
Abstract
Thymus tumors are rare primary neuroendocrine tumors that develop near the mediastinum. These tumors often have no known etiology but can arise from ectopic tissues in the mediastinum or occur within the thymus. This case study presents a rare finding of a 9-cm × 8-cm squamous cell carcinoma tumor arising from the thymus within the anterior mediastinum. The patient’s symptoms included congestion, coughing, and chest pain. The mass was initially found on a chest radiograph. Results of the echocardiogram showed that the tumor was impinging on the right ventricular outflow tract and the pulmonary artery of the heart.
Thymomas and thymic carcinomas are tumors that start from thymic epithelial cells, which give the thymus its structure and shape, and they develop near the mediastinum. 1 These tumors often have no known etiology but can arise from ectopic tissues in the mediastinum or occur within the thymus. Thymic carcinomas usually occur in people between the ages of 40 and 80. Thymic carcinomas are rare, with an annual incidence of approximately only 500 people in the United States diagnosed each year, accounting for about 0.2% to 1.5% of all cancers. 2 Many patients will be asymptomatic at the time of diagnosis. Some typical symptoms include coughing, chest pain, upper airway congestion, muscle weakness, fatigue, shortness of breath, arm or facial swelling, difficulty swallowing, anemia, and an increased risk of infection.
The focus of this case study is to present a rare finding of a thymic carcinoma that is impinging on cardiac structures—namely, the right ventricular outflow tract and the main pulmonary artery. Echocardiographic 2D, color, and Doppler analysis confirmed as well as defined this unique situation. This case study elucidates the importance of the sonographer’s critical thinking skills in being able to recognize extracardiac pathological entities that may affect cardiac function.
