
Abstract
Musculoskeletal injury (MSI) is a multifactorial occupational health problem affecting sonographers. Potential contributing factors to the development of MSI include the repetitive motion involved in the practice of diagnostic medical sonography, the design of the ultrasound equipment and workstations, patient volume, and sonographer work practices. This descriptive feasibility study evaluated the factors influencing sonographers’ use of self-protective scanning practices and was informed by some isolated constructs of the health belief model. Scanning practices, attitudes, and beliefs about MSI were collected in surveys before and after an educational seminar about MSI. The instrument that was developed can now be used for a larger data collection on this topic. Areas that remain to be addressed by the instrument include barriers to the adoption of self-protective scanning practices and the role self-efficacy in MSI prevention.
Work-related upper extremity musculoskeletal disorders associated with repeated trauma account for more than 60% of all newly reported occupational illness, according to the U.S. Department of Labor. 1 Work-related musculoskeletal disorders are likely attributed to musculoskeletal injuries, cumulative trauma disorders, repetitive motion disorders, occupational overuse syndromes, repetitive strain injury, and occupational cervicobrachial disorders. These disorders include chronic tendinitis, epicondylitis, back pain, nerve entrapment syndromes such as carpal tunnel syndrome, and neurovascular disorders such as thoracic outlet syndrome.1,2 Activities associated with subsequent development of these disorders include static or awkward postures, forceful or repetitive exertion, and vibration. 1 Repetitive motion associated with the practice of diagnostic medical sonography is considered a key factor that can increase the risk for sonographers to incur a musculoskeletal injury (MSI). Musculoskeletal injury disorders among sonographers have been estimated nationally and as high as 91% regionally in the United States.3,4 The anatomic areas most often involved in sonographer MSI are shoulder (84%), neck (83%), wrist (61%), back (58%), and hands (56%).4,5
Other health professions have been studied with regard to MSI. Nurses and physical therapists have been studied.6–8 In a study of physical therapists, lifetime prevalence of MSI is 91%. 8 MSI is related to factors in addition to repetitive motion. Psychosocial factors, such as job dissatisfaction, have been linked to MSI.3,9 Systemic diseases, such as diabetes mellitus, gout, arthritis, and lupus, can affect the risk of developing MSI. 10 Risk for MSI also varies with age, gender, socioeconomic status, smoking behavior, and obesity status. 11 The use of antibiotics in the group known as fluoroquinolones, such as ciprofloxacin and ofloxacin, have been linked to increased risk of tendon rupture and are being investigated in relationship to MSI.11,12
Information regarding the prevalence and prevention of MSI among sonographers has been disseminated in the sonography literature for two decades.2,3,13 Sonographers can minimize their risk of developing MSI with a combination of an ergonomic workstation, proper body positioning, and administrative controls, such as scheduling and job rotation. 14 The previously mentioned study of physical therapists evaluated the use of self-protective behaviors to reduce work-related strain on their bodies. In the study reported by Cromie et al., 8 88.7% of physical therapists reported responses of “almost always” to using at least one preventive self-protective behavior while working with patients. No such data have been located in the literature regarding what percentage of sonographers report utilizing self-protective scanning practices. Even with increasing evidence that points to methods for risk reduction, a lack of research exists that defines or explains what factors impact a sonographer’s choice to minimize personal risk for MSI.
Related Theory
Several theoretical models of health behavior have been applied to injury prevention; unfortunately, occupational injuries have not been specifically addressed.15,16 According to DeJoy, 17 the application of health behavior models and “research on workplace self-protective behavior has been piecemeal and atheoretical.” Studies on workplace self-protective behavior have typically focused on employee characteristics, behavior modification through reinforcement or operant-based approaches, and organizational and environmental correlates of good safety performance. 17 Several health behavior models are applicable to self-protective workplace practices and behavior.
