
Abstract
The relationship between migraine headaches and valvular heart disease usually relates to chronic use of ergotamine-based medical therapies. Significant aortic regurgitation can result in decreased global cerebral perfusion, and for patients with migraine headaches, decreased cerebral perfusion represents a key finding in relation to their symptomatology from migraines. Though headaches are rarely regarded as complications of aortic regurgitation, a case study is presented of significant aortic regurgitation in an ergotamine-naïve patient whose symptoms resolved after valve replacement surgery.
Introduction
Migraine headaches affect 10% to 20% of the general population, and in those who develop more severe or recurrent episodes, migraines lead to significant disability.1–3 The potential relationship between migraine headaches and cardiovascular disease usually revolves around the presence of an intracardiac shunt or the use of ergotamine-related medications for treatment.4,5 Chronically, ergotamine-based therapies, such as ergotamine or methysergide for headaches and perolide or cabergoline for Parkinson’s disease, increase the risk for development of valvular regurgitation. 6 However, in the case study presented, the patient had developed migraine headaches and was found to have significant aortic regurgitation without a history of ergotamine-related therapy. Further, his migraine headaches resolved after valve replacement surgery.
Case Presentation
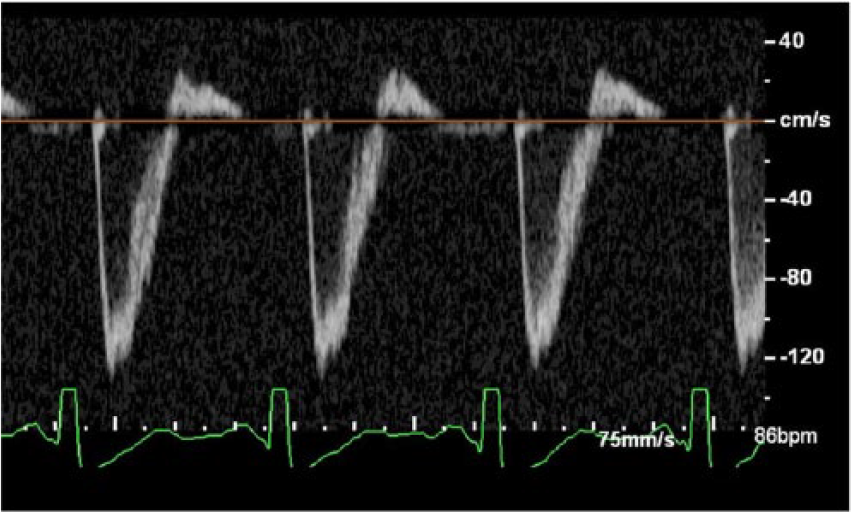
A 34-year-old male with hypertension presented to the student-run free clinic with a five-year history of headaches. These headaches occurred five to six times per day and were variably associated with shortness of breath. In the past two years, they had become severe and resulted in numerous trips to emergency rooms and urgent care centers, usually followed by extensive workups. These workups included brain computed tomography (CT) imaging, brain magnetic resonance imaging (MRI), polysomnograms, pulmonary function tests, and additional appointments with subspecialists. The patient experienced occupational and personal lifestyle limitations as a consequence of his headaches. Chronically, the patient required long-term nonsteroidal anti-inflammatory medications with opiates for significant exacerbations. At our clinic, the patient was found to have a 2/6 diastolic murmur on physical exam and was referred to cardiology. The patient underwent a transthoracic echocardiogram, which revealed severe aortic regurgitation with a low normal ejection fraction (50%) and left ventricular chamber enlargement with an end-diastolic volume index of 105 ml/m2 (Normal: ≤86 mL/m2) as measured from the two- and four-chamber apical views. Doppler images demonstrated a pressure half-time of 200 to 210 milliseconds (Severe aortic regurgitation: pressure half-time <200 milliseconds; see Figure 1). The transesophageal (TEE) confirmed the diagnosis of severe aortic regurgitation (see Figure 2). The vena contracta measured 0.65 cm (Severe aortic regurgitation: >0.6 cm; see Figure 3). Further, the TEE identified three leaflets, which excluded a bicuspid valve as the etiology and demonstrated a gap in the aortic valve closure during diastole (see Figure 4). By planimetry, the regurgitant orifice area measured 0.34 cm2, which by criteria suggested severe aortic regurgitation. With Doppler imaging, the regurgitant volume calculated to be 55 mL with a regurgitant fraction of 52%. The TEE showed diastolic flow reversal in the aortic arch and descending aorta (see Figure 5). An aortic valve replacement surgery was performed, and within one week, his headaches disappeared and have not returned. The patient continued to maintain follow-up visits in the student-run clinic and has had no further issues related to his heart or headaches. Prior to his visit in the student-run clinic, the patient had never been told that he had a heart murmur.
