
Abstract
This is a case study of solitary fibrous tumor (SFT), which is a rare neoplasm of mesenchymal origin that comprises less than 2% of all soft tissue tumors. SFT located in the extremities, especially in the legs, has a high possibility of developing malignancy. The case study presented demonstrates a sonogram which identified an inhomogenous hypoechoic solid lesion located in the subcutaneous layer of the femoral region. The use of Doppler showed hypervascular activity in the hyperechoic area. This finding was consistent with malignant SFT and confirmed by histopathologic exam. The possibility of an SFT should be a diagnostic consideration with any large soft tissue mass in extremities. This is a further consideration with the diagnostic medical sonography findings demonstrating a hypoechoic, well-defined mass that has a large collateral feeding vessel and displaces the adjacent structures.
A solitary fibrous tumor (SFT) is a rare neoplasm of mesenchymal origin that comprises less than 2% of all soft-tissue tumors. 1 SFT occurs in adults 20 to 70 years old and most frequently in those of about 54 years of age, with no gender predilection. 2 SFT components show a mix of connective tissue, cells, and hypervascular areas that consist of varied sizes of multiple blood vessels. 3 SFT has been related to hypoglycemia as well as the production of insulin-like growth factor, osteoarthropathy, and arthralgia. 4 SFTs can be found in the head (mostly in the orbital area), chest wall, mediastinum, pericardium, retroperitoneum, abdominal cavity, or in rare sites such as the meninges, salivary glands, adrenals, urinary bladder, or testis. 2 Forty percent of SFT cases are found in the subcutaneous layer of tissue. 3 Although an SFT is considered a benign tumor, because of its well-defined soft-tissue composition, 10% to 15% of SFTs recur and/or metastasize. 3 An SFT located in the extremities, especially in the legs, has a high possibility of developing into a malignancy. 3 It is important to use diagnostic medical sonography effectively to determine the characterization of a suspected lesion. 5 The radiologist interpreting the sonogram is expected to provide useful information to the referring physician as well as classify the tumor as benign or malignant. 6 The proper diagnostic approach for either a benign or malignant tumor will determine the proper treatment for the patient.