Value-expectancy models of health behavior are based on the idea that an individual estimates the seriousness of the risks, evaluates the costs and benefits of various actions, and then chooses a course of action that will maximize the expected outcome. One such value-expectancy model is the health belief model (HBM). The HBM is an explanatory model of individual health behavior that was developed by in the 1950s by Hochbaum and the United States Public Health Service. 18 The HBM states that individuals will modify personal behavior when they perceive that a condition is severe or that they are susceptible to the condition. Severity in the HBM is the seriousness of a condition and its sequelae in terms of both medical and social consequences. Susceptibility is defined as an individual’s subjective assessment of the risk of developing or contracting a health condition. 18 The combination of perceived severity and susceptibility is sometimes referred to as “perceived threat.” 18 The benefits versus cost of adopting a particular behavior are factored into decision making, although perceived susceptibility has been shown to be more important in preventive behavior than perceived benefits. Modifying factors of behavior include individual characteristics and cues to action that can prompt an individual to adopt a health behavior (Figure 1). Cues to action can include bodily events or environmental events and have not been well studied empirically. 18 Perceived barriers to taking action are also inherent in the HBM. The variables in the HBM can be added or combined in a linear fashion to test the model: Susceptibility + Severity + (Benefits – Barriers). Perceived barriers have been shown to be the most powerful single predictor of behavior across all behaviors and all studies. 17
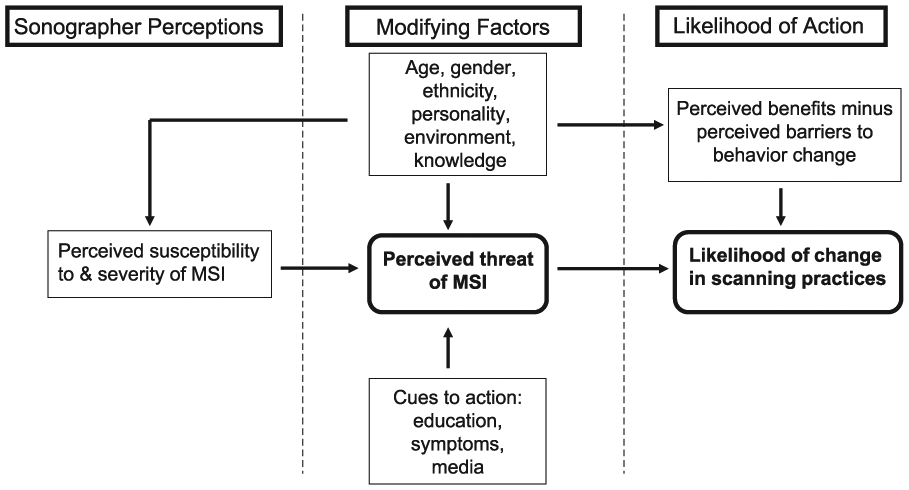
Health belief model: sonographer scanning practices and musculoskeletal injury.
In recent years, the concept of self-efficacy has been added to the HBM. Self-efficacy was taken from Bandura’s work on social learning theory and is the conviction within the client that he or she can successfully perform the suggested health behavior to achieve a successful outcome. 15 Self-efficacy has been shown to be especially important for behaviors involving lifestyle changes that involve long-term modification and maintenance. 17
The health belief model is an appropriate model to describe factors influencing sonographer adaptation in scanning practices with regard to MSI. Disseminating information to sonographers about MSI is important, but application of this information to everyday sonographic practice is crucial. This study was performed to better understand the factors affecting sonographers’ adaptation of scanning practices as a function of their perception of the severity of and susceptibility to MSI. The primary research question that was established for this study was the following: Does a sonographer’s perception of susceptibility to or severity of MSI influence adoption of self-protective scanning practices?
Additional research question that were posed included: Does pain elicited from scanning provide a cue to adopting self-protective scanning practices? Does education about MSI serve as a modifying factor in the sonographer’s perceived threat of MSI?
