
Abstract
Foramen ovale aneurysm was first documented in 1966. In the case presented, the aneurysm caused restriction of flow across the mitral valve, which in turn caused cardiac ventricular disproportion. Cardiac ventricular disproportion is defined as any subjective visual difference between the right and left chambers of the heart. During the patient’s detailed sonogram, a prominent pericardial effusion was documented; the patient was then scheduled to return for a fetal echocardiogram. During the fetal echocardiogram, ventricular disproportion was noticed, and upon further examination, a foramen ovale aneurysm was detected. At birth, the infant presented with respiratory difficulty, failure to respond to oxygen, and pulmonary hypertension.
Introduction
In 2013, the American College of Radiology and the American College of Obstetrics and Gynecology published guidelines for routine second trimester screening in obstetric sonography, including recommendations for evaluation of the fetal heart. These guidelines state that the four-chamber view and views of the left and right ventricular outflow tracts should be included in the examination. 1 The four-chamber view should demonstrate the foramen ovale flap within the left atrium, which reveals the blood shunting across from right to left. Flow across the foramen ovale from the right atrium displaces the septum primum into the left atrium. The foramen ovale is one of the two fetal shunts that allow blood to bypass the pulmonary circulation. Foramen ovale aneurysm is also known as an atrial septal aneurysm or redundant septum primum flap. 2 Foramen ovale aneurysm and premature atrial contractions are often seen together, and it is thought that the flap extends across the left atrium and interferes with the sinoatrial node–atrioventricular node conduction cycle. 3 Foramen ovale aneurysm was first documented in 1966, 4 and its prevalence is about 0.6% to 1.7% of fetuses during fetal echocardiogram examination. 5
Case Report
A 33-year-old Caucasian female, gravida 4, para 2-1-0-3, presented at 27 weeks 1 day of gestation. The patient was referred for late prenatal care, increased body mass index, previous history of gestational diabetes, and a prior progeny with hydrocephalus. Detailed sonographic assessment revealed a normal anatomic survey, with the exception of a 4-mm pericardial effusion (Figure 1).

Four-chamber view showing the ventricular disproportion and pericardial effusion.
The patient returned three weeks later for a fetal echocardiogram. Images revealed subjective cardiac ventricular disproportion. The left ventricle appeared much smaller than the right ventricle (Figure 2).

Four-chamber view showing the ventricular disproportion and the large foramen flap nearly filling the left atrium.
Upon further inspection, there was a large foramen ovalis flap that appeared to be causing mitral valve obstruction (Figure 3).
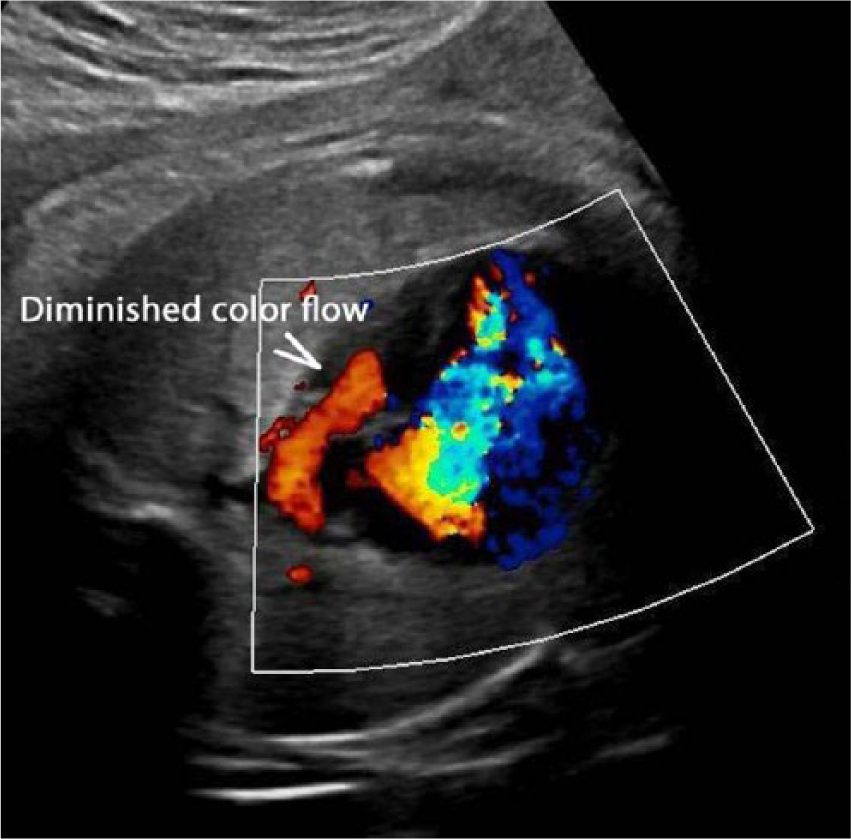
Color Doppler image showing decreased flow into the left ventricle.
The patient returned three weeks later and the left ventricle began to take on more of a hypoplastic appearance. Blood flow was seen to cross the mitral valve; however, it was clearly diminished, with velocities in the 40-cm/s range. Normal flow velocities have a mean of 48 to 49 cm/s through the mitral valve. 6 Color Doppler was also scarcely seen in the left ventricle (Figure 4). The velocities across the tricuspid valve were 87 cm/s.
