
Abstract
Solitary fibrous tumors are rare mesenchymal tumors that typically arise from the pleura and rarely originate from the mesentery. We herein report a case involving a 66-year-old patient who presented with a mass on the left abdomen. This mass had been incidentally noticed 10 years earlier. The patient sometimes experienced abdominal pain. Physical examination revealed an irregular mass, which was resected. A biopsy of the mass revealed that it was a solitary fibrous tumor originating from the mesentery of the small intestine. The patient was discharged 1 week after surgery and had an uneventful clinical course throughout the 4-month postoperative follow-up.
Introduction
Solitary fibrous tumors (SFTs) are a group of rare spindle cell mesenchymal tumors mainly arising from the thoracic pleura. These are rare ubiquitous tumors that originate from the mesenchyme and are characterized by high fibrosity and hypervascularity. 1 Although abdominal SFTs have been reported, involvement of the mesentery is rare. 2 SFTs are usually benign and remain asymptomatic unless they place pressure on adjacent tissues, making them hard to detect. Both computed tomography (CT) and magnetic resonance imaging (MRI) can help to diagnose SFTs; however, a definitive diagnosis relies on immunohistopathology, in which STAT6 and CD34 are used as highly specific markers. 3 Macroscopically, most SFTs are well-circumscribed and frequently encapsulated masses. SFTs are typically tan-white, firm, and multinodular in appearance and may exhibit hemorrhagic and myxoid changes. 4 In some instances, SFTs show malignant features and invasion of surrounding tissues. 5 Therefore, complete surgical resection with intact borders is recommended. 6 Because recurrence may occur even 20 years after treatment, 7 long-term surveillance may be beneficial.
Case report
A 66-year-old man was admitted into the general surgery department with intermittent abdominal pain. Abdominal CT revealed a soft tissue mass measuring 101 × 69 × 87 mm and extending along the left lower abdominal peritoneal space (Figure 1). Plain CT revealed an irregular homogeneous low-density mass and surrounding lymph node enlargement (Figure 1(a)). In the arterial phase, numerous blood vessels were observed surrounding the mass. In the venous and delayed phases, the enhancement was seen to extend from the periphery to the center (Figure 1(b)–(d)).

Computed tomography images. (a) Plain scan. Transverse image analysis revealed a mass in the left abdominal region (white arrow). (b) Arterial phase. (c) Venous phase. (d) Delayed phase.
The patient had a >10-year history of a mass on the left abdomen with intermittent pain. The patient could not provide the exact size of the tumor. His abdominal pain was relieved after rest and was not accompanied by diarrhea, constipation, nausea, vomiting, hematemesis, or other abnormalities. However, his abdominal pain had worsened 20 days previously. His stool and urine were normal, and there had been no significant change in his weight recently. The patient had previously undergone an operation involving the vertebrae and ribs as a result of trauma.
Hematological parameters, biochemical parameters and tumor marker levels (CA125, CA19-9, CA72-4, alpha-fetoprotein, and carcinoembryonic antigen) were normal. Surgical exploration revealed a firm mass in the left abdominal region. The mass originated from the mesojejunum and was enclosed by omental adhesions. Therefore complete tumor resection and partial omentectomy were performed to ensure safe surgical margins. Gross examination of the tumor revealed an incomplete fibrous envelope. Histopathological analysis of the mass revealed spindle-shaped cells with hypocellular and hypercellular regions rich in collagen (Figure 2(a)). Cellular atypia, pleomorphism, and necrosis were observed. Immunohistochemical analysis revealed that the mass was positive for CD34, STATA6, CD99, and vimentin (Figure 2(c), (d)) and negative for DOG1, her-2, p53, S-100, and CD117. The mass was also negative for pan-cytokeratin and smooth muscle actin, and the Ki-67 index was 40% (Figure 2(b)), indicating that the tumor cells were actively growing in some areas. The surgical margins were clear. The patient was discharged 1 week after surgery without complications and remained disease-free at the end of his 4-month clinical follow-up period.