Materials and Methods
A pre-experimental, pretest/posttest designed project was approved by the Institutional Review Board at Kent State University. This feasibility study was performed in northeastern Ohio. The location was accessible to the researcher for travel to present the educational component of the project. The setting included a total of seven sonographic laboratories within large and small facilities in which a variety of different sonographic examinations were performed (i.e., general, OB/GYN, vascular, cardiac). A convenience sampling method was employed, based on agreement by the sonographic laboratories to allow staff to be available for one hour. Thirty sonographers completed the initial survey. Follow-up surveys were returned by 27 of the 30 sonographers, for a response rate of 90%. The data from the initial survey completed by three sonographers who did not complete the follow-up were excluded from the data analysis.
The survey items were reviewed by two content experts in the area of musculoskeletal injury in sonographers, Carolyn Coffin and Joan Baker. These reviewers identified 34 questions out of the 40 survey items that had been asked in various formats in previous research studies. This review was performed to establish content validity. The first 10 respondents were enrolled and participated in the educational seminar in a single session to establish readability and construct validity. After completion of the initial survey and seminar, feedback was sought in a focus group format to gather additional information from the participants. As a result of these discussions and the careful review of the participants’ use of the survey, minor format changes of survey instrument were made, with checkboxes converted to a table. The survey content was not changed; therefore, face validity was established.
The designed intervention was an educational seminar on MSI. After obtaining signed informed consent, the participants completed a survey (referred to as “initial survey”). This survey instrument consisted of four parts: demographic information, current scanning practices, attitudes and beliefs about MSI, and personal experience with and education about MSI. Demographic information collected included age, gender, type of sonography education, length of scanning experience, and registry and employment status.
Information about scanning practices was divided into availability of ergonomic features and equipment and use of such features and equipment. The responses were given in choices of percentages (i.e., 0%, 1%–25%, 36%–50%, 51%–75%, 76%–99%, and 100% of time). The availability and use of the following features and equipment were assessed: adjustable height scan, sonography scanning chair, adjustable height keyboard, adjustable height monitor, preprogrammed image annotation, voice scan technology, patient positioning devices (e.g., wedges and sponges), and adaptive devices (e.g., arm rests and cable braces). A question was asked regarding how often the sonographer consciously adjusts scanning practices for ergonomic considerations, with the same percentage choices for responses. The percentage of procedures performed as portable/mobile examinations per day and the types of sonographic equipment by manufacturer/platform were also asked about.
Questions regarding sonographers’ knowledge and beliefs about MSI were anchored with a 5-point Likert response from strongly disagree (1) to strongly agree (5) and a don’t know/unsure response option. The following statements were used to assess the construct of perceived severity of MSI in sonography:
I believe that MSI is a problem for the sonography profession.
I know a sonographer who has been affected by MSI.
Perceived susceptibility was considered with the following statements:
I believe MSI is a problem or potential problem for me personally as a sonographer.
I have been affected by MSI related to scanning.
One potential cue to action that was queried was pain. The following statements were used to assess the respondents’ pain related to scanning:
I usually have pain while scanning.
I usually have pain after scanning.
Additional information concerning personal experience with MSI symptoms was assessed by questions regarding sites of pain during or after scanning and whether or not treatment had been sought for pain. The other potential cue to action considered was education. The respondents were asked if MSI was part of their sonography education and if they had undergone any previous educational presentations on the topic of MSI. A space for additional respondent comments was included.
After survey completion, the participants attended a one-hour educational session about MSI and its prevention. This educational activity was a combined lecture and videotape presentation. The videotape, commercially available through Biodex, Inc., provided information about risk factors for MSI, proper ergonomic scanning practices with demonstration, and active learning by the use of stretching exercises. All participants performed the stretching exercises during the presentation. Information regarding the prevalence of MSI, proper ergonomic scanning practices, and suggested adjustments to scanning techniques was given in lecture and handout format. Each participant earned one hour of Society of Diagnostic Medical Sonography (SDMS) approved CME credit on completion of the educational session. Each participant was given a cable brace, which is a sonography-specific adaptive device with a Velcro strap that can be placed on the scanning arm to reduce wrist strain while scanning.