Case Report
A 27-year-old woman came to the surgical clinic of PKU Muhammadiyah Hospital in Gamping Yogyakarta with a chief complaint of a lump in her upper left thigh. The lump was initially soft; however, over 10 months, it had grown to the size of an egg. Because the patient felt pain and the lump was getting bigger, she presented to the hospital. The physical examination confirmed a lump that was hard on palpation and clinically immobile.
The clinician suspected a possible aneurysm. The sonogram, however, demonstrated a inhomogenous hypoechoic solid lesion. It was located in the subcutaneous layer of the femoral region, measuring 7 cm × 6 cm in diameter. It had a well-defined margin that deviated from the course of the femoral artery and vein inward, medially. It was 1.37-cm away from the left femoral artery and vein. The use of Doppler showed hypervascular activity in the hyperechoic area (Figure 1).
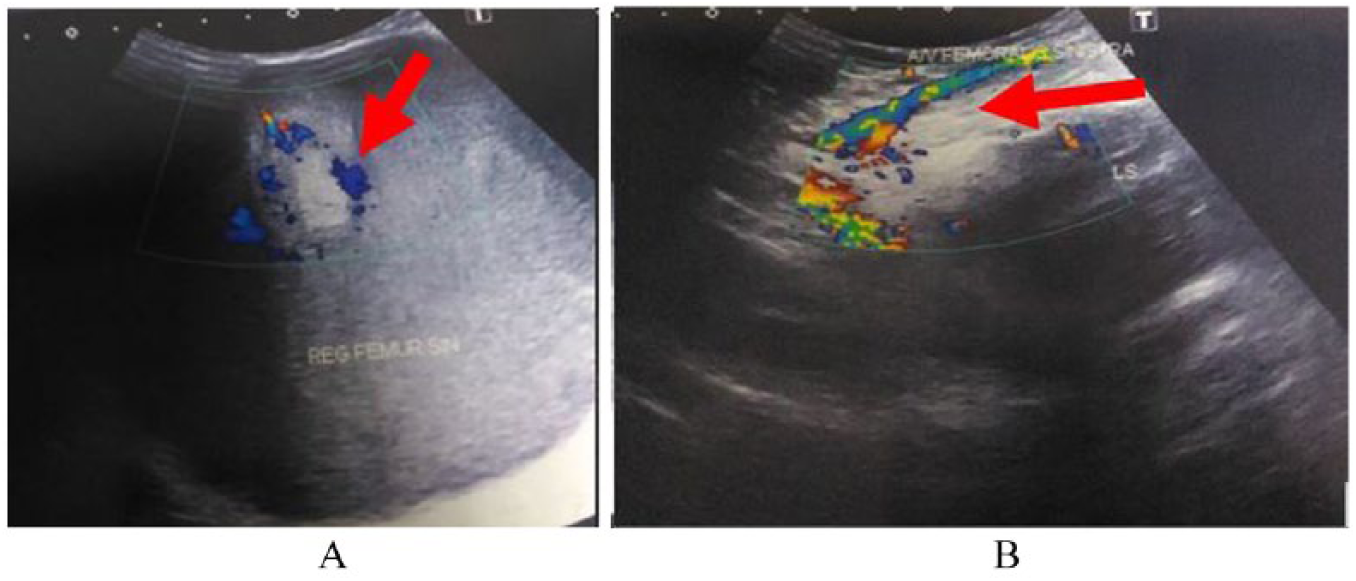
(A) Inhomogeneous hypoechoic solid lesion in the soft tissue of the left femur region. Color Doppler demonstrated hypervascular activity in the hyperechoic component. (B) This lesion deviated from the femoral artery and vein inward toward the medial region of the left femur.
Tumor resection was performed the following day at the site of the tumor. The surgeon found a solid mass with some fatty components. The tumor’s diameter was approximately 15 cm (Figure 2). Histopathological examination with hematoxylin and eosin (HE) showed a malignant solitary fibrous tumor (SFT) with a differential diagnosis of a malignant epithelioid hemangioendothelioma. 1 A microscopic examination revealed a highly cellular tumor that was composed of round cell nuclei to spindles, granular core chromatin, and both solid as well as partially loose material. Within the tumor, the space adjacent to endothelial cells demonstrated some mitosis (Figure 3).

Gross images of the extracted tumor. The partially solid tumor tissue had a yellowish color, with some fat components.
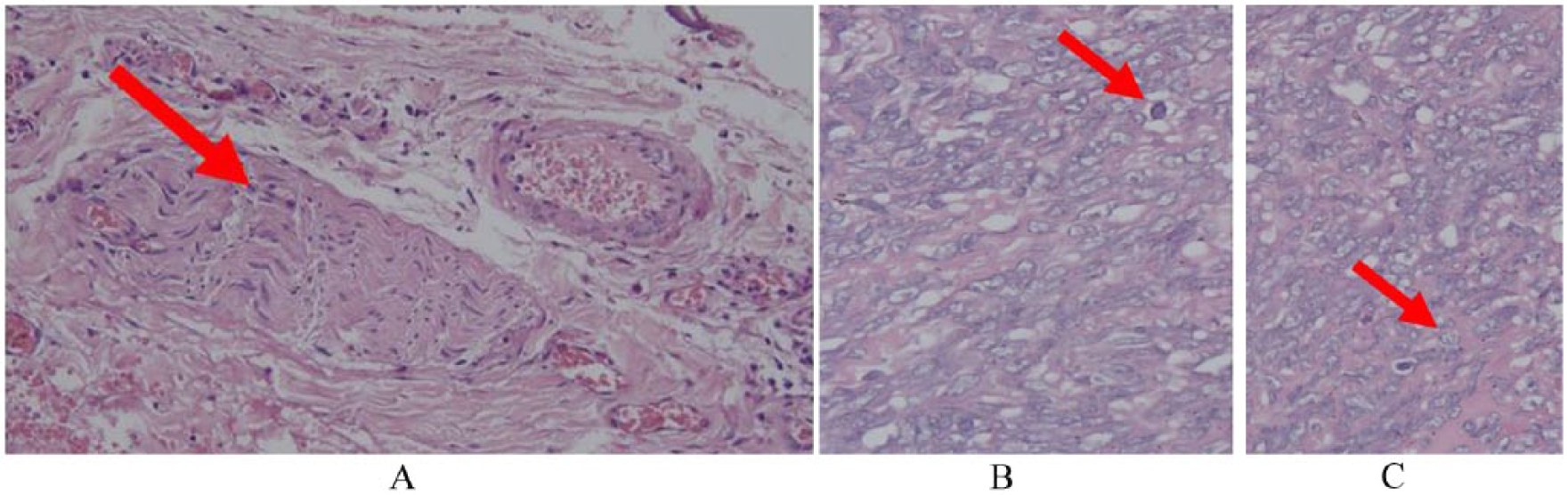
Highly cellular tumor composed of round cell nuclei to spindles (a), granular core chromatin (b), partially solid, partially loose tumor tissue that surrounds the space adjacent to endothelial cells. (c) Some evidence of mitosis can be found with hematoxylin and eosin staining (100× and 400×).
