
Abstract
Objective
To compare Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) and Alvarado scores with multislice computed tomography (MSCT) for diagnosing acute appendicitis (AA).
Methods
This retrospective study included patients with abdominal pain who had undergone MSCT, and whose medical notes included RIPASA and Alvarado score parameters. MSCT was compared with RIPASA and Alvarado scores for diagnosing AA.
Results
Of 297 patients included, sensitivity, specificity and accuracy for diagnosing AA were 95.2%, 73.6% and 87.2% for RIPASA score (cutoff value 7.5) and 63.1%, 80.9% and 69.7% for Alvarado score (cutoff value 7). Sensitivity, specificity and accuracy of MSCT for diagnosing AA were 98.9%, 96.4% and 98.0%, respectively. In terms of accuracy, statistically significant differences were observed between RIPASA and Alvarado scores, and between MSCT and RIPASA scores. The mean RIPASA score was significantly different in the simple AA group (9.7 ± 2.2) compared with other AA groups (10.5 ± 1.7). No statistically significant difference was observed in RIPASA score between nonperforated and perforated AA. MSCT sensitivity, specificity and accuracy for diagnosing simple AA were 94.1%, 96.4% and 95.8%, respectively; for differentiating perforated and nonperforated AA, scores were 90.2%, 95.2% and 94.1%, respectively.
Conclusion
MSCT is the optimum diagnostic tool for AA, followed by RIPASA score and Alvarado score, particularly in diagnosing simple and perforated AA.
Introduction
Acute appendicitis (AA) is the most common surgical abdominal emergency, occurring in 7–12% of the general population; 1 its diagnosis is usually based on clinical manifestations and laboratory tests. An atypical type of AA accounts for approximately 30% of cases,2,3 however, and some other diseases resemble its clinical manifestations.4–8 Thus, the correct – and differential – diagnosis of AA is of great importance in informing the choice of clinical treatment.
The Alvarado scoring system, which is based on specific findings observed in AA, was developed to aid AA diagnosis and has been shown to have good diagnostic validity.9–11 The Alvarado score is widely used in the diagnosis of AA due to its convenience, economy and avoidance of radiation exposure, although studies have reported poor diagnostic accuracy for AA when used in women, children and the elderly.12,13 A new scoring system was therefore developed, the Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score,14,15 which produced higher sensitivity and specificity than the Alvarado score. The value of RIPASA for discriminating different stages of AA, however, has not been investigated. Computed tomography (CT), particularly multislice (MS)CT, is widely performed and important in the diagnosis and differential diagnosis of AA because of its higher accuracy than ultrasonography.16,17
In the present retrospective cohort study, medical records from patients with abdominal pain were retrieved and MSCT scan results, and RIPASA and Alvarado scores were analysed to compare their value in diagnosing AA.
Patients and methods
Study population and clinical data
This retrospective cohort study included patients treated for abdominal pain between June 2009 and June 2012 at Jinshan Hospital, Fudan University, Shanghai, China.
The inclusion criteria comprised patients with complete medical records (including MSCT examination) and all parameters required to calculate RIPASA and Alvarado scores. The exclusion criteria comprised children (<18 years old), pregnant female patients and patients who were allergic to iodinated contrast material. Cases of AA with appendectomy performed >24 h following MSCT examination were also excluded, to reduce the bias of AA stages. For the diagnosis of AA, MSCT images, and RIPASA and Alvarado scores, were evaluated retrospectively from complete medical notes.
The study was approved by the Institutional Review Board affiliated to Jinshan Hospital, Fudan University, Shanghai, China (approval No. 2008-34). Since this was a retrospective cohort study, informed consent was not required.
MSCT scan and image interpretation
Abdominal scans were performed using a 64-slice Somatom Sensation 64 MSCT scanner (Siemens, Erlangen, Germany). Lower abdomen scans extended from the superior border of the third lumbar to the pubic symphysis, and whole abdomen scans extended from the diaphragmatic dome to the pubic symphysis. Unenhanced scans and contrast-enhanced scans were performed, and CT scanning parameters were as follows: tube voltage, 120 kV; tube current, 200 mA; collimation, 0.6 mm; reconstruction slice thickness, 1.0 mm; reconstruction interval, 0.5 mm; pitch, 1. Patients suspected of colonic tumour, or ureteral or pelvic lesions, received 1500 ml of water (as negative contrast material), orally at 0.5, 1 and 1.5 h prior to scanning, to improve the quality of image acquisition. Patients suspected of requiring urgent surgery did not receive oral contrast material, to avoid delaying treatment. Patients who underwent enhanced CT were administered 1–1.5 ml/kg Ultravist® 370 (370 mgIodine/ml, Bayer Schering Pharma, Guangzhou, China), intravenously (i.v.) at a rate of 3 ml/s. Scanning commenced 60 s following the initiation of i.v. injection.