Each participant was mailed a follow-up survey 21 days after the educational session. The follow-up survey consisted of the same questions in the same format without repeating questions regarding demographic information or particular manufacturers of sonographic equipment used in practice. Respondents were asked to return the survey within one week after receipt. Every sonographer who returned the follow-up survey was entered into a drawing for two $25 gas cards as an incentive to increase response rate.
Results
All respondents signed an informed consent prior to participation. The sample consisted of 30 sonographers from northeastern Ohio. The sonographers in the sample were recruited and enrolled during a total of seven educational seminars held at the ultrasound laboratories. The clinical practice settings included ultrasound laboratories within radiology departments at community and teaching hospitals, an outpatient imaging center, and a perinatal physicians’ office. Twenty-seven valid responses were analyzed using SPSS for Windows 21.0. Cronbach’s alpha for the survey items relating to attitudes and beliefs about MSI was calculated as 0.85.
Data collected are provided with the demographics for respondents summarized in Table 1. All respondents are currently working in the field of sonography (77.8% employed full-time and 22.2% part-time). The average number of hours worked per week was 35.75 on the initial survey (range, 19–56) and 35.72 on the follow up survey (range, 15–48). The number of hours worked per day was 8.68 on the initial survey and 8.48 on the follow-up survey. The average number of patients scanned per day by the sonographer was reported as 10.57 (range, 7–14) on the initial survey and 11.27 (range, 4–17.5) on the follow-up survey.
Respondent Demographics.
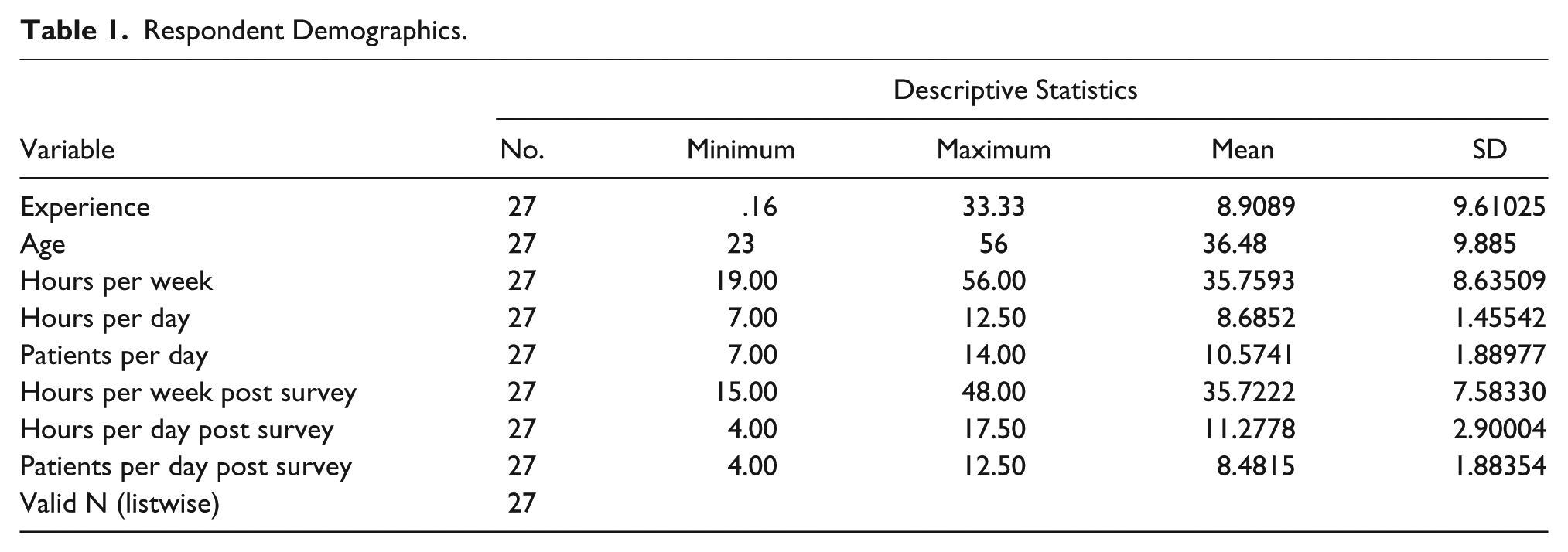
With regard to registry status, 74.1% of the respondents are registered in at least one specialty area by American Registry of Diagnostic Medical Sonography (ARDMS), and 25.9% are not registered. None of the sonographers reported holding sonography certifications from any organizations other than the ARDMS. The mean age of the respondents was 36.4 years (SD = 9.88; range, 23–56 years). The average length of scanning experience was 8.9 years (SD = 9.61; range, 1 month–33.33 years). Twenty-five respondents (92.6%) were female, with the remaining two sonographers being male. Over half of the respondents (55.6%) reported that MSI prevention was part of their sonography education, and 33.3% responded that they had previously attended an educational seminar on the topic of MSI.
