
Abstract
Distal intersection syndrome is the tenosynovitis of the second compartment and the third compartment, at their cross point, in the dorsal wrist. It is a rare disorder presenting with pain, swelling, and tenderness in Lister’s tubercle area of the wrist. One of the causes may be the pulley effect of Lister’s tubercle on the third compartment, where the resultant tenosynovitis can spread to the second compartment through their communication foramen. This case of distal intersection syndrome is induced by hyperflexion and abduction injury of the thumb, which may have caused tenosynovitis of the third compartment by overstretching over Lister’s tubercle. It is unique that in addition to the typical presentation of the syndrome with tenosynovitis of the second and third compartments, the fourth compartment also displayed tenosynovitis. This extra presentation may result from the possible communication between the third and fourth compartments.
Introduction
The tendons that extend the wrist and fingers are held in place on the dorsal wrist by the extensor retinaculum. This ligament attaches to numerous bony landmarks around the dorsal wrist, creating six compartments; each compartment holds various tendons. Whereas the majority of tendons travel in a direct path through the forearm into the wrist, the tendons within the first and third compartments travel at an angle as they cross the wrist to insert into the thumb. To arrive at the thumb, these tendons in the two compartments must cross over the top of the tendons in the second compartment. These intersection points are prone to becoming irritated, resulting in inflammation of the sheath around the tendons (i.e., tenosynovitis), more commonly diagnosed as proximal and distal intersection syndrome.1,2
The second compartment is located near the radial aspect. It contains the tendons of the extensor carpi radialis brevis and the extensor carpi radialis longus. The extensor carpi radialis brevis originates from the lateral epicondyle of the humerus via the common extensor tendon, whereas the extensor carpi radialis longus originates directly from the lateral supracondyle. They run side by side in the deep portion of the forearm, join and travel in the second compartment, and insert into the base of the second and third metacarpals.
This compartment is first crossed over from ulnar to radial by the musculotendinous junctions of the extensor pollicis brevis and abductor pollicis longus from the first compartment at an angle of 60 degrees at about 4 cm proximal to the Lister’s tubercle of the wrist2,3 (Figure 1). This intersection of the first compartment and the second compartment is the proximal intersection. As the tendons of the second compartment extend further distally, they pass radial to Lister’s tubercle, in the proximal wrist. At the same level, the tendon of the extensor pollicis longus in the third compartment passes ulnar to Lister’s tubercle. The extensor pollicis longus muscle originates from the middle third of the posterior ulna and adjacent interosseous membrane and travels parallel to the tendons in the second compartment in through the forearm. As the tendons in the two compartments extend distally, the tendon in the third compartment turns at Lister’s tubercle and crosses over the second compartment to insert into the distal phalanx of the thumb (Figure 1). This intersection of the second compartment and the third compartment is the distal intersection. 2
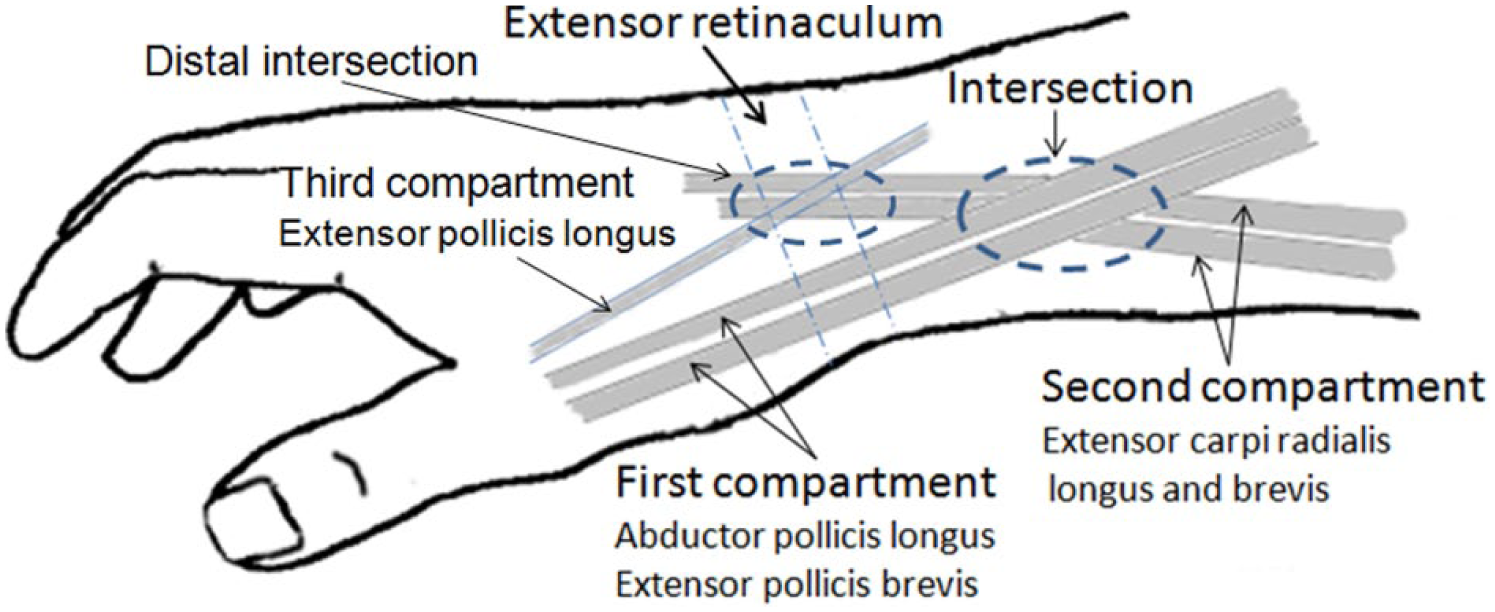
The anatomy of the (proximal) intersection and the distal intersection in the dorsal forearm and the wrist.