The appendix was reconstructed using multiplanar reformation and curved planar reformation techniques. CT findings were evaluated as follows: maximum appendiceal diameter; maximum appendiceal wall thickness; maximum depth of the intraluminal appendiceal fluid; defect in enhancing appendiceal wall; periappendiceal inflammation; phlegmon or abscess; extraluminal air; intraluminal and/or extraluminal appendicolith.
Simple AA was diagnosed when maximum depth of the intraluminal appendiceal fluid was >2.6 mm.18,19 Phlegmonous AA was diagnosed when appendiceal diameter was >6 mm with associated periappendiceal inflammation.1,20,21 Perforated AA was diagnosed when appendiceal diameter was >6 mm with at least one of five specific CT signs: defect in enhancing appendiceal wall, phlegmon or abscess, extraluminal air, extraluminal appendicolith.22,23 Images were evaluated separately by two radiologists (J.W.Q., W.L.) with > 8 years’ experience, who were blinded to the clinical score results during the image evaluation period, and who reached consensus following discussion when disagreement occurred. Mean values were calculated for the two sets of measurement data obtained by the two radiologists.
Alvarado and RIPASA score
Alvarado appendicitis scoring system. 9
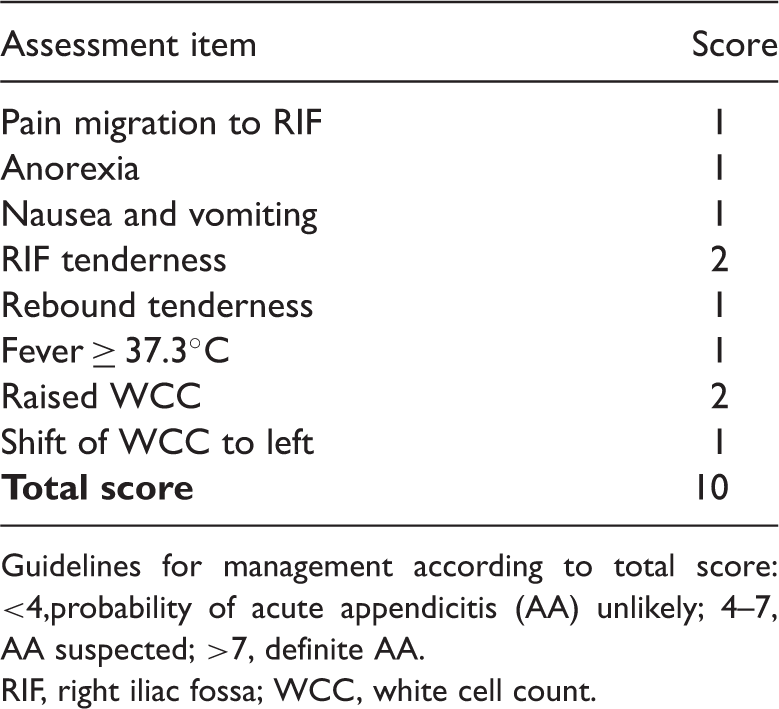
Guidelines for management according to total score: <4,probability of acute appendicitis (AA) unlikely; 4–7, AA suspected; >7, definite AA.
RIF, right iliac fossa; WCC, white cell count.
Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) appendicitis scoring system. 14

Guidelines for management according to total score: <5, probability of acute appendicitis (AA) is unlikely; 5–7.0, low probability of AA; 7.5–12.0, probability of AA is high; >12, definite AA.
Negative urinalysis, absence of blood, neutrophils or bacteria; RIF, right iliac fossa; RLQ, right lower quadrant; WCC, white cell count.
