
Abstract
Objective
In this investigation, we aimed to explore risk factors for 90-day hospital readmission among patients with cirrhosis and ascites in an Asian population.
Methods
In this retrospective study, we included consecutive patients diagnosed with cirrhosis and ascites hospitalized in Renji Hospital between 2018 and 2022 to elucidate risk factors for 90-day readmission. We conducted multivariate logistic regression analysis to identify readmission risk factors.
Results
We included 265 patients with cirrhosis and ascites. A 43% readmission rate was observed within 90 days. After adjustment for multiple covariates, we found that readmission within 90 days was independently linked to reduced levels of hemoglobin (odds ratio [OR] 0.96, 95% confidence interval [CI] 0.94–0.97) and serum albumin (OR 0.88, 95% CI 0.83–0.93), and higher Model for End-Stage Liver Disease and sodium (MELD-Na) scores (OR 1.04, 95% CI 1.01–1.07) at discharge.
Conclusions
Patients with cirrhosis who have ascites are frequently rehospitalized within 90 days after discharge. Lower hemoglobin or albumin and higher MELD-Na scores at discharge may be the main risk factors for hospital readmission.
Introduction
Cirrhosis is the end stage of chronic liver disorder. Cirrhosis leads to substantial morbidity and health care costs, making it a primary cause of global mortality.1,2 Its prevalence in the United States (US) is 0.27%, with a 26.4% mortality rate. 3 Although there has been much advancement in medical and pharmacological therapies, the burden of inpatient care linked to cirrhosis continues to rise. In the US in 2011, there were 658,900 hospitalizations related to cirrhosis, reflecting an annual increase. 4 The cost of hospitalizations for cirrhosis has also been rising steadily. Between 2001 and 2011 in the US, the annual cost of cirrhosis-associated hospitalization doubled from USD 4.8 to USD 9.8 billion, and the mean cost increased from USD 13,079 to USD 15,193. 4 Furthermore, a systematic review revealed a 31% increase in cirrhosis-associated hospitalization costs or portal hypertension complications between 1993 and 2012. 5 These statistics highlight the escalating impact of cirrhosis on health care resources, emphasizing the need for effective management strategies to reduce hospitalizations and the associated costs while improving patient outcomes.
The frequency of hospital admissions is an essential factor contributing to rising health care costs in the US. In 2004, the estimated cost of unplanned readmissions was USD 17.4 billion, accounting for 20% of Medicare hospital payments. The rate of readmission has been proposed as a national quality indicator, and elucidating the modifiable risk factors of readmission is considered essential to reducing the associated costs. 6 Recent studies have indicated that early rehospitalization of decompensated patients with cirrhosis is costly and associated with worse outcomes. 1
It is believed that 27.1% of rehospitalizations are avoidable. 7 For cirrhosis treatment, necessary gastroenterology consultation, 8 early outpatient follow-up, 9 and specialized caregiving protocols such as a “day hospital” 10 all lower the risk of readmission. These are resource-intensive interventions that require risk stratification to identify high-risk individuals. Therefore, much research has been carried out to elucidate the risk factors for readmission in patients with cirrhosis,11–23 which include cirrhosis-linked complications, higher discharge Model for End-Stage Liver Disease (MELD) scores, the number of medications at discharge, presence of diabetes, and male sex as independent readmission predictors11–23 in Western countries, but not in China.
Ascites is among the most frequent complications of cirrhosis, occurring in approximately 50% of patients within 10 years of diagnosis. 24 The development of ascites marks a critical step in the pathogenesis of cirrhosis, indicating substantial portal hypertension and signaling decompensated disease. Compared with other complications, patients with ascites are at high risk of frequent hospitalizations and readmissions for cirrhosis. 25 Therefore, the identification of risk factors for readmission in patients with cirrhosis and ascites is important to avoid rehospitalization.
This investigation specifically focused on patients with cirrhosis and ascites with the aim to delineate factors influencing the readmission risk in this high-risk subgroup compared with more general cirrhosis cohorts in the literature. Because risk factors likely vary across geographic regions according to patterns of race and ethnicity as well as practice, this research provides uniquely important data for Asian populations.