Discussion
Diagnostic medical sonography (DMS) was useful in determining the extent, consistency, vascularity pattern of the lesion, and the presence of invasion to bone. 4 A suggested soft-tissue tumor assessment algorithm with DMS would include (1) clinical and physical examination of the patient, (2) location and characterization of the tumor’s structure, (3) gray-scale sonographic evaluation of the tumor, (4) Doppler integration of the vascularity of the lesion, (5) dynamic examination, and (6) a diagnostic differential that includes advanced imaging, such as magnetic resonance imaging (MRI), when DMS cannot differentiate between benign or malignant soft tissue.7,8
The importance of the clinical and physical examination of the patient is that it provides important information for the radiologist. A long-standing soft-tissue mass that is relatively stable in size would suggest a benign tumor. 4 When this entity is found in children, the most likely diagnosis is a hemangioma or lymphangioma. 7 A history of previous trauma may suggest hematoma or seroma. 7 However, 21% of malignant soft-tissue masses or sarcomas have a history of trauma at the site of the tumor.8,9 Interestingly, the patient in this case had no history of trauma, so it was possible to exclude a diagnosis of hematoma or seroma.
Clinically, SFTs are often diagnosed at an early stage, presenting as pedunculated localized masses with benign histologic features. The patient outcome is favorable after a complete resection of the mass. 10 The patient in this case report complained of pain due to a growing lump. Pain sensation can be a possible indicator of soft-tissue sarcoma.4,5,7 Pressure-induced pain that spreads to a specific area may indicate a neurogenic tumor. 8 This particular patient had no referred pain, so it was possible to exclude the diagnosis of a neurogenic tumor.
When identifying a tumor with DMS, the sonographer/sonologist needs to indicate whether the tumor is subcutaneous, intramuscular, intermuscular, originating from nerves or blood vessels, juxta-articular, or attached to the tendon sheath. 11 The superficial location refers to the subcutaneous tissue and the skin above the superficial investing fascia, which separates the subcutaneous tissue from the underlying muscle. Soft-tissue tumors located in the inner layer (deep soft-tissue tumor) that have a heterogeneous appearance and echotexture on DMS, internal hemorrhage, or necrosis could suggest a possible malignancy.4,11
Guidelines from the National Institute for Health and Care Excellence and European Society for Medical Oncology have used 5 cm as the diagnostic cutoff for the size of a characteristic malignant lesion. 11 This is in agreement with the work by Chari and Campbell, 7 who suggested that a lesion greater than 5 cm indicates a diagnosis of a soft-tissue sarcoma. The size of the lesion in the present case was 7 cm × 6 cm, suggesting a sarcoma.
