face because of the nature of their job tasks, consistent and intermittent reminders about basic safety principles are important.26–28 Previous research studies on this subject have recommended that radiologic professionals receive a workshop or training session approximately every 6 months in hopes of reinforcing safe scanning techniques and positions. Allowing participants to view a multimedia tutorial that includes pictures and explanations of safe scanning practices at a minimum of 4- to 6-month intervals would likely be beneficial. The results of this research study showed that the majority of radiologic professionals improved their awareness and practice of safe scanning practices after viewing the multimedia tutorial, and regular reinforcement of these principles would likely enhance the long-term benefits.
Study Strengths
The majority of prior research studies have only identified and described which scanning techniques contribute to the development of musculoskeletal injury, yet they have not proposed specific solutions to the problem. Three research studies have explained specific ergonomic scanning techniques that radiologic professionals can use in their daily practice to remain safe from injury.16,18,25 Research studies that have proposed a means to help educate radiologic professionals about safe and ergonomic work practices primarily included providing an experiential workshop led by a knowledgeable clinician. 27 However, the experiential workshops used, although shown to be beneficial, carry the drawback that the participant is not able to revisit, review, or re-experience the majority of the materials encountered. This study is the first to propose using a multimedia tutorial accessed via the Internet as a means to educate radiologic professionals about ergonomic work practices. That 64% of all possible subjects participated indicates that this technique draws a good response.
Study Limitations
The present study does have some limitations. There has not been a study establishing the reliability or validity of a survey concerning ergonomic scanning strategies of radiologic professionals. As a result, the research team created and used a survey that did not have established reliability or validity. The survey was distributed to a small convenience sample of 25 radiologic professionals currently employed at hospitals located in a single center, and with only 16 participants, the results do not have statistical significance and are not generalizable. The study participants viewed the multimedia presentation and were then given a 6-week period to adjust their scanning practices as they deemed necessary and appropriate before they completed the postintervention survey. However, there was no follow-up at an interval such as 3 to 6 months after the study to determine long-term retention of learning.
Future Research
The multimedia tutorial that this research group presented to the radiologic professionals included ergonomic scanning techniques specific to two types of sonographic examinations—the transabdominal scan and the transvaginal pelvic scan. This was because ergonomic guidelines have been proposed for only these two common types of scans, although there are many other types of scans that sonographers are likely to encounter on a daily basis. Ergonomic guidelines while performing these other scans have not been established, so they were therefore not included in the multimedia tutorial. It is recommended that future studies investigate and outline possible ergonomic scanning techniques and principles for a broader spectrum of sonography specialties. This future research could be a comprehensive and standardized set of guidelines that would benefit the profession, describing how these professionals can perform scans in a safe and ergonomic manner. This work of scan-specific ergonomic instructions could then be presented in a comprehensive multimedia tutorial accessed via the Internet by multiple radiologic professionals. A future study with a larger number of participants from multiple institutions would increase the generalizability of the data.
In an attempt to protect the anonymity of the participants, individual changes from preintervention survey to postintervention survey were not tracked. Data were analyzed in aggregate form to assess prevailing trends from the entire group. In future studies, it may benefit researchers to individually track participant answers to determine individual changes and to provide information on how the multimedia tutorial specifically affected individuals. Although self-reported surveys are a low-cost, fast, and convenient way to collect data, they have limitations. It would be ideal to conduct a study in which the participants were video monitored during their workday for a specified period of time after having received an intervention of multimedia training on safe body mechanics. This video could be viewed and assessed by a blinded occupational therapist with expertise in ergonomics. This would provide an objective outcome to determine if their work practices improved after the intervention of multimedia training on proper body mechanics instead of self-reporting. This study was based solely on self-reporting in improved workplace practices; having a third party evaluate proper ergonomic postures would be a valuable way to determine the effect of multimedia presentations and their actual influence.32–34
Conclusion
This study suggested that providing radiologic professionals with a multimedia tutorial on ergonomics may result in an increase in the incorporation of safe scanning techniques into actual practice. Because of the high rate of musculoskeletal injury among radiologic professionals, it is paramount that practitioners and supervisors alike take the initiative to educate themselves about physical risk factors that contribute to injury. Ergonomic solutions can then be incorporated into practice in an attempt to decrease the incidence and prevalence of injury and pain. Viewing a multimedia ergonomics tutorial on low- and high-risk scan-specific practices is one such method that has the potential to be easily used by practitioners on a large scale.
Footnotes
Acknowledgements
The author would like to acknowledge the contributions of his co-investigator on this study, Susan Hardesty, MS, OTR, Senior Occupational Therapist and Ergonomic Specialist at Eskenazi Health, as well as Brian Eddy, MS, OTR, Samantha Kolakowski, MS, OTR, Mathew O’Connor, MS, OTR and David Proctor III, MS, OTR, all graduate students in the Master of Science in Occupational Therapy Program at Indiana University at the time this research was done.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.