Methods
This retrospective observational investigation was carried out at Renji Hospital from January 2018 to December 2022. This research was authorized by the review board of Renji Hospital in January 2023 (approval no. was KY2021-285-B), and the study protocol was followed in accordance with the provisions of the 1975 Declaration of Helsinki. Prior approval was acquired from the institution’s human research committee. Waiver of informed consent was granted by the ethics committees of Renji Hospital. All patient details have been de-identified to maintain confidentiality and comply with ethical guidelines. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 26
Patients
Consecutive patients with cirrhosis confirmed via imaging tests, liver biopsy, or clinical data for a cirrhosis-linked complication, as well as those with evidence of cirrhosis with ascites confirmed on ultrasound during the index hospitalization, were included in this research. The exclusion criteria were 1) death or discharge to hospital care, 2) liver transplantation before or during hospitalization, 3) missing outcome data for readmission within 90 days after discharge at the index hospitalization.
Variables
The data collected during the index hospitalization included demographic information such as patients’ age, sex, and insurance. Additional data included the patient’s history of alcohol use, smoking, marital status, cirrhosis etiology, length of hospitalization, comorbid conditions, and Charlson comorbidity index. Routine laboratory parameters were also assessed, and the Child–Turcotte–Pugh (CTP) model for MELD and sodium (MELD-Na) scores were used to elucidate liver disease severity. Additionally, the change in CTP (ΔCTP) and MELD-Na (ΔMELD-Na) scores at discharge was calculated as the CTP or MELD-Na score at the initial examination after hospitalization minus the CTP or MELD-Na score at discharge.
Outcomes
In this study, 90-day readmission was defined as the primary outcome. Subsequent hospital admissions within 90 days after the index hospitalization were recorded by reviewing each patient’s computerized medical record at the institution. These records included documents such as inpatient discharge summaries, history and physical examination, test results, daily notes, and outpatient clinic and telephone notes. Furthermore, notifications by patients, family members, or physicians outside the hospital regarding hospitalization at other institutions were also recorded. This comprehensive approach allowed the acquisition of hospitalization events at other institutions to provide a complete record of subsequent admissions.
Statistical analysis
Statistical analysis was carried out using R software version 4.1.2 (www.r-project.org). The data were summarized using descriptive statistics. For categorical variables, absolute numbers and proportions were calculated. The mean and standard deviation were calculated for continuous variables with a Gaussian distribution. The median and interquartile range were used for continuous variables with a non-normal distribution. Statistical tests were performed to compare different patient groups. For categorical variables, the chi-square test was used whereas for continuous variables with a Gaussian distribution, the Student t-test was applied. For continuous variables that were non-normally distributed and ordinal categorical variables, the nonparametric Kruskal−Wallis rank-sum test was used. These tests were applied to assess differences between patients with and without hospital readmission. Additionally, multivariate logistic regression was used to identify potential predictors of readmission with p < 0.05 in univariate analysis. A p-value <0.05 was deemed statistically significant.
Results
As shown in Figure 1, 265 patients with cirrhosis were included in the analysis. Of these, 114 (43%) were readmitted to the hospital within 90 days. Table 1 lists the characteristics of selected patients at the index hospital admission. In total, 52% of participants were women, with a median age 59 years.