Fascia edema, skin thickening, hemorrhage, and necrosis are highly significant factors leading to malignancy.8,11 Peritumoral lobulation and edema are also significant factors that suggest malignancy. An obtuse angle formed between the superficial investing fascia and the subcutaneous mass that crosses the fascia would suggest a malignancy. Malignant tumors of the subcutaneous compartment have a greater tendency to develop a close relationship with the fascia than benign lesions, as illustrated in Figure 4. 8
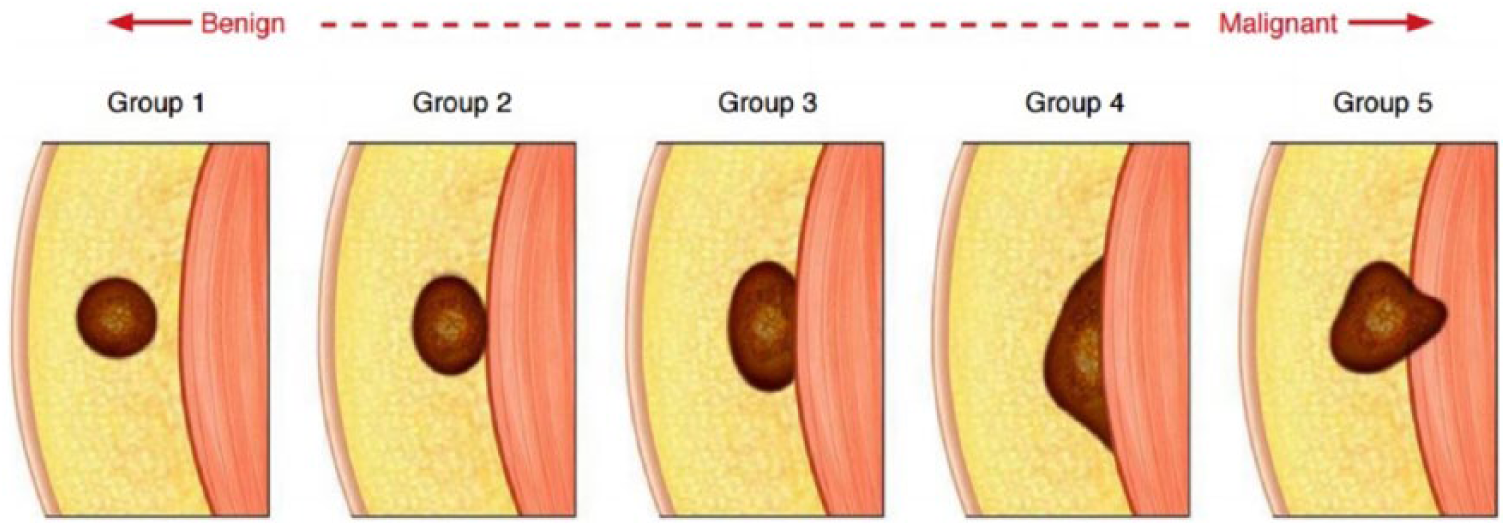
Schematic image of the tumor relationship with fascia. A tumor without fascia contact (group 1) or minimal contact with the fascia (group 2) leads to a benign tumor profile, whereas a tumor that contacts the fascia widely an obtuse angle (group 4) and crosses to the fascia (group 5) strongly suggests malignancy. 12
In the case presented, based on the DMS findings, the tumor had minimal contact with the fascia. This suggests that this was a benign tumor profile (group 2), consistent with previous reports that reveal most SFTs have a well-defined margin. 13 In this patient, there was no fascia edema or skin thickening.
Next, the sonographic gray-scale images in this case study demonstrated an inhomogenous hypoechoic solid lesion. Echogenicity within the mass was associated with an amount of collagen contained within lesion. The higher the echogenicity of a lesion, the more often the lesion contains collagen. The inhomogeneity of the lesions was associated with myxoid degeneration that can appear on the histopathologic examination. 4
Of the various malignant indicators mentioned above, the presence of necrosis in this case was an indicator of malignancy. In color Doppler examination, hypervascularization was appreciated only within the lesion, at the hyperechoic area. The absence of vascularization in the hypoechoic area suggested a process of necrosis. Hypervascularization within the hyperechoic area of the lesion may be caused by a perilesional vessel in a large tumor. This is in concordance with previous reports that collateral feeding vessels were present in 35% of SFTs. 13 Although it is not specific, this sonographic finding may help the radiologist in narrowing the differential diagnosis.
