
Abstract
Abdominal sonography is the most common imaging method used in the detection of ascites. In the presence of cirrhosis, the most likely etiology of ascites is portal hypertension, secondary to the chronic liver disease. A case study is presented of a male with hepatitis C cirrhosis, with symptoms of ascites, which was confirmed with abdominal sonography. Ascitic fluid obtained by paracentesis confirmed the etiology of the ascites was cardiogenic. Significant improvement was documented after heart failure protocol was implemented. Abdominal sonography can detect the presence of ascites with accuracy but lacks the accuracy to diagnose the precise cause.
Introduction
Ascites is defined as an abnormal fluid collection in the abdominal cavity. Its presence is a sign of serious disease of an underlying organ system and usually carries an unfavorable prognosis. 1 The most likely cause in 80% of cases is portal hypertension from liver cirrhosis. 2 However, ascites can be a consequence, combination, or complication of a number of diseases, including hepatic, cardiac, and renal diseases; infection; and malignancy. The diagnosis of ascites depends on the patient’s signs and symptoms as well as imaging, most frequently sonography. Because many diseases can cause ascites, samples of ascitic fluid must be analyzed to develop an etiology. Combined analysis of the laboratory data and the clinical and pathological data is essential for establishing a precise etiology. Once an etiology for the ascites is established, treatment can be adjusted or implemented accordingly. An unusual case study is presented of grade 3 ascites from a cardiac origin in a patient with concurrent cirrhosis and renal failure.
Case Report
A 48-year-old man with a history of stage V chronic kidney disease on hemodialysis, heart failure with preserved ejection fraction, and untreated hepatitis C presented with a chief complaint of progressively worsening abdominal pain. He also reported abdominal distension for five days. He noted weight gain and shirts not fitting properly around his abdomen starting two months prior but denied fever, chills, trauma, alcohol consumption, or missing hemodialysis.
On arrival to the emergency room, the patient’s primary issue was a distended, uncomfortable abdomen. Labs obtained in the ED revealed normal aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase, total bilirubin, total serum protein, and serum albumin. A sonogram (Figure 1) demonstrated significant ascites. It also was negative for obstructive causes, including portal vein thrombosis. A chest radiograph (Figure 2) revealed evidence of heart failure. A sonographically guided diagnostic paracentesis was performed removing 4.26 L of fluid, which revealed a white blood cell of 130 x 109/L, ascites protein 3.4 g/dL (high), ascitic albumin 1.5 g/dL, serum albumin 2.7 g/dL, and serum-ascites albumin gradient (SAAG) 1.2 g/dL. A total of two paracentesis were performed one day apart with total fluid removal approaching 12 L.
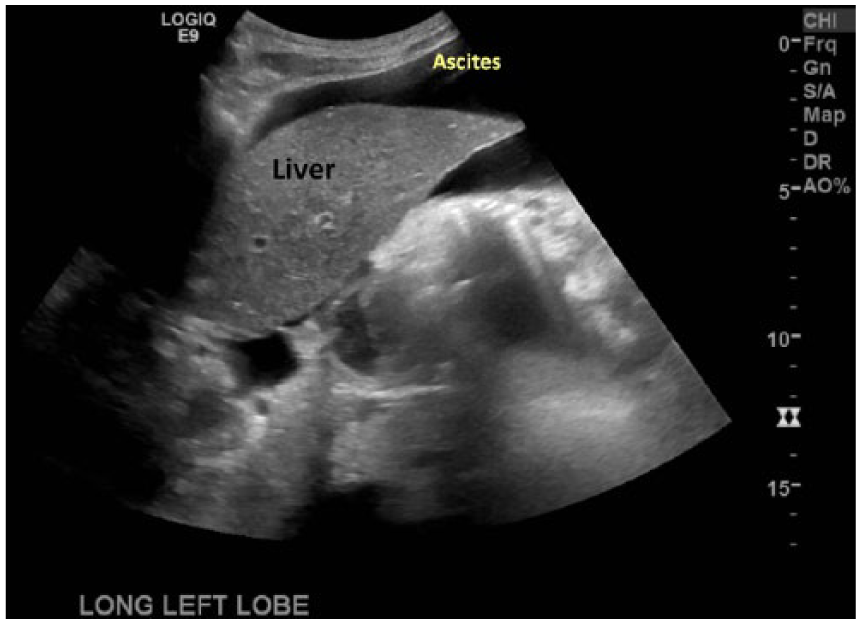
Abdominal sonography demonstrating a large amount of ascites around the liver.