Paired sample t tests were used to evaluate for significant differences between initial survey and follow-up survey item responses (significance P < .05). The responses for the items relating to sonographer scanning practices were given in average percentage of time the respondent used a particular self-protective or ergonomic feature or scanning practice. The responses were coded as follows: 0% = 0, 1% to 25% = 1, 26% to 50% = 2, 51% to 75% = 3, 76% to 99% = 4, and 100% of the time = 5. The majority of responses showed slight changes in the numeric mean. No statistically significant changes in use of height-adjustable stretcher (P = .147), height-adjustable chair (P = .717), adaptive devices (P = .158), and adjustable keyboard (P = .364) were reported. Statistically significant changes were noted in the use of preprogrammed image annotation (P = .00), patient positioning devices (sponges, wedges, etc.) (P = .028), and height-adjustable monitors (P = .012).
Small differences were also noted in the sonographer attitudes/beliefs about MSI (Figure 2). There were slight increases in mean scores from initial survey to follow-up survey for five of the six items. Increases in the mean scores were noted for the questions regarding perceived severity of MSI. The first item that related to susceptibility had a slight decrease in mean score from the initial to follow-up surveys. The item, which read “I believe MSI is a problem or potential problem for me personally as a sonographer,” had a mean score of 4.37 on the initial survey and a mean score of 4.30 on the follow-up survey. The decrease did not change the overall response category, which remained in the agree category. The only item in the sonographer attitudes and beliefs section that had a change in response category based on mean score on the follow-up survey was “I usually have pain while scanning.” The mean score for this item on the initial survey was 2.85 (in the disagree category), and the mean score on the follow-up survey was 3.0 (neither agree nor disagree). The P values for all items related to sonographer attitudes/beliefs were greater than .05, and therefore no statistically significant change in attitudes occurred between pretest and posttest evaluation.
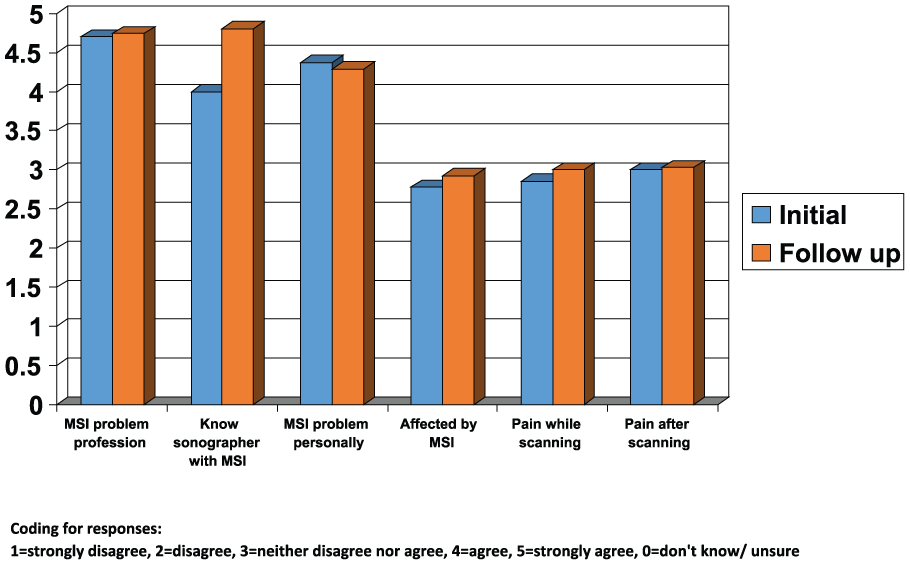
Sonographer beliefs/attitudes about musculoskeletal injury.