Clinically, intersection syndrome presents with pain, swelling, and tenderness at the point of the intersection. This occurs just proximal to the wrist for a proximal syndrome and in the area of Lister’s tubercle, in the dorsal wrist, for a distal syndrome. Proximal intersection syndrome, most often referred to as just intersection syndrome, has an incidence rate between 0.20% and 0.37% in the general population3,4 and 1.9% in hand and wrist patients. 5 The incidence rate of distal intersection syndrome is even lower—around 0.3% in hand and wrist patients. 5 The characteristic pathology of distal intersection syndrome is tenosynovitis in the second and third compartments. 1 The following report describes a case of distal intersection syndrome with unique pathologic presentation, in which tenosynovitis was present not only in the second and third compartments but also in the fourth compartment.
Patient Case
A 30-year-old female was referred for a sonographic examination due to left dorsal wrist swelling and pain. Five months prior, she lost control of a garbage bin and had her left thumb hyperflexed and abducted by the falling container. Right after this incident, the dorsal thumb was painful, and the dorsal wrist near the radial aspect started swelling and had pain. After two sessions of physical therapy, including electric stimulation and massage, the swelling and pain diminished, but any movement of the wrist or the thumb continued to cause wrist pain. In addition, the middle aspect of the dorsal wrist started swelling 4 months prior. Movement of any of the fingers caused pain in the dorsal wrist. No further treatment was given. The patient had no history of previous forearm, wrist, or systemic disease. Physical examination of the left dorsal wrist revealed obvious swelling of the radial two-thirds of the wrist. The patient reported tenderness to palpation over the area of swelling, especially in the area of Lister’s tubercle, and flexion or extension of the wrist or fingers induced pain in the dorsal wrist.
A systematic sonogram of the dorsal wrist was performed with a linear high-frequency transducer (8–17 MHz) using the Alpinion E-CUBE 9 ultrasound equipment (Alpinion Medical Systems USA, Bothell, WA). No abnormality was identified in the first, fifth, and sixth compartments. Scanning of the second compartment started from the dorsal forearm at the level of proximal intersection down to the wrist. From right distal to the proximal intersection to the ends of the separate sheath of each tendon in the compartment, the synovial sheath of the full length tendon demonstrated a thick hypoechoic area surrounding the tendons (Figure 2A, B). The third compartment had a similar appearance to the second compartment from proximal to distal intersection to distal to distal intersection (Figure 3A–E). To evaluate the vasculature in the compartments, power Doppler interrogation was applied. Mild hyperemia was displayed in the sheath of the third and second compartments (Figure 4A, B). The fourth compartment also demonstrated a thick hypoechoic area surrounding the tendons and mild hyperemia in the sheath (Figure 5A–C).