Statistical analyses
Data are presented as mean ± SD, n incidence or %. Statistical analyses were performed using Stata® statistical software, release 7.0 (StataCorp LP, College Station, TX, USA). Based on cutoff values of 7.5 for RIPASA and 7.0 for Alvarado scores,9,14,15 the sensitivity, specificity, and accuracy were calculated for diagnosing AA. Differences in the accuracy of RIPASA compared with Alvarado scores in diagnosing AA were assessed using χ2-test. Differences in the accuracy of RIPASA score for diagnosing simple AA versus other types of AA, simple AA versus phlegmonous AA, and perforated AA versus nonperforated AA were analysed using Student’s t-test. Sensitivity, specificity and accuracy of MSCT for diagnosing simple AA and differentiating perforated from nonperforated AA were calculated. Differences in accuracy, sensitivity and specificity between MSCT and RIPASA scores for diagnosing AA were analysed using χ2-test. A P value < 0.05 was considered statistically significant. Cohen's κ coefficient was used to test inter-rater agreement and a κ-value > 0.75 was considered good.
Results
Distribution of disease, confirmed by pathology results and/or surgery, in 297 patients aged 19–87 years with abdominal pain.

Data presented as n incidence or mean ± SD.
RIPASA, Raja Isteri Pengiran Anak Saleha Appendicitis.
AA, acute appendicitis.
Lower abdomen MSCT scans were performed in 194 cases and whole abdomen MSCT scans were performed in 103 cases. Unenhanced scans were performed in 90 cases of phlegmonous appendicitis, and unenhanced and contrast-enhanced scans were performed in the remaining 207 cases.
Interobserver agreement between the two radiologists who evaluated CT images was very strong, with a κ-value, 0.96. Interobserver agreement between the two surgeons who evaluated the Alvarado and RIPASA scores was less strong, but still good, with a κ-value of 0.76.
The sensitivity, specificity and accuracy values for diagnosing AA were 95.2% (178/187), 73.6% (81/110) and 87.2% (259/297) for RIPASA score (cutoff value 7.5) and 63.1% (118/187), 80.9% (89/110) and 69.7% (207/297) for Alvarado score (cutoff value 7), respectively. There was a statistically significant difference between RIPASA score and Alvarado score in terms of diagnostic accuracy for AA (χ2 = 26.93, P < 0.001).
The sensitivity, specificity and accuracy of MSCT for diagnosing AA were 98.9% (185/187), 96.4% (106/110) and 98.0% (291/297), respectively. There were significant differences between MSCT and RIPASA scores in terms of diagnostic accuracy (χ2 = 25.13, P < 0.001), sensitivity (χ2 = 4.59, P = 0.03), and specificity (χ2 = 22.28, P < 0.001) for AA. (Figure 1). A statistically significant difference was found between the mean RIPASA score for the simple AA group (9.7 ± 2.2) compared with the other types of AA grouped together (10.5 ± 1.7; t = −2.32, P = 0.02). The mean RIPASA score in the phlegmonous AA group (10.4 ± 1.7) was significantly different from the simple AA group (t = −2.16, P = 0.03). No statistically significant difference was found in RIPASA score between the nonperforated and perforated AA groups (t = −0.84, P = 0.40). Diagnosis of simple AA using MSCT revealed sensitivity, specificity and accuracy values of 94.1% (32/34), 96.4% (106/110) and 95.8% (138/144), respectively. Use of MSCT for the differential diagnosis of perforated versus nonperforated AA revealed sensitivity, specificity and accuracy values of 90.2% (37/41), 95.2% (139/146) and 94.1% (176/187), respectively. Representative CT scan images are shown in Figures 2–4.