Case Report
This patient is an African American man (age, 53 years; height, 6′2′′; weight, 209 lbs) complaining of recent chest pain and dyspnea. He has a history of a heart murmur and systemic hypertension. The chest radiograph showed a mass near his heart, measuring 9 × 8 cm, and was located near the aorta and pulmonary artery. Associated laboratory findings are as follows: white blood cells (WBC), 31.8; hemoglobin (HGB), 8.2; hematocrit (HCT), 26.3; sodium (Na), 132; potassium (K), 4.4; platelets (PLT), 359; blood urea nitrogen (BUN), 23; creatinine, .93; and glucose, 115. The following laboratory values were abnormal findings: WBC, HBG, HCT, NA, and PLT.
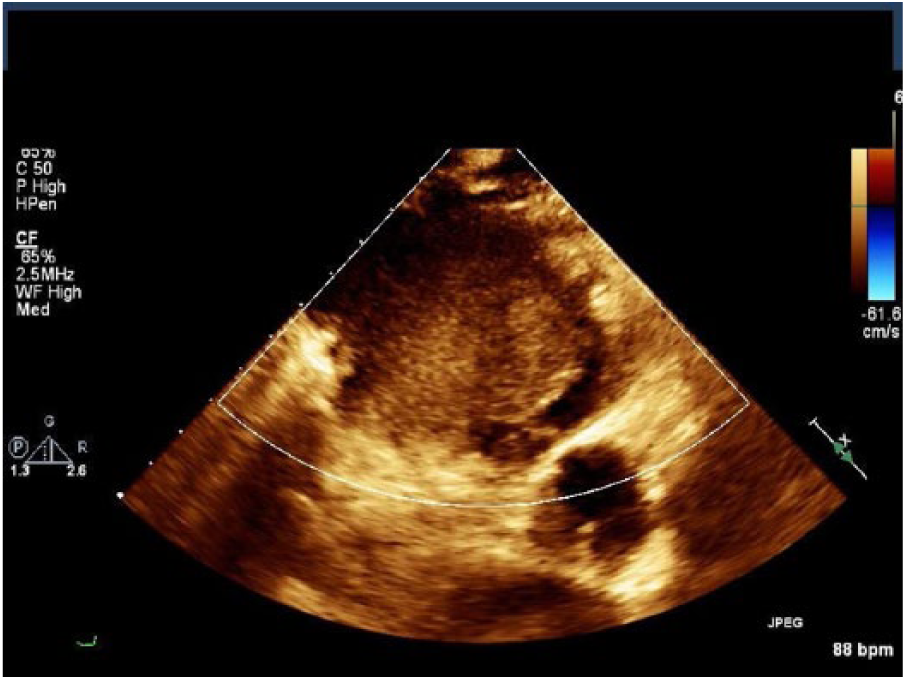
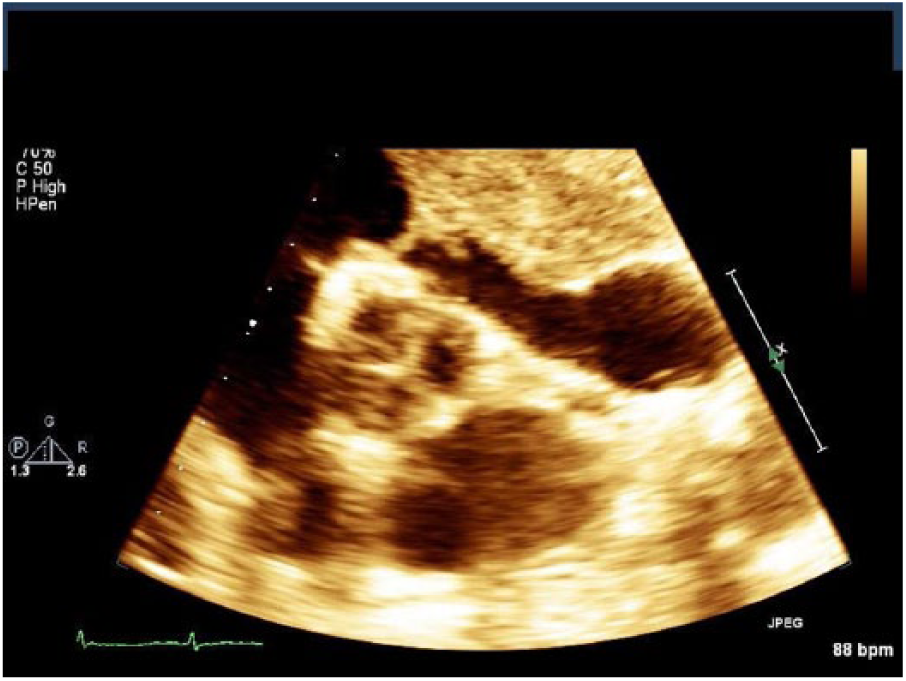
After finding the mass initially on a chest radiograph, the patient was sent to the echocardiography laboratory for further examination. With echocardiographic imaging, a 9-cm × 8-cm solid mediastinal mass was found that was impinging on the right ventricular outflow tract and the pulmonary artery (Figures 1-6). The mass was hypovascular and homogeneous throughout, seen in the parasternal short-axis view only. Color flow Doppler of the blood flow in the main pulmonary artery indicated aliased high velocities (Figure 6). Peak pulsed wave spectral Doppler velocity of blood flow measured a Vmax of 108 cm/s in the right ventricular outflow tract (RVOT) and approaching 240 cm/s in the left pulmonary artery. Continuous wave Doppler of tricuspid regurgitation indicated a Vmax of 262 cm/s. It was obvious through 2D analysis that the tumor’s size was large enough to impinge on the right side of the heart at the level of the pulmonic valve. The histopathological examination of the specimens from the patient resulted in a diagnosis of a squamous cell carcinoma of the thymus, an epithelial tumor of the thymus.
Mass seen in the parasternal short-axis view near the mediastinum.