The survey item designed to assess the likelihood of using self-protective scanning practices, based on the perceived threat of MSI, asked how often the sonographer consciously adjusts scanning practices for ergonomic considerations. This question had responses in choices of groups of percentages (i.e., 0%, 1%–25%, etc.). The percentages were coded for data entry as 0% = 0, 1% to 25% = 1, 26% to 50% = 2, 51% to 75% = 3, 76% to 99% = 4, and 100% of the time = 5. The mean score on the initial survey for how often the sonographer consciously adjusts scanning practices was 2.62, and the mean score on the follow-up survey was 2.92. While the mean score increased slightly for the follow-up evaluation, the P value was .411, indicating that the slight increase numerically was not statistically significant.
Discussion
The main focus of this research was to develop a reliable survey instrument that addresses MSI among practicing sonographers. A calculated coefficient of 0.8 indicates a highly reliable instrument that is ready for greater application. The pilot data provided some interesting results, and these are discussed relative to their descriptive nature. The mean scores in the scanning practices section of the survey increased in seven of the nine areas. The increases were modest, however, and the majority of the increases did not equate to a statistically significant change in the percentage of time respondents reported using specific ergonomics features or devices. Statistically significant changes were noted in the use of preprogrammed image annotation, patient positioning devices, and the use of height-adjustable monitors.
Overall, the mean responses for the sonographer attitudes/beliefs section increased at least minimally between the initial and follow-up surveys. The mean scores indicate that the respondents agree that MSI is a problem for the profession and know a sonographer who has been affected by MSI. The item stating “I believe MSI is a problem or potential problem for me personally as a sonographer” had a mean score of 4.37 on the initial survey and a mean score of 4.30 on the follow-up survey. Both of these means fall within the response category of agree. The P value was .663, indicating no statistical significance. This particular item was used to assess respondents’ perception of susceptibility to MSI. Susceptibility is the major factor that affects preventive behavior in the health belief model. The only item for which the change in mean scores affected the response category was the item that reflected pain while scanning. The mean score for the initial survey was 2.85, which is in the disagree category. The mean score for the follow-up survey was 3.00, which falls in the neither agree nor disagree category. It is possible that the respondents became more aware of pain while scanning after the seminar. The mean number of patients scanned per day reported increased from 10.57 on the initial survey to 11.27 on the follow-up survey, which may be another explanation for the awareness of pain while scanning.
The intent of the educational seminar was to elicit a cue to action. The mean scores for the percentage of time the respondents consciously adjusted scanning practices for ergonomics increased slightly but did not change the overall category of percentage of time. Cues to action are difficult to quantify. Another cue to action for sonographers may be pain related to scanning. On the follow-up survey, 16 of the 27 respondents (59.2%) reported having pain at least 50% of the time related to scanning. Of the sonographers who reported pain related to scanning, the mean score for percentage of time scanning practices were adjusted for ergonomics was 3.12 (51%–75% of time). For the remaining 11 respondents who reported having pain related to scanning less than 50% of the time, the mean percentage of time scanning techniques were consciously adjusted for ergonomics was 2.63 (26%–50% of time). Sonographers need to be educated on biofeedback from their bodies while scanning and how to use this information as cues to action.