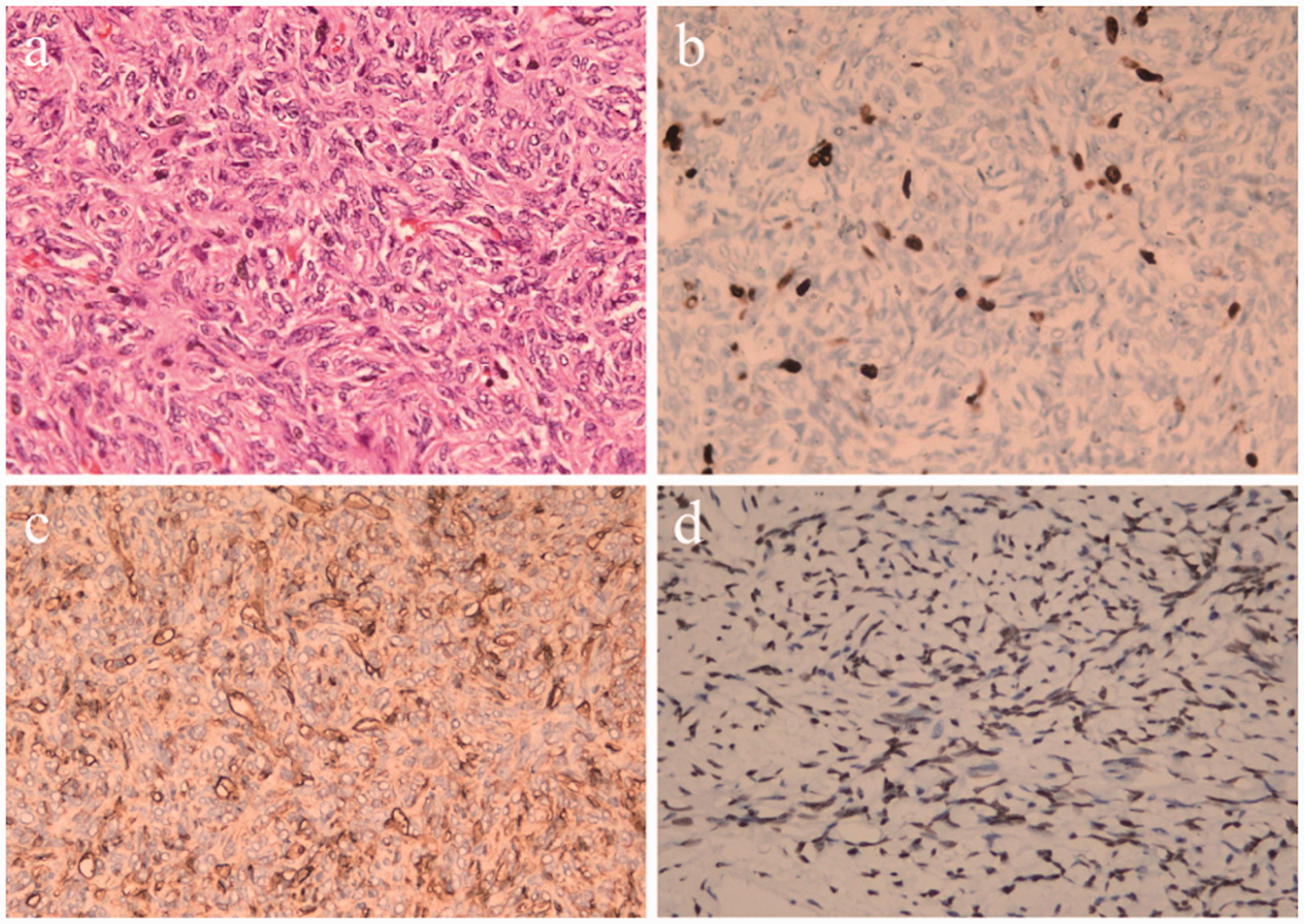
Pathological examination of the neoplasm (magnification: 400×). (a) Spindle-shaped cells with hypocellular and hypercellular areas (hematoxylin and eosin stain). (b) The Ki-67 index was 40%. (c, d) The neoplasm was strongly positive for CD34 and STAT6.
Discussion
SFTs most frequently arise from the pleura, but they have also been observed in nearly every anatomical location of the human body. 8 However, an SFT arising from the mesentery is very rare. 7 A comprehensive literature search revealed 21 SFTs of the mesentery (Table 1). Of these, most were found in men, and the affected patients had a median age of 54 years (range, 26–82 years). These mesentery SFTs seem to more commonly occur in the ileum. As in our case, all cases reported in the literature were treated surgically. Based on these published reports, it is clear that extrapleural SFTs most commonly occur in adults but have a wide age distribution. SFTs are usually slowly growing and painless, with no clinical symptoms unless they compress adjacent tissue. 7
Reports of solitary fibrous tumors of the mesentery in the English-language literature.

M, male; F, female; NROM, no recurrence or metastasis.
CT and MRI are effective in the diagnosis of SFTs. Most tumors are round or lobulated with clear boundaries, and the mass is often large and completely enveloped. 25 On multi-slice CT imaging, SFTs appear as heterogeneously enhancing, multiloculated soft tissue masses. Areas of dense or scattered calcification and central tubular or rounded hypoattenuating regions representing necrosis are also observed. Enhancement is most conspicuous in the arterial and early portal venous phases with washout of contrast in the delayed phase. However, if fibrous elements are predominant, contrast enhancement becomes marked in the delayed phases as well. 4 Multiple peripheral blood vessels were observed in the arterial phase of the present case. This feature is thought to be an important diagnostic factor for SFTs.
SFTs exhibit a heterogeneous appearance on both T1- and T2-weighted MRI, with the appearance of the solid areas ranging from isointense to hypointense relative to skeletal muscle on all sequences. In contrast, cystic areas appear hyperintense on T2-weighted images. The contrast enhancement is similar to that seen on CT imaging.
Differential diagnoses of SFTs include other benign tumors involving the mesentery, such as desmoids, inflammatory pseudotumors, mesenteric fibromatosis, and leiomyomas. Gastrointestinal stromal tumors may be identified by the presence of extensive foci of hemorrhage and necrosis. Malignant lesions of the mesentery that need to be excluded before achieving a diagnosis of SFTs include soft tissue sarcomas, leiomyosarcomas, lymphoma, and metastases. 20 The presence of rounded necrotic areas, calcifications, and the above-described enhancement pattern in the arterial, portal venous, and delayed phases aid in distinguishing between SFTs and other neoplasms arising from the mesentery.
The most effective therapeutic modality for SFTs is surgical resection. The role of other treatment modalities in the management of SFTs is unclear. Some reports in the literature have demonstrated the effectiveness of radiotherapy for the control of SFTs.26,27 Chemotherapeutic drugs and novel targeted drugs seem to exert some activity on SFTs. 28 However, a consensus has not been achieved concerning the effectiveness of radiotherapy and chemotherapy against SFTs.
Conclusion
Although it is difficult to make a definitive diagnosis of an SFT before surgery, CT or MRI may help to identify the tumor. Imaging techniques can be used as the first-choice methods of diagnosing this tumor and for analyzing its morphology, density, and composition. Enhancement is also essential. The primary treatment of an SFT is surgical removal of the tumor with clean margins. Long-term follow-up is necessary after surgery.
Footnotes
Ethics statement
The First Hospital of Lanzhou University does not require ethical approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this case report and its accompanying images.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.