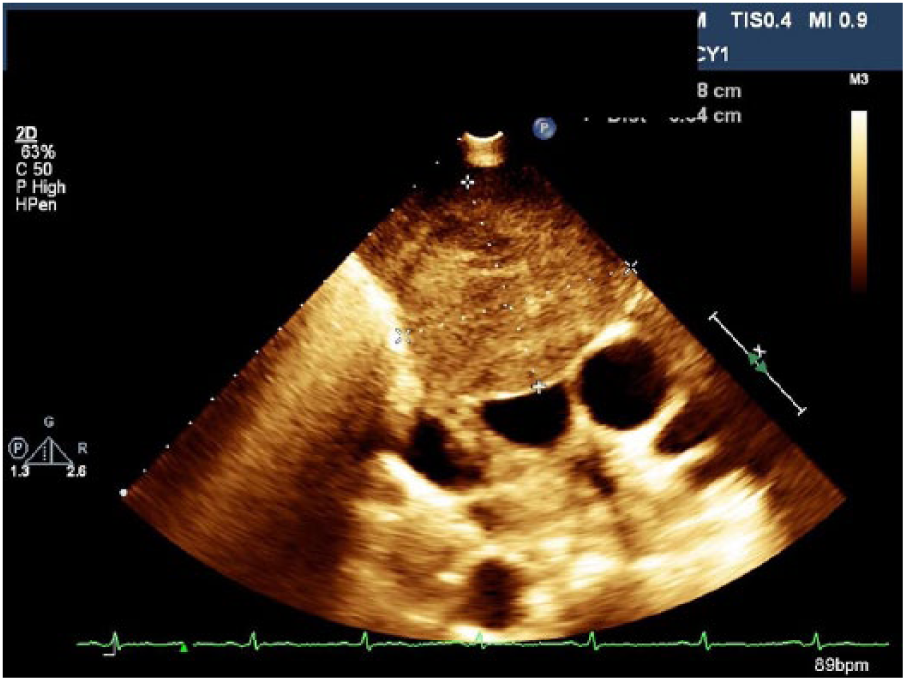
Widest point of the mass.
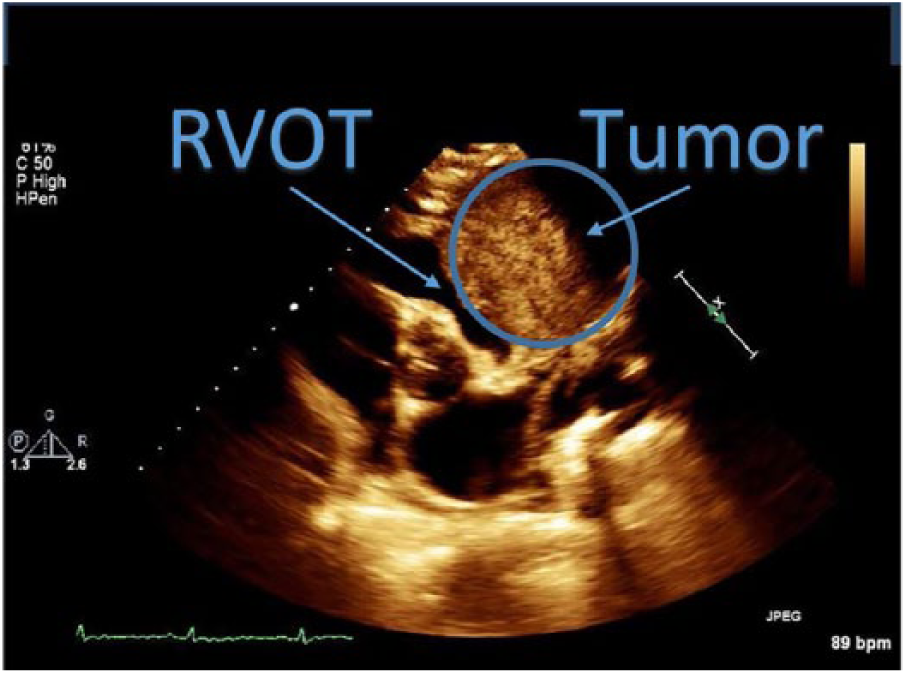
Parasternal short-axis view shows that the tumor is impinging on the right ventricular outflow tract and pulmonary artery.
Parasternal short axis view of the mass at the aortic level, impinging on the right ventricular outflow tract.