Flow diagram showing multislice computed tomography (MSCT) and Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score diagnostic accuracy in patients with or without acute appendicitis (AA). CT (+), case diagnosed as AA by MSCT; CT (−): AA ruled out by MSCT. Representative multislice computed tomography (MSCT) scan image showing phlegmonous acute appendicitis (AA). In this case, Alvarado score was 3 and Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score was 10. The appendix was reconstructed using the multiplanar reformation technique; arrow indicates the appendix (diameter, 11.6 mm) with periappendiceal inflammation; appendicolith and fluid seen in appendiceal lumen; CT findings met the diagnostic criterion of phlegmonous AA. Representative multislice computed tomography (MSCT) scan image showing simple acute appendicitis (AA). In this case, Alvarado score was 2 and Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score was 6.5. The appendix was reconstructed using the multiplanar reformation technique; arrow indicates the appendix (diameter, 8.5 mm) without findings of periappendiceal inflammation; fluid seen in appendiceal lumen (diameter, 3.1 mm); computed tomography findings met the diagnostic criterion of simple AA. Representative multislice computed tomography (MSCT) scan image showing perforated acute appendicitis (AA). In this case, the Alvarado score was 7 and Raja Isteri Pengiran Anak Saleha Appendicitis (RIPASA) score was 10.5. The appendix was reconstructed using the multiplanar reformation technique; the long arrow indicates markedly enhanced and swelling appendix (diameter, 12.8 mm); the short arrow indicates defect in enhancing appendiceal wall located in the distal appendix; periappendiceal abscess with rim enhancement was observed; computed tomography findings met the diagnostic criterion of perforated AA.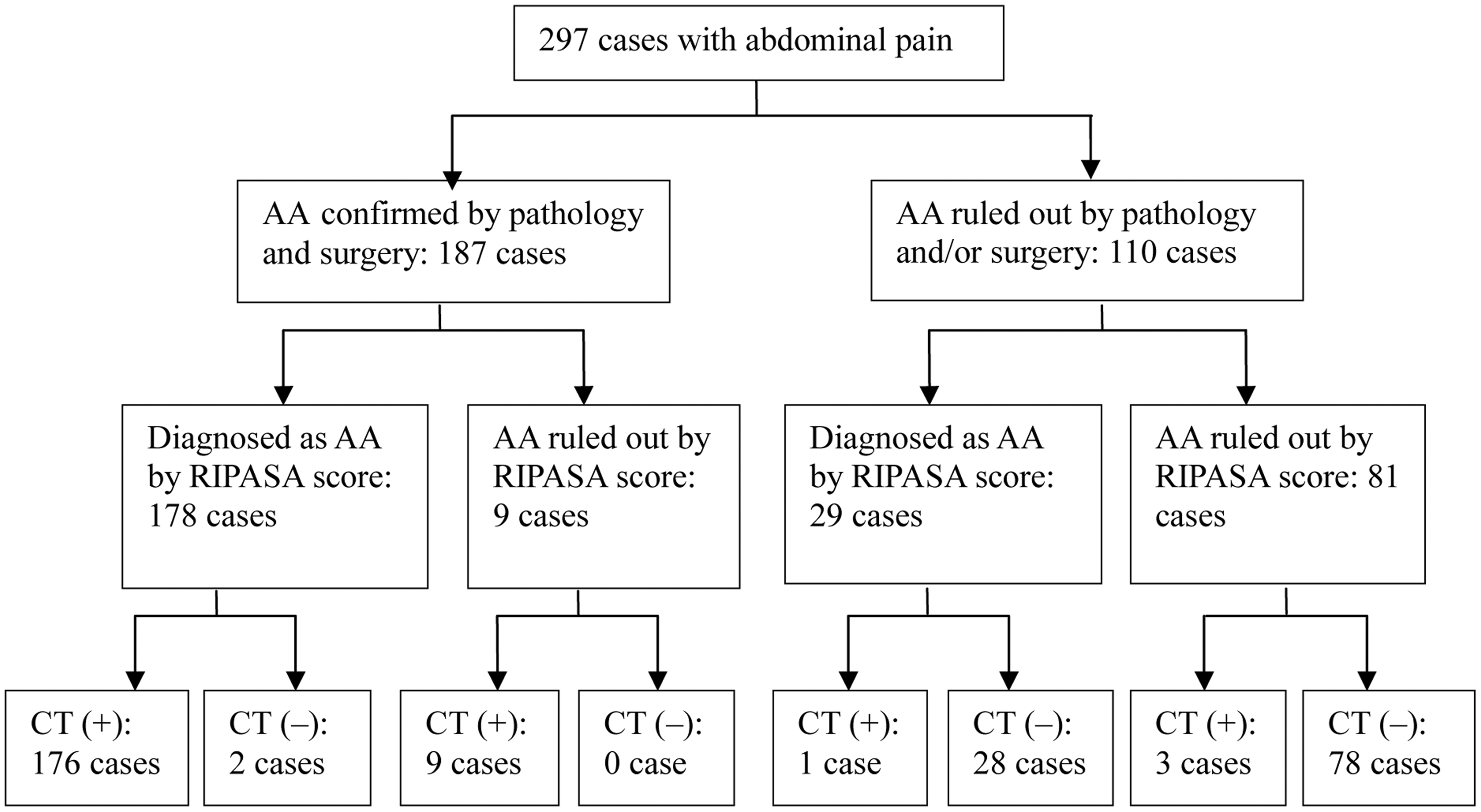



Discussion
In the current study of adults with abdominal pain, cutoff values of 7.5 for the RIPASA score and 7 for the Alvarado score yielded sensitivity, specificity and accuracy of 95.2%, 73.6% and 87.2% (RIPASA), and 63.1%, 80.9% and 69.7% (Alvarado), respectively, for diagnosing AA. The RIPASA score had a significantly higher diagnostic accuracy compared with Alvarado score in the current study, and concurred with the results of previous reports,14,15 in which the diagnostic value of RIPASA score was higher than that for the Alvarado score for diagnosing AA. The RIPASA score contains parameters such as age and sex, which could increase the accuracy compared with Alvarado score, and the RIPASA score also contains more parameters that could aid with the differential diagnosis of AA. All 14 parameters of the RIPASA score are easily obtained from good clinical histories, examinations and investigations, and RIPASA score is easy to implement without additional costs. Compared with the Alvarado score, therefore, the RIPASA score may be more appropriate for the diagnosis of AA.