Limitations
The survey instrument did not have questions that specifically asked about barriers to adoption of self-protective scanning practices. With a larger sample using this survey instrument in its current form, barriers may be implied due to number of patients scanned per day, percentage of workload performed as portable/mobile sonography, and/or types of sonographic and adaptive equipment available. A series of questions to measure barriers would be important for continued research, and an example question might be, “What barriers do you feel you face in your ability to protect yourself from MSI?” As mentioned previously, barriers to action are the single best predictor of health behavior. Research has shown that job-related barriers are often a major factor in noncompliance with use of personal protective equipment. 17 In reviewing respondent comments on the initial and follow-up surveys, some examples of potential barriers were provided. Barriers for these respondents included scheduling, job type, and job rotation. Lack of available ergonomic equipment was noted to be a problem on portable examinations in some facilities and has been a historical problem for sonographers who have been scanning for many years.
Another construct that needs to be addressed in the survey instrument is self-efficacy. The construct of self-efficacy is important in the HBM because it serves as a prerequisite to behavior change. Self-efficacy is vital in long-term behavior change and maintenance. A method to improve self-efficacy in proper ergonomic scanning would be the use of a hands-on training session using scanning practices instead of videotape. In the current study, passive learning for scanning techniques was provided through the use of the videotape. Active learning was used for stretching, as the participants were asked to stand and practice stretches several times throughout the tape. Several comments about stretching were recorded in the comments section on the follow-up surveys. Respondents noted that they were using the stretches and felt stretching was helpful in reduction of pain related to scanning.
Another potential area where self-efficacy could have been assessed in the current study relates to the cable braces participants received during the educational seminar. During the videotape, proper use of cable braces was demonstrated. These Velcro straps are placed on the forearm, and the transducer cable is attached to the strap to reduce strain from the weight of the cable. The cable braces were distributed at that point in the videotape but were not used with actual sonographic equipment during the seminar. A question could have been posed in the follow-up survey instrument to assess the sonographer’s confidence in using the cable brace properly.
Characteristics of the sample, such as the distribution of gender and number of patients scanned per day, are similar to results from large studies of several thousand sonographers previously reported.19,20 Threats to internal validity are history, maturation, testing, instrumentation, regression, and interaction of selection and maturation. Threats handled by this design are selection and mortality. Distribution of cable braces to participants represented a potential threat to internal validity of the study in the form of a threat to history. The interval between the initial and follow-up surveys was three weeks, representing threat secondary to maturation. The survey instrument remained the same for the initial and follow-up surveys, posing no apparent threat to instrumentation. External threats to validity are not controlled; therefore, no generalizations can be made from this data collection. A larger sample would allow for regression techniques to be used to evaluate multiple factors that may influence a sonographer’s use of self-protective behaviors while scanning.
Conclusions
A reliable survey instrument was developed for use in measuring some of the constructs of the HBM as they relate to MSI among practicing sonographers. The respondents in this descriptive study recognized the problem of musculoskeletal injury but self-reported an inability to adjust to ergonomic scanning practices during their clinical practice. Increasing sonographer awareness of susceptibility to MSI may be important in the context of the health belief model to assist sonographers in adopting self-protective scanning practices as a long-term behavioral change. Inclusion of additional areas of the HBM may be important to better capture the multifactorial nature of MSI. Inclusion of survey questions that address the identification of barriers and the concept of self-efficacy in the adoption of self-protective scanning behaviors will be critical in the further use of this instrument.
Footnotes
Acknowledgements
The authors gratefully recognize Carolyn Coffin, MPH, RDMS, RDCS, RVT, FSDMS, and Joan Baker, MSR, RDMS, RDCS, FSDMS, for their willingness to share their knowledge in the field of ergonomics and their careful review of the survey instrument.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.