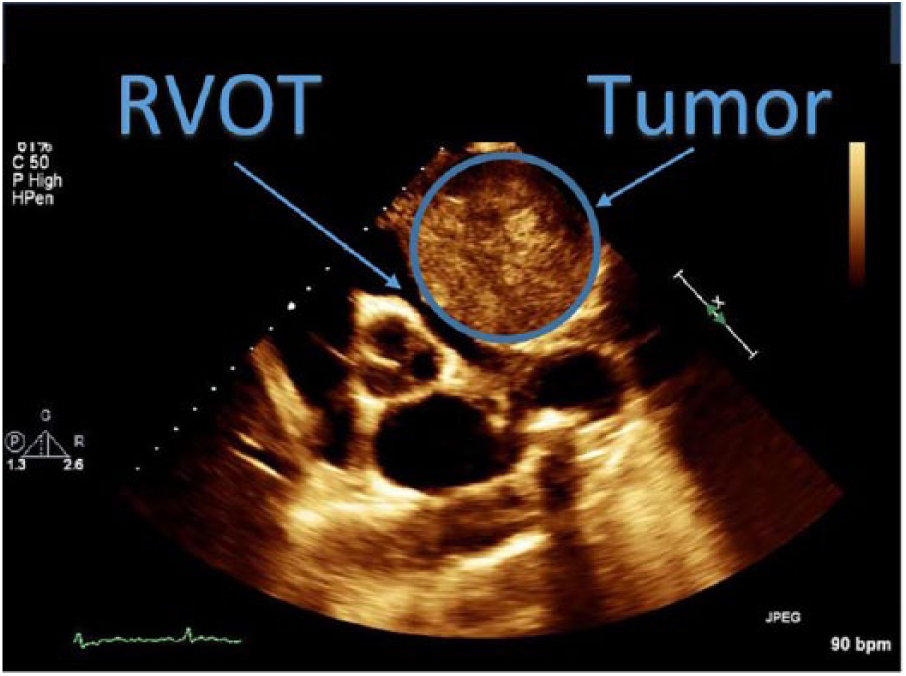
Zoom of parasternal short axis view showing the mass impingement of the right ventricular outflow tract.
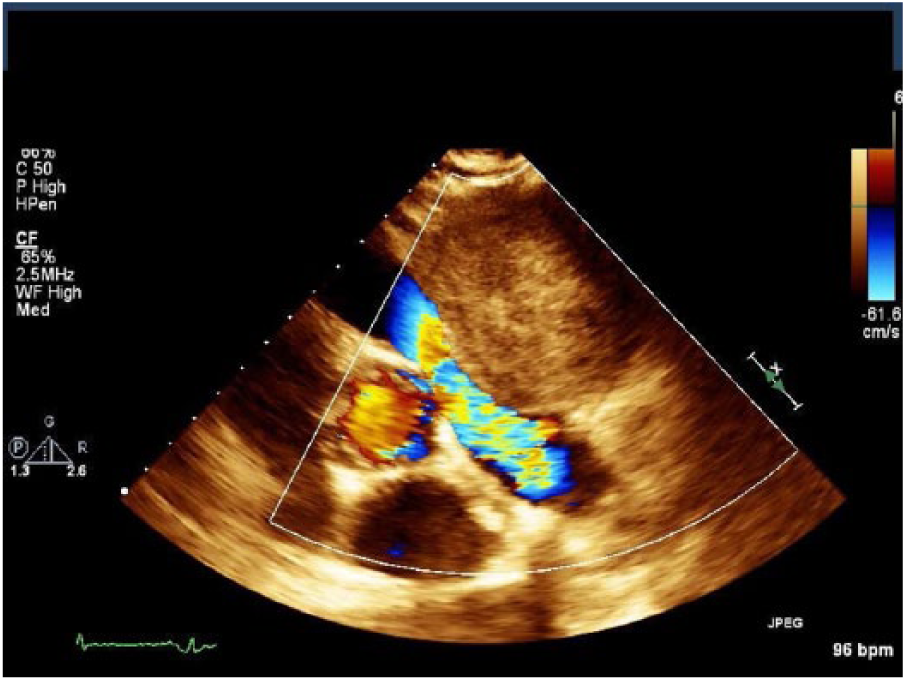
Color flow Doppler of blood flow through the right ventricular outflow tract.