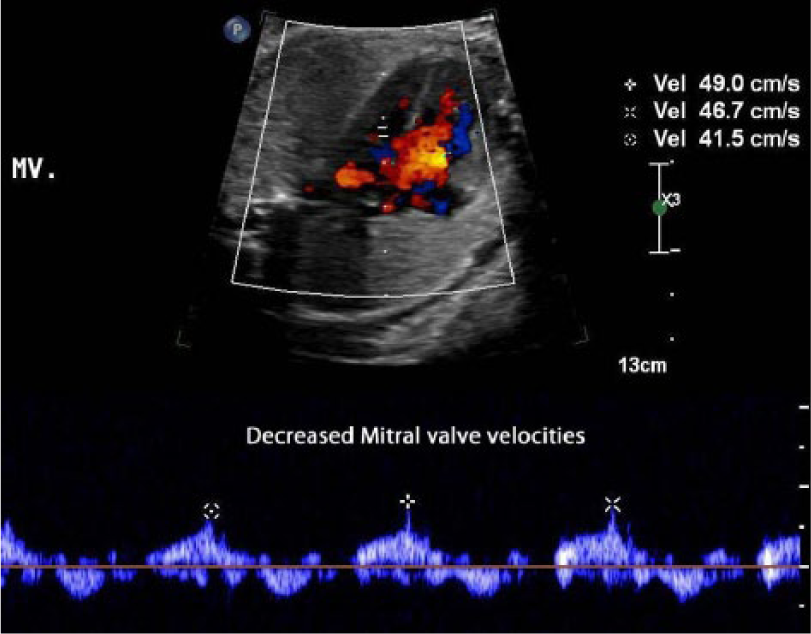
Spectral Doppler waveform showing diminished flow across the mitral valve.
At birth, the infant presented with low pulse oximeter readings at 57% and respiratory distress, which ultimately led to pulmonary hypertension. The infant was then intubated. Next a transthoracic neonatal echocardiogram revealed a small aortic annulus (4.0 mm) and small mitral annulus (8.4 mm). Normal values are 13.8 to 31.8 mm. 7 The left ventricle was underfilled and poorly functioning and appeared hypoplastic. On day three of life, the infant was extubated and placed on continuous positive airway pressure. On day four of life, the infant was converted to a nasal cannula and then subsequently placed on room air. Follow-up echocardiogram demonstrated improvement of the left-side structures when compared with the echocardiogram performed at birth. Color Doppler demonstrated filling of the left ventricle to the cardiac apex, and there was no evidence of left ventricular outflow obstruction. The aortic annulus had improved and now measured 6 mm. The peak gradient across the aortic valve had improved as well. The neonatal heart continued to exhibit mitral valve regurgitation, but the pulmonary hypertension had resolved.
Discussion
Early in fetal development, a thin membranous septum primum separates the atria of the fetal heart. Later in gestation, a thicker septum secundum grows along the primum.5,10 Flow across the foramen ovale from the right atrium displaces the septum primum into the left atrium. After birth, the pulmonary circulation normalizes with the pulmonary venous return, which causes increased left atrial pressure. This increase causes the septum primum to adhere to the septum secundum, closing the foramen ovale.5,10 The foramen ovale is routinely visualized in second and third trimester fetal sonograms while obtaining four-chamber views of the heart. If the foraminal flap extends as much as 50% into the left atrium, it constitutes a foramen ovale aneurysm.5,7
Although it is often an isolated finding, previous research has demonstrated an association between foramen ovale aneurysm and fetal arrhythmias. In one study, 36% of fetuses with foramen ovale aneurysm had premature atrial contractions. 8 If fetal arrhythmia is detected, one should evaluate the foramen flap for redundancy. Other associated anomalies include atrial septal defect, tricuspid atresia, hypoplastic right heart, aortic stenosis, transposition of the great vessels, Epstein’s anomaly, and atrioventricular valve obstruction. 9 In the case presented, it is thought that the foramen ovale aneurysm did indeed cause atrioventricular obstruction. After the foramen ovale closed at birth, the blood flow could then increase across the mitral valve and structures normalized.
Conclusion
Although foramen ovale aneurysm is typically an isolated finding 8 on a fetal sonogram, the present case demonstrated changes to normal cardiac anatomy when perfusion was altered. The redundant flap caused diminished flow across the mitral valve, which then resulted in ventricular disproportion, with the left ventricle becoming small. If a foramen ovale aneurysm is detected in a fetal sonogram, close monitoring and follow-up fetal echocardiograms may be necessary to screen for ventricular disproportion, fetal arrhythmia, and other associated anomalies. Foramen ovale aneurysm is a fairly benign process; however, it can cause other changes to the fetal heart. Close monitoring is necessary to watch for changes associated with obstructed mitral valve flow and fetal arrhythmias. In the present case, closure of the foramen ovale after birth allowed blood flow within the heart to normalize, and structures returned to normal size. However, due to respiratory distress and pulmonary hypertension, the neonate did require medical intervention through day four of life. It is hoped that through the routine visualization of fetal cardiac structures in the second and third trimesters as well as increased resolution of sonographic technology, detection rates of foramen ovale aneurysm in utero will increase, allowing proper care of these infants after birth.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.