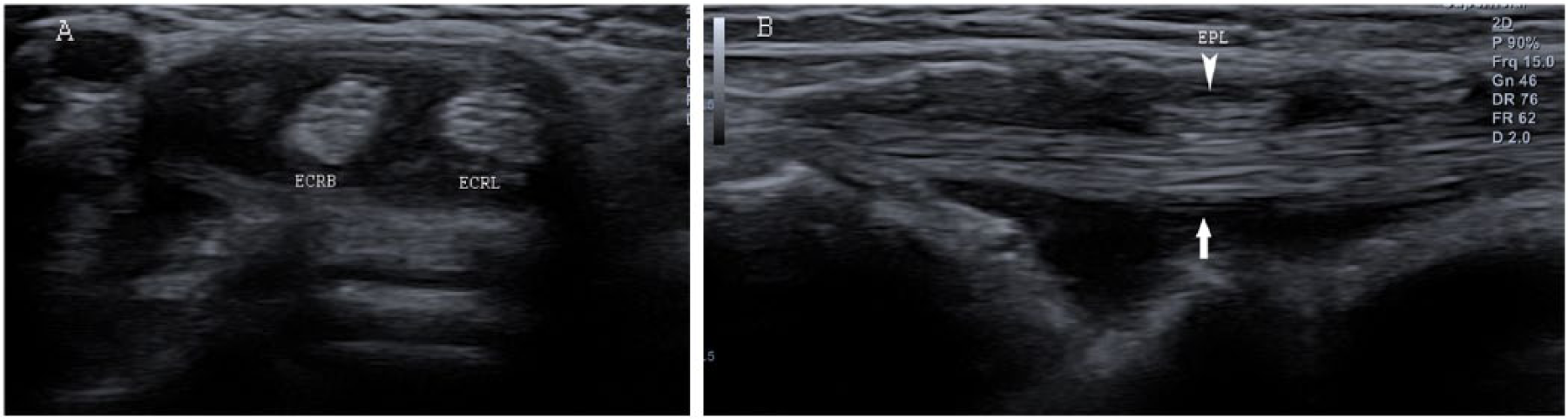
Thick hypoechoic area surrounding the tendons in the second compartment. (A) Transverse view. The tendons of the extensor carpi radialis longus (ECRL) and the extensor carpi radialis brevis (ECRB). (B) Longitudinal view. Superficial to the second compartment (arrow), the crossing third compartment (arrowhead) containing the extensor pollicis longus (EPL) can be seen.