Discussion
The thymus is an important organ of the endocrine system that aids in the maturation of T lymphocyte cells in the immune system. It begins as a paired organ, originating from the third and fourth pharyngeal pouches. The thymic buds migrate down the neck along the trachea and into the mediastinum toward the pericardium, where it fuses. As the heart migrates into the thoracic cavity during embryonic development, the thymus moves along with it. The thymus resides anterior to the major vessels of the heart and in front and just above the heart and the aortic arch. Large in size in the infant, the gland matures in size and function around ages 10 to 12 years and atrophies greatly by adulthood. 3
While thymic carcinoids lack fibrous compartmentalization and cystic changes and are frequent findings in thymomas, they commonly exhibit irregular areas of necrosis or hemorrhage. Thymic carcinoids may also contain fine calcifications as part of the differential. According to Nasseri and Eftekhari, 1 their appearance on radiographs and computed tomography (CT) is nonspecific. A mediastinal mass may not be evident on CT, even in the presence of endocrine abnormalities. The thymus is typically very pliable and does not cause compression or displacement of the adjacent structures. This attribute can be an important part of a sonographic evaluation because cardiac rhythms and respiratory variations can affect the shape of the thymus. By contrast, solid tumors are less malleable or compressible, and they are more rigid. 1
Thymic carcinoma is difficult to diagnose, with thymoma being a differential in the diagnosis. 3 Ninety percent of tumors in the thymus are thymomas, with the remaining 10% being thymic carcinomas. Both are diseases that form cancer cells on the outside surface of the body of the thymus gland. Thymic carcinomas are different from thymomas, however, in that thymic carcinomas grow more quickly than thymomas and can metastasize aggressively throughout the body. Only about 5% of patients with invasive thymomas have distant metastases at diagnosis, whereas 50% to 65% of patients with thymic carcinomas have metastases at diagnosis. 1 Nasseri and Eftekhari 1 state that thymomas show morphologic and immunohistochemical features that are characteristic of thymic epithelial cells. In contrast, the epithelial cells of thymic carcinomas do not. Also, thymic carcinomas usually lack a well-defined capsule, whereas up to two-thirds of thymomas are encapsulated.
Shimosato et al. 4 was the first to report thymic carcinoma. Thymic carcinoma was originally thought to be a type C thymoma, but it has now been categorized into subtypes recognized by the World Health Organization. 5 Thymic carcinoma comes with a poor prognosis, with a five-year survival rate of 20% to 30% and a two-year survival rate of 50%. 6 Squamous cell carcinomas, however, have a more favorable prognosis than other types of thymic carcinomas. Patients are usually diagnosed in the latter stages of tumor progression due to the lack of symptoms caused before extension of the disease.
The World Health Organization has created a classification system for thymomas and thymic carcinomas. 5 The classification system is based on the histologic type. Histologic subtypes of thymic carcinoma include the following (combinations of the following types can occur): squamous cell (epidermoid) thymic carcinoma, lymphoepithelioma-like thymic carcinoma, sarcomatoid thymic carcinoma (carcinosarcoma), clear cell thymic carcinoma, mucoepidermoid thymic carcinoma papillary thymic adenocarcinoma, and undifferentiated thymic carcinoma.
Standard primary treatment for patients with these tumors is surgical resection with en bloc resection for invasive tumors. Radiation therapy, chemotherapy, and/or surgery are indicated depending upon stage. The prognosis depends on how well the thymic carcinoma can be resected and whether or not there is recurrence. Currently, optimal management of thymic carcinoma has yet to be well defined, owing to the small number of cases reported each year. The risk of second malignancies and recurrence of these tumors is high. Therefore, lifelong clinical management and follow-up are appropriate.3,5,6,7
Echocardiographic 2D and Doppler evaluation in this case helped to define how the tumor was impinging on the RVOT and pulmonic valvular apparatus. Two-dimensional imaging in the parasternal short axis (PSA) view at the aortic level easily demonstrated the tumor’s presence near the RVOT and pulmonic apparatus. Spectral and color Doppler analysis showed an abnormal increase in blood flow velocities through the RVOT and main pulmonary artery, mimicking a pathological situation of pulmonic and infundibular stenosis, which may have contributed to the patient’s complaint of chest pain and dyspnea.
Conclusion
Sonographic evaluation of mediastinal masses is becoming more common due to its widespread availability and ability to characterize the internal appearance of the mass. In this case, the sonographer was required to recognize the tumor’s extracardiac presence by identifying and measuring the size of the tumor and to subsequently use 2D, spectral, and color Doppler analysis to evaluate blood flow characteristics through the RVOT, pulmonary artery, and the main pulmonary artery (PA) of the heart. The use of echocardiography, in this case, defined the interaction of the mass with cardiac structures that was not evident in the chest radiograph.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.