Figure 5 demonstrates the normal anatomy of the femoral vein. Normally vascular structures lie in the dermis layer of the skin, which is derived primarily from mesoderm. In this case, a soft-tissue mass appeared to displace the femoral artery and vein into the superficial layer. Therefore, it is reasonable for clinicians to suspect a femoral aneurysm. An SFT has a tendency to displace adjacent structures, especially the femoral artery or vein, as demonstrated in this case study. 13
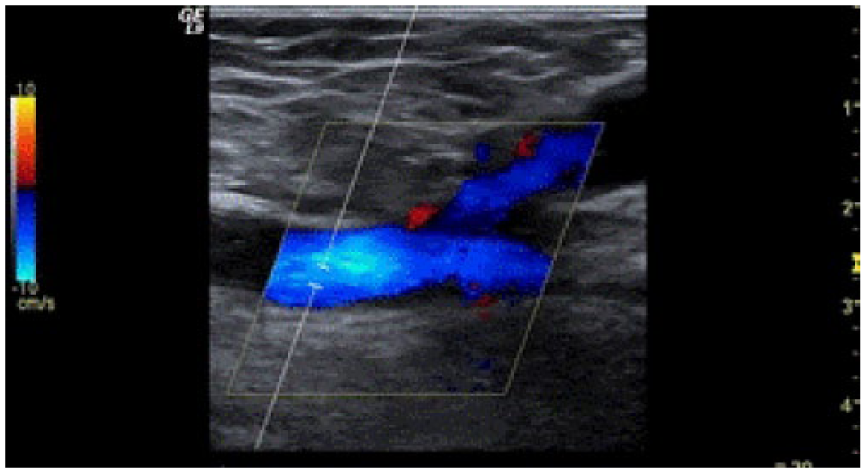
Normal anatomy of the femoral vein within the dermis layer. 14
In addition, a suggested diagnostic algorithm would include a dynamic sonographic examination, which is performed by putting pressure on the mass with the transducer to distinguish a cystic from a solid lesion. Sonopalpation can show the movement of internal echoes, which can suggest a cystic lesion leading to abscess. Although compression may be helpful to distinguish cystic or solid lesions, current elastographic examinations are considered less likely to provide information needed by clinicians than on gray-scale sonograms.8,11
Lastly, important advice given by the radiologist is needed when DMS does not differentiate between a benign and malignant soft-tissue mass. Sonographic features in this study demonstrated a large inhomogenous, hypodense soft-tissue tumor in the subcutaneous layer (measuring more than 5 cm in diameter) that was well defined and displaced the left femoral artery and vein to the medial region. The presence of a huge mass and a large collateral feeding vessel and the displacement of the left femoral artery and vein could be used as diagnostic parameters of malignancy. Nevertheless, MRI is sometimes required to reveal proliferation of fibrous tissue as well as tumor and adjacent tissue, which facilitates surgical decisions for tumor removal. 15
The accuracy of DMS is 79% for assessing a superficial soft tissue mass when a differential diagnosis is considered. The sensitivity and specificity of DMS for characterizing malignant superficial soft-tissue tumors is 94.1% and 99.7%, respectively. 16 DMS has high accuracy for differentiating benign from malignant superficial soft-tissue tumors but nevertheless must still be correlated with histopathologic findings. 15
HE staining in the present case study revealed malignant SFT with a differential diagnosis of malignant epithelioid hemangioendothelioma (Figure 3). The following four standards are used to categorize benign or malignant tumors: (1) high mitotic activity (greater than four mitosis/10 high-power fields), (2) high cellularity with crowding and overlapping of nuclei, (3) presence of necrosis, and (4) cellular pleomorphism. 17 Histopathologic examination in accordance with these four standards allows for a suspected lesion to be classified as a malignant tumor.
The presence of erythrocytes within the cytoplasmic vacuoles is a helpful clue for diagnosis of epithelioid hemangioendothelioma. However, CD34 immunohistochemistry and staining for S-100 are still required to differentiate between SFT and hemangioendothelioma. 18 An SFT will give a positive result for CD 34 and a negative result in S-100 staining. 4
Treatment of lesions by a clinician plays an important role, because incomplete tumor resection will facilitate a recurrence of the mass. An extrathoracic SFT has a significantly higher recurrence rate, especially if tumor resection is incomplete. 13 Factors affecting the recurrence of a tumor are (1) extrathoracic location (especially extremities); (2) invasion of the lesion into adjacent structures, making it difficult for resection; (3) tumor size greater than 10 cm, and (4) malignancy features on histopathologic examination. 13
Long-term follow-up is necessary in this case, because an SFT is often initially found with clinical indications and matched with histopathologic features. 13 SFT management requires a multidisciplinary team of experts in orthopedic surgery, radiology, and pathology. Any soft-tissue tumor findings need to be evaluated for clinical, imaging, and biopsy that will determine the next decision to manage the patient.8,11
Conclusion
The possibility of an SFT should be a diagnostic consideration if there is any large soft-tissue mass in the extremities. This is a further consideration when DMS findings demonstrate a hypoechoic, well-defined mass with large collateral feeding vessel displacing the adjacent structures.
Footnotes
Acknowledgements
The author thanks Winny Setyonugroho, Master of Hospital Administration, Universitas Muhammadiyah Yogyakarta, for his valuable assistance in processing this case report, especially in administration.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.