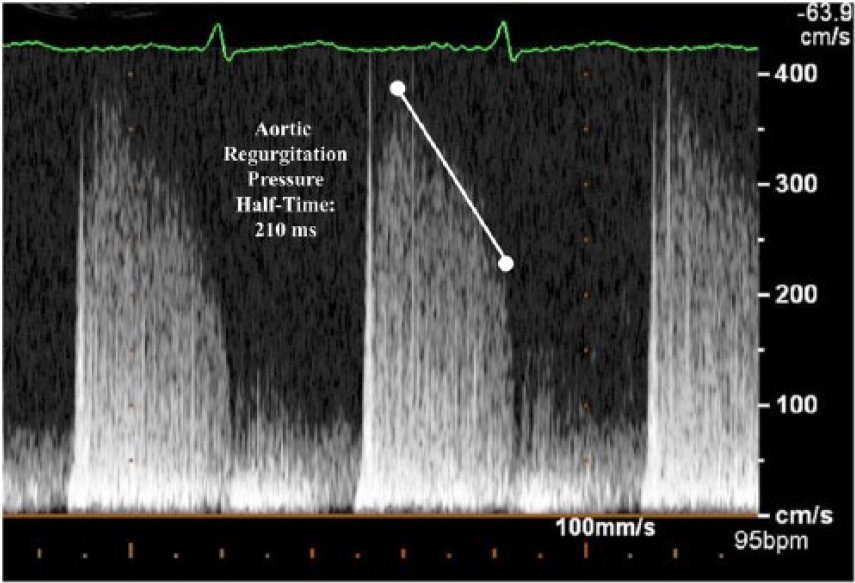
Spectral Doppler image obtained from the apical five-chamber view during a transthoracic echocardiogram.
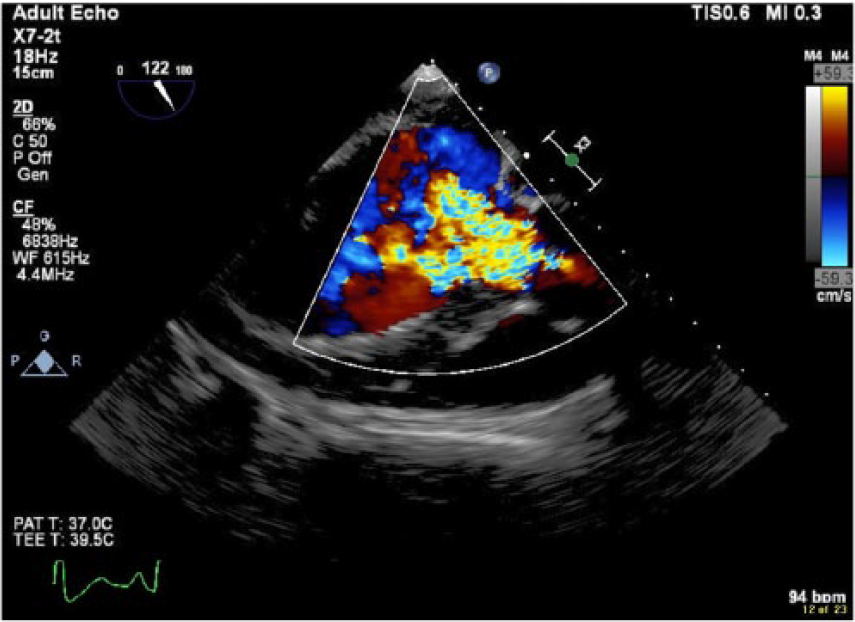
Transgastric view obtained from transesophageal echocardiogram, which demonstrates the aortic regurgitation jet occupying more than two-thirds of the left ventricular outflow tract.
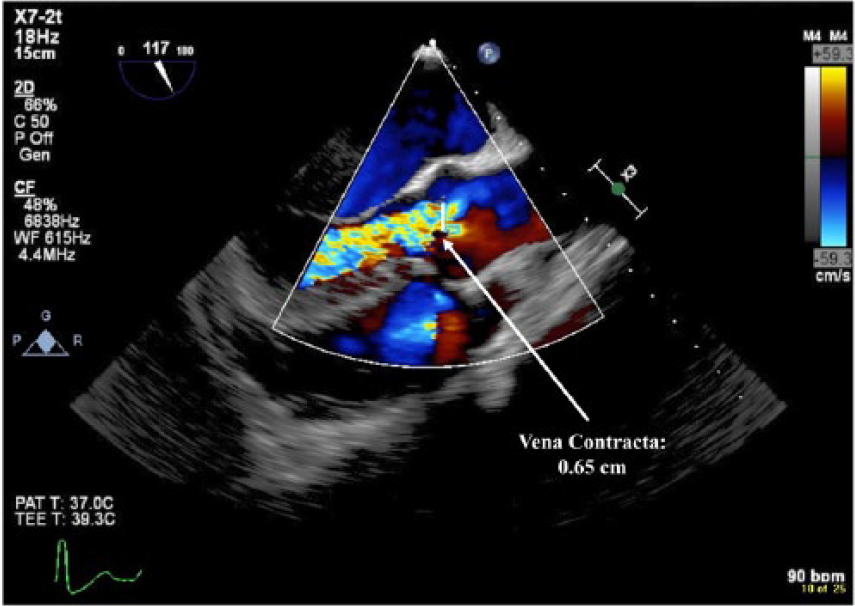
Transesophageal image demonstrating the vena contracta used to assess aortic regurgitation severity.