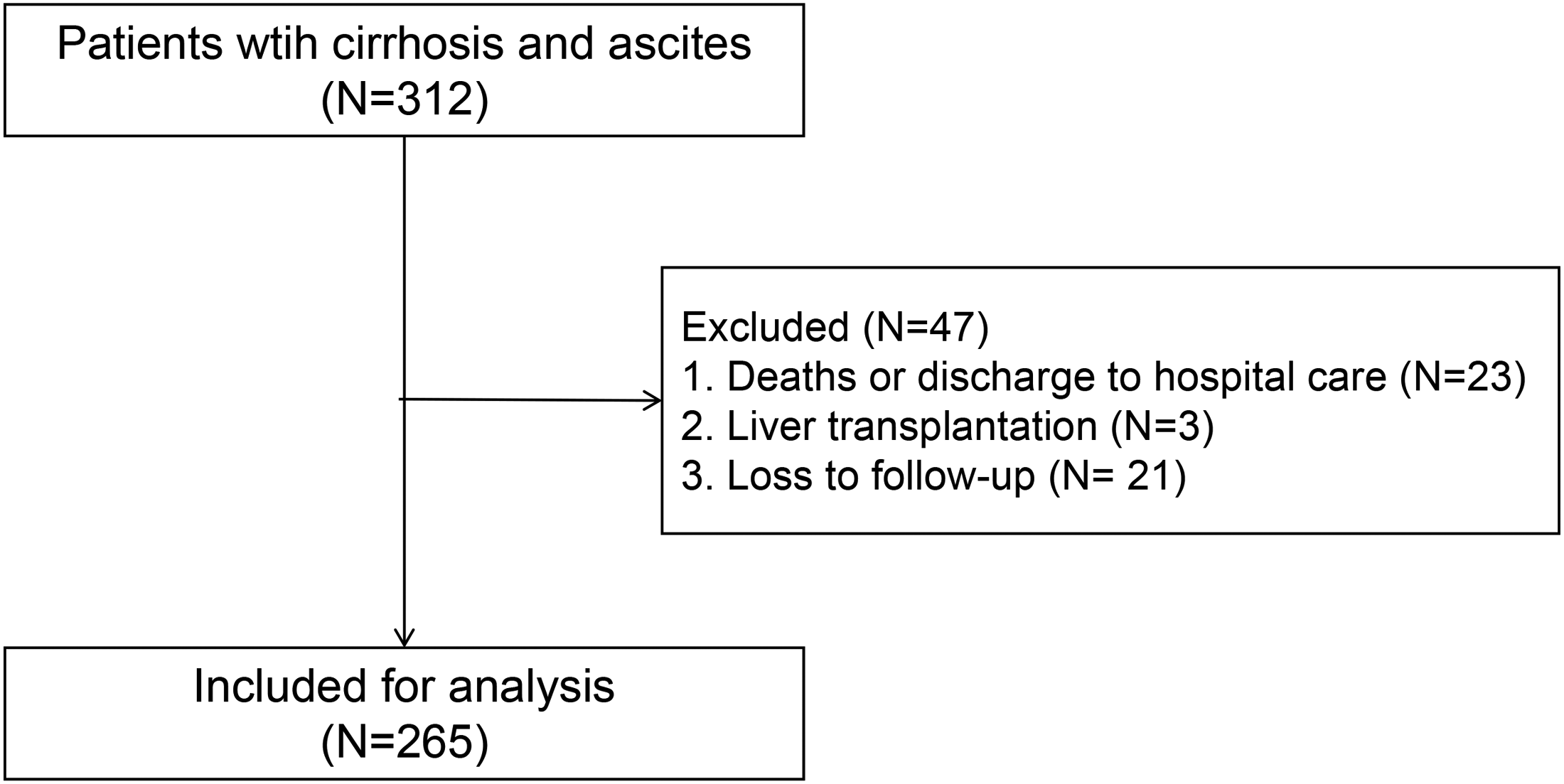
Flow chart depicting inclusion of patients with cirrhosis and ascites in the analysis.
Univariate relationship between baseline variables and 90-day readmission in patients with cirrhosis and ascites.

SBP, spontaneous bacterial peritonitis; HRS, hepatorenal syndrome; HE, hepatic encephalopathy; EGV, esophageal and gastric varices; DM, diabetes mellitus.
Univariate analyses
The analysis of baseline variables (Table 1) showed that within 90 days, readmitted patients had a markedly prolonged median index hospital stay in comparison with non-readmitted patients (16 vs. 13 days, p < 0.001). Moreover, etiological differences in cirrhosis were observed between groups, with a higher percentage of readmission among patients with alcoholic cirrhosis (11.4% vs. 6.62%, p = 0.037) and cirrhosis of unknown etiology (25.44% vs. 17.88%, p = 0.037) compared with those who had an autoimmune etiology. No other baseline variables including age, sex, residence, insurance status, severity of ascites, or comorbidities were significantly different between non-readmitted and readmitted patients.