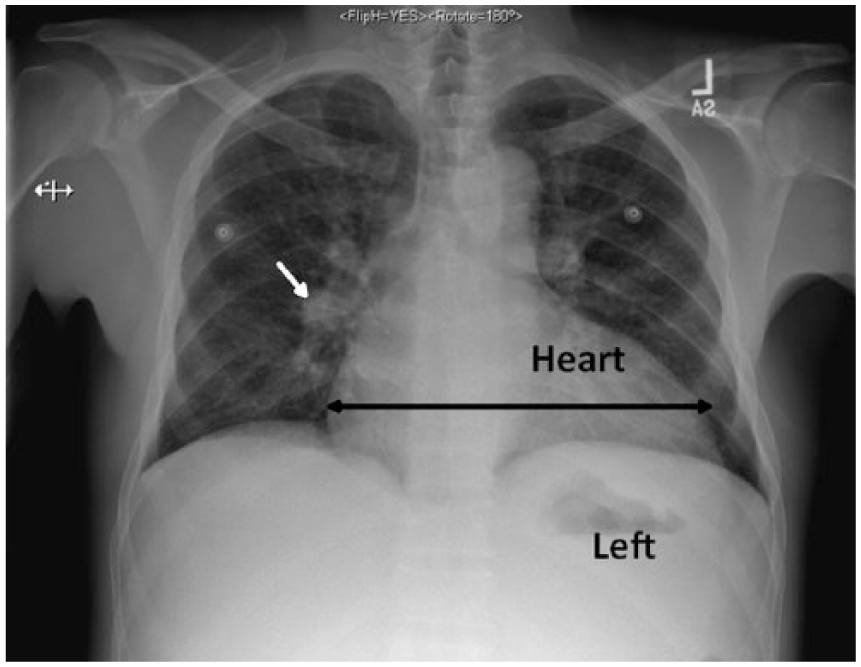
Posterioranterior chest radiograph revealing vascular congestion (short white arrow), mild bilateral interstitial edema, and enlarged cardiac silhouette (long double black arrow), consistent with congestive heart failure.
A cardiology consultation was obtained, and an echocardiogram revealed a normal ejection fraction of 55% to 59%, bilateral atrial enlargement, along with moderate anterior/posterior mitral annular calcification. Mild-moderate mitral valve regurgitation and moderate tricuspid valve regurgitation were appreciated. Cardiology diagnosed acute and chronic congestive heart failure with preserved ejection. B-type natiuretic peptide (BNP) was elevated at 3206 pg/mL due to acute heart failure with preserved ejection fraction and (less likely) fluid overload secondary to stage V chronic renal disease. A computed tomogram (CT) of the abdomen/pelvis scan was obtained (Figure 3) showing a large volume of ascites and signs of liver cirrhosis. Along with hemodialysis and diuresis (patient still produced urine), the patient’s medications were optimized and included metoprolol tartrate, amlodipine, lisinopril, and hydralazine. Cardiology recommended a fluid restriction of 1500 mL/day. Abdominal ascites did not reaccumulate during his hospitalization. He was discharged in stable condition on hospital day nine.