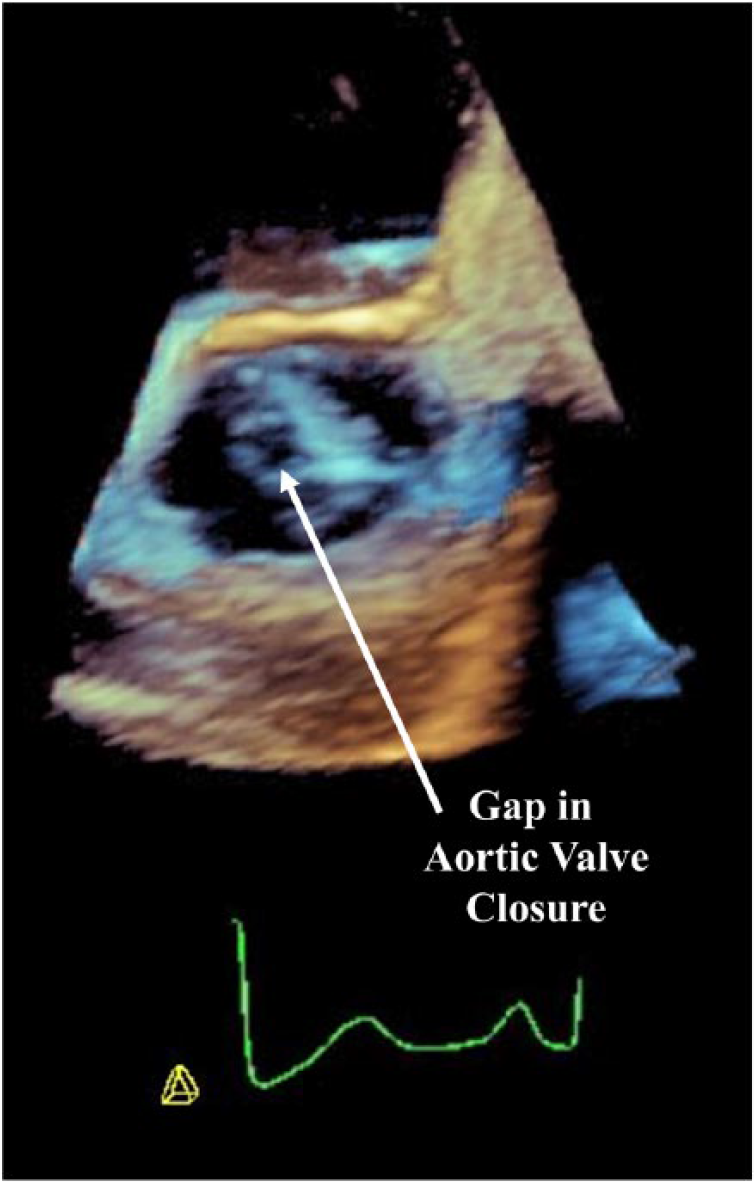
3D transesophageal echocardiographic image showing the etiology of the aortic regurgitation as a gap in closure of the aortic valve.
Spectral Doppler image of the descending thoracic aorta demonstrating diastolic flow reversal.
Discussion
Classically, the most common association between migraine headaches and valvular heart disease is related to certain migraine treatments involving ergotamine-related medications, such as methysergide for headaches and perolide or cabergoline for Parkinson’s disease. As ergotamine-based therapies emerged, Bana et al. 4 noted that patients maintained on chronic therapy were at risk for developing heart murmurs, and with cessation of therapy, some of these findings regressed. More recent investigations described how patients on ergotamine-based medications usually developed valvular regurgitations.7,8 For patients requiring chronic ergotamine-derived therapy, 20% to 25% of patients developed moderate or severe valvular regurgitation, and with a higher cumulative dose, there was a greater risk for developing these valvular lesions. 6 While these relationships are appreciated, the patient in this case study had no significant prior exposure to these agents.
Historically, aortic regurgitation causes a host of notable physical exam findings and symptoms, which are more readily observed due to patients tolerating aortic regurgitation longer than most other valvular lesions. While there are no prior clinical studies to implicate aortic regurgitation as a significant cause of headaches, aortic regurgitation does decrease cerebral blood flow and in rare instances 9 can result in cerebral ischemia. 10 Global cerebral ischemia is often present in patients with migraine headaches. 11 Further, the degree of brain hypoxia during migraines is correlated to the severity of the headache. 11 While not historically associated with headaches, aortic regurgitation may account for this patient’s symptoms, particularly as its repair caused the headaches to cease. When a patient presents with symptoms of migraine headaches, considering other atypical etiologies that stem from nontraditional physiologic causes may lead to better understanding and more accurate diagnoses.
Conclusion
Limited physiologic data suggest aortic regurgitation reduces cerebral blood flow, and in certain clinical settings, this may manifest as significant headaches. This particular patient presented with headaches and a diastolic murmur and was diagnosed with severe aortic regurgitation. After surgery, his headaches resolved. Further studies into the hemodynamics of how valvular heart disease affects other organs may describe side effects or symptoms beyond the heart in these types of patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.