Computed tomography is thought to be important in the diagnosis and differential diagnosis of AA,3,16,17 however, no studies to date directly compare the RIPASA score with CT in the diagnosis of AA. In the current study, the sensitivity, specificity and accuracy of MSCT were significantly higher than those of the RIPASA score for diagnosing AA. There were statistically significant differences in diagnostic accuracy, sensitivity and specificity between MSCT and RIPASA score, indicating that MSCT is an important supplement to RIPASA score. This may be because the RIPASA score lacks highly specific parameters, and in many other diseases (including inflammation of the caecum and/or ascending colon, gastrointestinal perforation, and right ureter calculus), a few abnormal parameters that are included in the RIPASA score often develop.
The diagnostic value of the RIPASA score has been documented as being higher than the Alvarado score for AA,14,15 however no study has reported the diagnostic value of the RIPASA score for different types of AA. In the current study, the RIPASA score for the simple AA group was significantly lower than for other types of AA grouped together, indicating that the diagnostic value of this score for simple AA was lower than for other types of AA grouped together, based on the guidelines for management according to RIPASA total score. This may be explained by the fact that simple AA had more atypical presentations than other types of AA grouped together in the current study and, therefore, RIPASA score could not effectively address the problem of differentially diagnosing simple AA.
Comparable with published reports,18,19 the sensitivity, specificity and accuracy of MSCT for diagnosing simple AA were 94.1%, 96.4% and 95.8%, respectively, indicating that MSCT is an important procedure for the diagnosis of simple AA.
Clinical management options for perforated AA are reported to be different from those for nonperforated AA.22–24 The routine treatment of choice for perforated AA is administration of antibiotics and/or drainage, with or without appendectomy 6–12 weeks following antibiotic treatment. In patients with nonperforated AA, prompt appendectomy is recommended to reduce the risk of complications. Thus, differentiating perforated from nonperforated AA can be critically important in order to select the correct therapeutic approach. To date, no study has reported the value of the RIPASA score for differentiating perforated from nonperforated AA, however. In the current study, there was no statistically significant difference in the RIPASA score between the nonperforated and perforated AA groups. However, use of MSCT for differentiating perforated from nonperforated AA revealed a sensitivity, specificity and accuracy of 90.2%, 95.2% and 94.1% respectively, which were similar values to those reported previously.22,23 These results indicate that MSCT is superior compared with the RIPASA score in the differential diagnosis of perforated versus nonperforated AA.
The current study is limited by the fact that it is a retrospective cohort study, however, sample cases with complete medical notes are presented, which improves the accuracy of the results, and provides evidence that may guide the choice of clinical pathway in the diagnosis of abdominal pain. Cases of AA with appendectomy performed >24 h following MSCT examination were excluded, which may have biased the MSCT results, however, this was done to avoid inaccurate reporting of the stages of AA, since some nonperforated AA may rapidly progress to perforated AA after 24 h. 23
In conclusion, the current study suggests that MSCT is the optimum diagnostic tool for AA compared with RIPASA and Alvarado scores, particularly in cases of simple and perforated AA. The study also showed that the RIPASA score may be a superior diagnostic scoring system compared with the Alvarado score for AA, which is important in hospitals where MSCT scans are not readily available. A prospective study of MSCT versus the RIPASA score should be conducted, to further confirm the superiority of MSCT over RIPASA in terms of sensitivity, specificity and accuracy in the diagnosis and differential diagnosis of AA.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the Science and Technology Commission of the Jinshan District of Shanghai (Grant No. 2010-3-18).
Acknowledgement
The authors thank Dr Yong Zhang for collecting the clinical histories as part of his routine duties.