Univariate analysis of laboratory parameters at discharge (Table 2) during the index hospitalization indicated significant differences between non-readmitted and readmitted patients. Within 90 days, readmitted patients had significantly reduced hemoglobin levels (mean 88.68 vs. 105.04 g/L, p < 0.001) and elevated neutrophil count (median 2.96 vs. 2.24 × 109/L, p = 0.002), C-reactive protein (CRP, median 6.54 vs. 2.78 mg/L, p < 0.001), international normalized ratio (INR, median 1.29 vs. 1.25, p = 0.033), D-dimer (median 1.19 vs. 0.88 mg/L, p = 0.004), and MELD-Na scores (median 14.22 vs. 6.35, p < 0.001) as compared with non-readmitted individuals. Readmitted patients also had significantly lower serum sodium (median 136.1 vs. 139.1 mmol/L, p < 0.001), elevated total bilirubin (median 34.95 vs. 23.00 mmol/L, p = 0.034), and lower albumin (median 29.15 vs. 34.4 g/L, p < 0.001) levels. Finally, readmitted patients had significantly lower ΔCTP scores (p = 0.003) compared with non-readmitted patients. There were no significant differences observed between the groups for platelet count, ALT, AST, ALP, GGT, creatinine, or change in MELD-Na score.
Univariate relationship between laboratory parameters at discharge during index hospitalization and 90-day readmission in patients with cirrhosis and ascites.

WBC, white blood cells; PLT, platelets; CRP, C-reactive protein; INR, international normalized ratio; TB, total bilirubin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; GGT, γ-glutamyl transferase; ALB, albumin; MELD, Model for End-Stage Liver Disease; Na, sodium; CTP, Child–Turcotte–Pugh; SD, standard deviation.
Multivariate analyses
In the univariate analyses, 17 clinically relevant variables with p < 0.1 were identified as candidates for inclusion in the multivariate model. After adjusting for other variables, multivariate regression analysis indicated that reduced hemoglobin (odds ratio [OR] 0.96, 95% confidence interval [CI] 0.94–0.97; p < 0.001) and serum albumin (OR 0.88, 95% CI 0.83–0.93; p < 0.001), and higher MELD-Na score (OR 1.04, 95% CI 1.01–1.07; p = 0.021) at discharge, were independent risk factors for 90-day hospital readmission (Table 3).
Multivariate analysis of risk factors for cirrhosis-related readmission among patients with cirrhosis and ascites.

CRP, C-reactive protein; INR, international normalized ratio; ALB, albumin; CTP, Child–Turcotte–Pugh; MELD, Model for End-Stage Liver Disease; Na, sodium; CI, confidence interval.
Discussion
The primary aim of this investigation was to elucidate the potential factors associated with 90-day readmission in patients with cirrhosis and ascites. The results of this study provide several key insights into this problem. Our findings indicated that the duration of the index hospitalization, lower levels of hemoglobin and serum albumin, and cirrhosis with alcohol and unknown etiologies were independent risk factors for 90-day readmission in patients with cirrhosis and ascites. A decrease in hemoglobin and albumin levels was associated with 4% and 8% higher odds of readmission, respectively.
In this investigation, we found a 90-day readmission rate of 43% among patients with cirrhosis who had ascites, consistent with the high readmission rate among patients with cirrhosis reported in the literature.11,12,15,19,20,27,28 The finding of this research underscores the complexity and challenges of managing this patient population, particularly in the post-discharge period. Therefore, strategies to reduce this high rate are urgently required. It is noteworthy that the duration of the index hospitalization was a determining factor for readmission. This could indicate that patients with longer initial hospital stays might experience more severe symptoms or complications that necessitate their return to the hospital, increasing the likelihood of readmission.
Regarding laboratory parameters, several markers of inflammation, liver dysfunction, and coagulation were significantly associated with readmission. These include hemoglobin level, neutrophil count, CRP, INR, D-dimer, total bilirubin, serum sodium and albumin, and CTP score at discharge. These data are consistent with those of other studies reporting similar associations.11–14,18,20,21,27,28 These laboratory parameters could serve as potential predictors of the risk for readmission to help guide post-discharge management strategies aimed at reducing hospital readmissions.