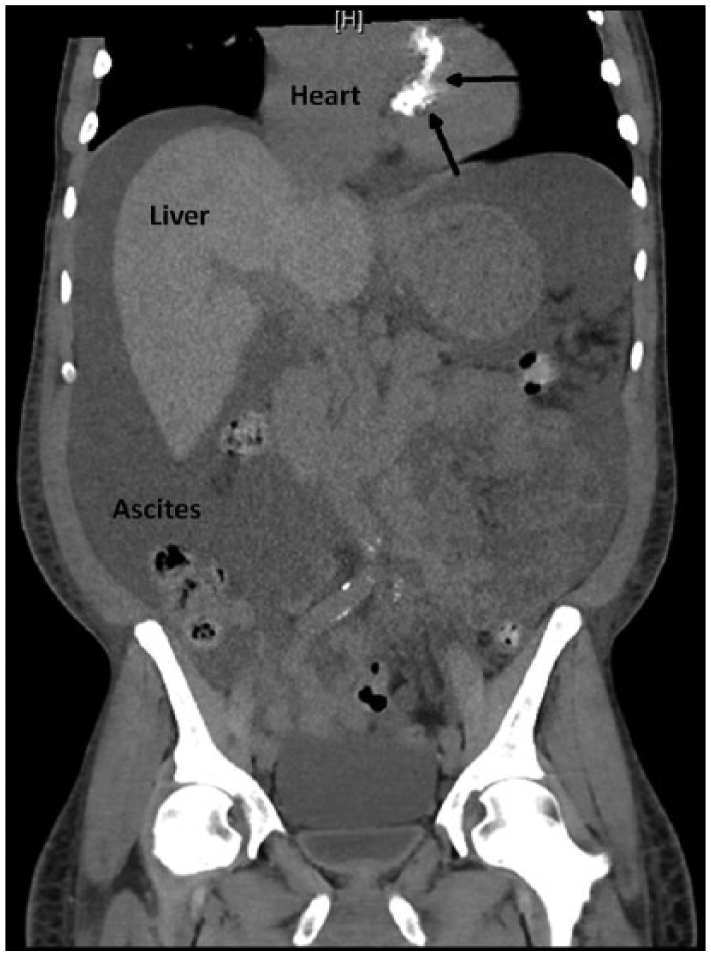
Coronal computed tomogram of the abdomen and chest illustrating abdominal ascites, cirrhotic liver, and mitral annular calcifications (indicated by arrows).
Discussion
This case has three unique elements. First, while probably not the first case of cardiac ascites to occur in a patient with both liver disease and heart failure diagnosed by sonography, it appears to be the first reported. A MEDLINE search was performed specific to English language literature from January 1, 1966, to December 31, 2016, using the keywords cirrhosis, ascites, heart failure, and sonography. No cases could be located of ascites due to heart failure in the presence of cirrhosis using sonography to diagnose ascites.
Second, abdominal sonography plays a pivotal role in the screening and differential diagnosis of ascites. In fact, it has essentially replaced the clinical examination and other radiologic examinations and is now the standard of care. 3 Not only can sonography detect small amounts of intraabdominal fluid, it is also capable of distinguishing intraabdominal cystic and solid masses as small as a few centimeters. 4 Confirming the presence of ascites with sonography, even when cirrhosis and renal failure are present, however, does not define the etiology. Abdominal sonography is thus the method of diagnosing the presence of ascites, not the etiology.
The third and most important element to this report is the unusual cause of the ascites as confirmed by the analysis of the ascitic fluid. Ascitic total protein level alone has been used in the past to determine the etiology of ascites but is not as reliable as the SAAG. 5 The SAAG is high (≥1.1 g/dL) in portal hypertension-related ascites, as in cases of liver cirrhosis or congestive heart failure. 6 Additionally, a high SAAG (>1.1 g/dL) and high total protein (>2.5 g/dL) without hepatic venous outflow tract obstruction is indicative of cardiac ascites.7,8 The patient had a SAAG level of 1.2 g/dL and an ascitic total protein of 3.4 g/dL, which, combined with the clinical presentation and echocardiogram, are pathognomonic for cardiac failure. Cardiac ascites comprises a small minority of all ascites cases, with one publication citing a 5% incidence. 9 In this patient’s case, the treatment course was aimed at continuing hemodialysis for his stage V chronic renal disease to maintain homeostasis, two separate diagnostic and therapeutic paracenteses, and heart failure medications. Cardiology began treatment of heart failure with metoprolol, amlodipine, aspirin, lisinopril, and hydralazine. He was also started on torsemide for fluid control. The patient’s history of noncompliance with hemodialysis and medications, due to financial hardship, resulted in a social work consult to provide the patient with additional resources.
In summary, the initial diagnostic finding of ascites was confirmed by sonography, and despite an obvious cause of cirrhosis, the ultimate condition that resulted in the ascites was cardiac failure. This case demonstrates that a sonographic diagnosis of ascites is an important component in an integrated approach to patient care. This case presents additional complications that point to finishing the diagnostic protocol, which is prudent and leads to pragmatic changes in the clinical decisions used to treat patients with ascites.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.