Multivariate assessment revealed that reduced hemoglobin and serum albumin at discharge as well as increased MELD-Na score were independent predictors of 90-day readmission, consistent with the literature.13,19,21 Identifying these independent predictors could help in risk stratification and developing targeted interventions to decrease the readmission rate in this high-risk patient population. Specifically, reduced hemoglobin levels could be indicative of variceal bleeding or hypersplenism, which are complications of portal hypertension in advanced liver disease, leading to increased readmission rates. Additionally, it has been hypothesized that lower serum albumin levels not only reflect liver synthetic dysfunction but also malnutrition and a more pronounced systemic inflammatory response, which are associated with poorer outcomes and increased health care utilization. The MELD-Na score has been identified as an independent risk factor for readmission in multiple studies;11–13,15,21,28,29 this score reflects the severity of liver disease and the patient’s overall prognosis. The MELD-Na score is often used to prioritize candidates for liver transplantation, which inherently poses a greater risk of complications requiring readmission.
This investigation elucidated behavioral, social, and economic predictors of readmission risk. However, in contrast to other studies investigating the role of medical insurance, sex, or smoking and drinking in the readmission risk of patients with cirrhosis,13,14,20,28,30 no relationship was observed between medical insurance and risk of readmission in patients with cirrhosis and ascites. One potential interpretation of this is that our study was performed in an Asian population with lifestyles that differ from those of other racial and ethnic groups. Additionally, nearly all Chinese citizens have medical insurance that is supported by the government. Although 32.63% of patients paid for their medical expenses themselves, none of these patients were residents of Shanghai and did not worry about the medical expense.
Despite our study data, hospital readmission in patients with cirrhosis remains a complex issue with multiple contributing factors. As suggested in other studies,8–10 a comprehensive approach, including medical management optimization, close post-discharge follow-up, patient education, and multidisciplinary care coordination, may be required to effectively reduce readmissions in this patient population.
Some limitations in the present research should be noted. First, although sufficient for multivariate analysis, the sample size of 265 patients is still relatively small. A larger cohort could provide greater statistical power. The single-center design also limits generalizability to other populations. Moreover, including multiple hospitals could also improve the external validity of the findings. Second, owing to the study’s retrospective nature, social factors affecting readmission including financial status and social support, among others, were not assessed and should be addressed in future prospective research. Third, the retrospective nature of this study means that causality between the identified risk factors and readmission outcomes cannot be definitively established. Fourth, we did not record the number of readmissions, which did not allow us to explore risk factors for patients with fewer versus more readmissions. A prospective dataset is needed to identify not only patients at risk for readmission but also those at risk for multiple readmissions. Fifth, this study was performed at a single center in China, with most patients in this relatively small sample having cirrhosis associated with autoimmune liver disease. The main cause of cirrhosis in China is HBV infection. 31 Prospective multicenter datasets are needed to explore risk factors for readmission among patients with cirrhosis and ascites that is mainly caused by HBV infection, which is more applicable to other Chinese populations.
Overall, the present research provides evidence highlighting the high hospital readmission rate among patients with cirrhosis and ascites and the potential predictors of readmission. Further studies are needed to develop and evaluate interventions to reduce readmissions in this high-risk patient population.
Footnotes
Acknowledgements
We thank all of the participants for their contributions to this study.
Authors’ contributions
CFR conceived and designed the study. NL, MX, SYL, and MQY collected and reviewed the data. SYL and MQY collated the data, and NL and MX analyzed the data. NL and MX wrote the manuscript, and NL, MX, and CFR revised the manuscript. XBL extensively edited the manuscript. All authors reviewed and approved the final manuscript for submission. All authors were involved in data acquisition, the general design of the trial, interpretation of the data, and critical revision of the manuscript. We ensured that all the authors had access to all the raw datasets. NL, MX, and CFR have verified the data; all of these authors are independent of any company or investor. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Data availability statement
The data supporting this study’s findings are available on request from the corresponding author.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study received funding from the 2023 Nursing Clinical Project (hlbynkt2023-001).