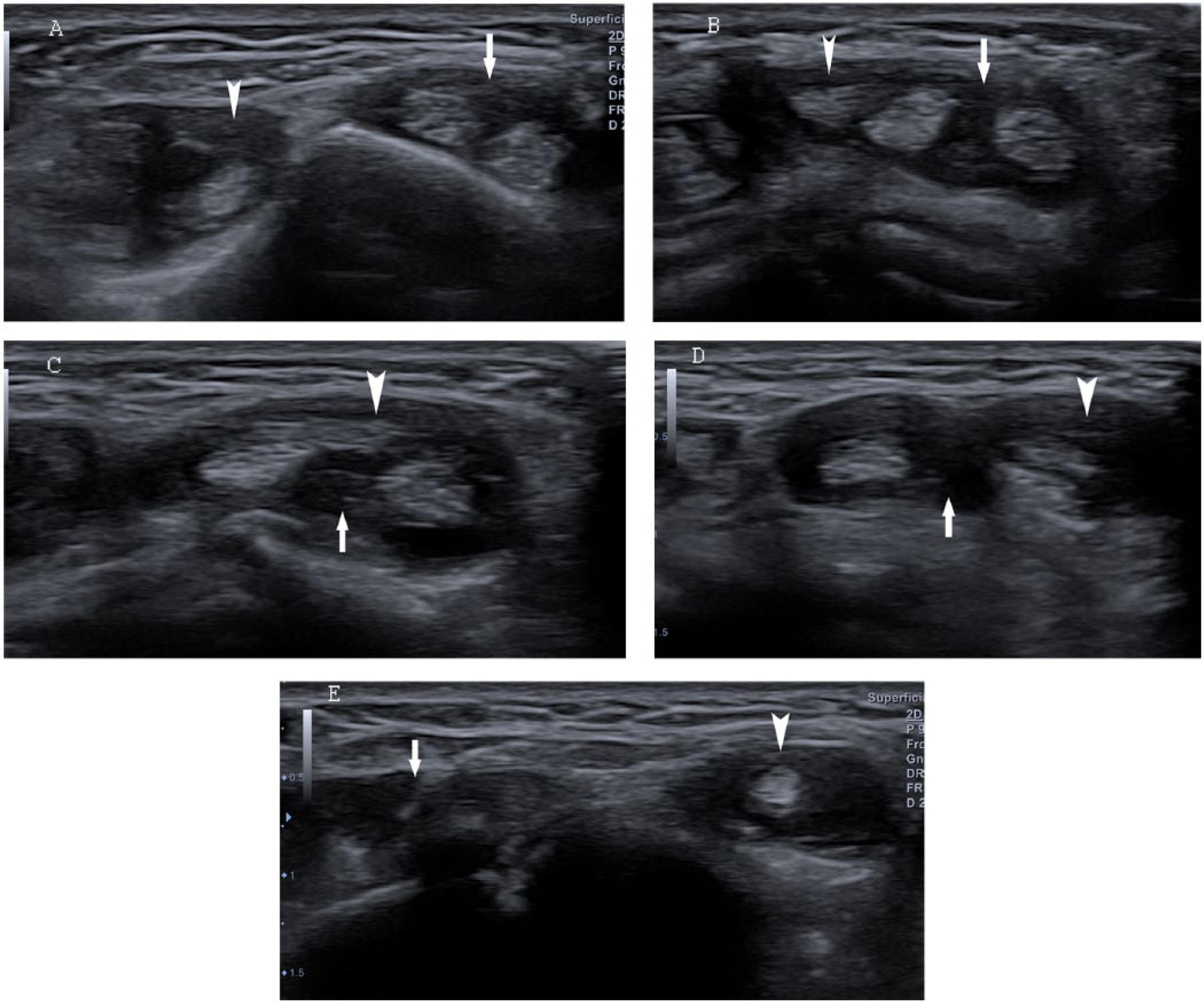
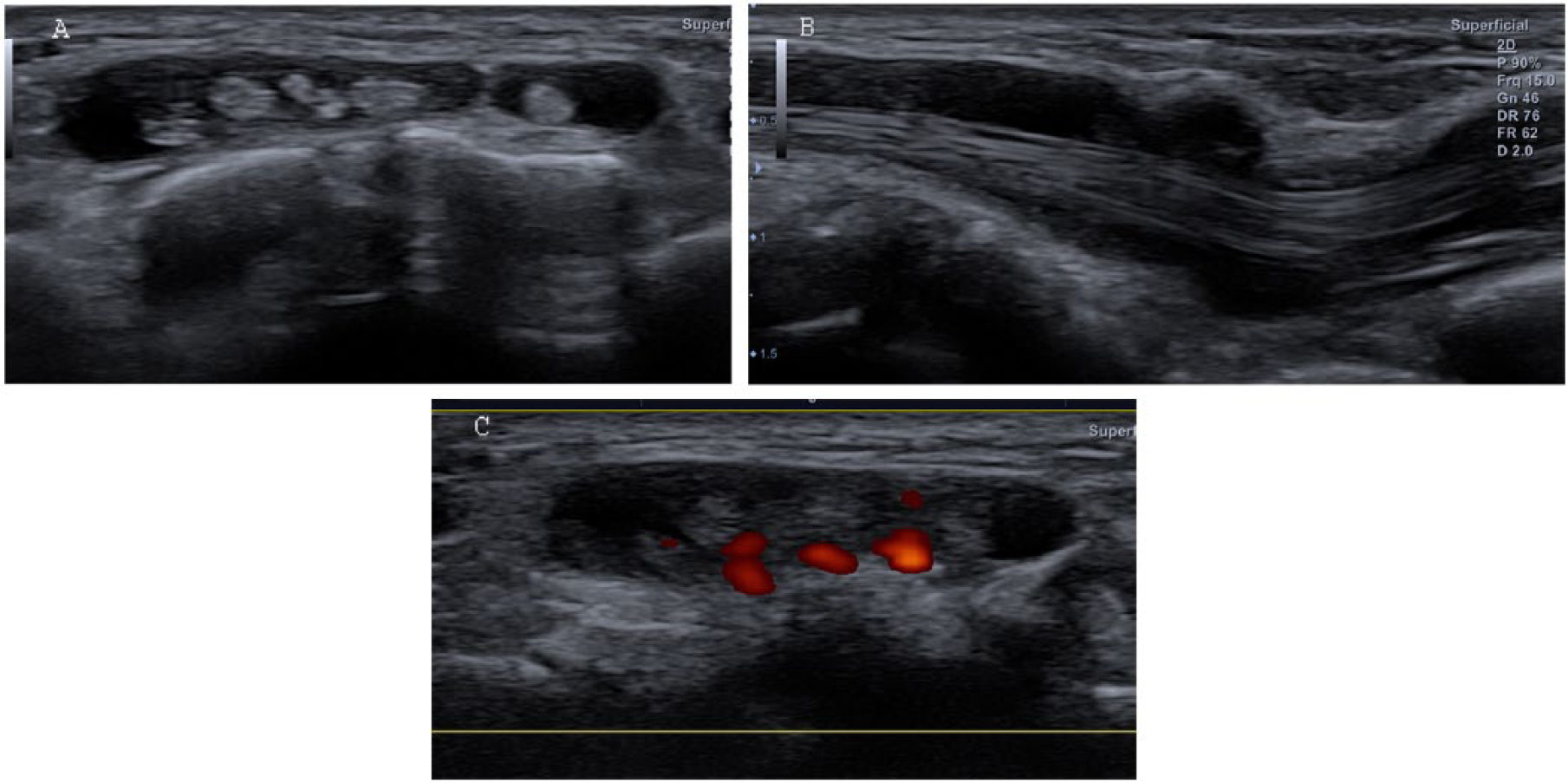
Transverse image of the distal intersection region. (A) The third compartment (arrowhead) with thick hypoechoic rim surrounding the tendon of extensor pollicis longus in the dorsal wrist ulnar to Lister’s tubercle, (B) approaching the cross point with the second compartment (arrow), (C) at the cross point, (D) leaving the cross point, and (E) after crossing.
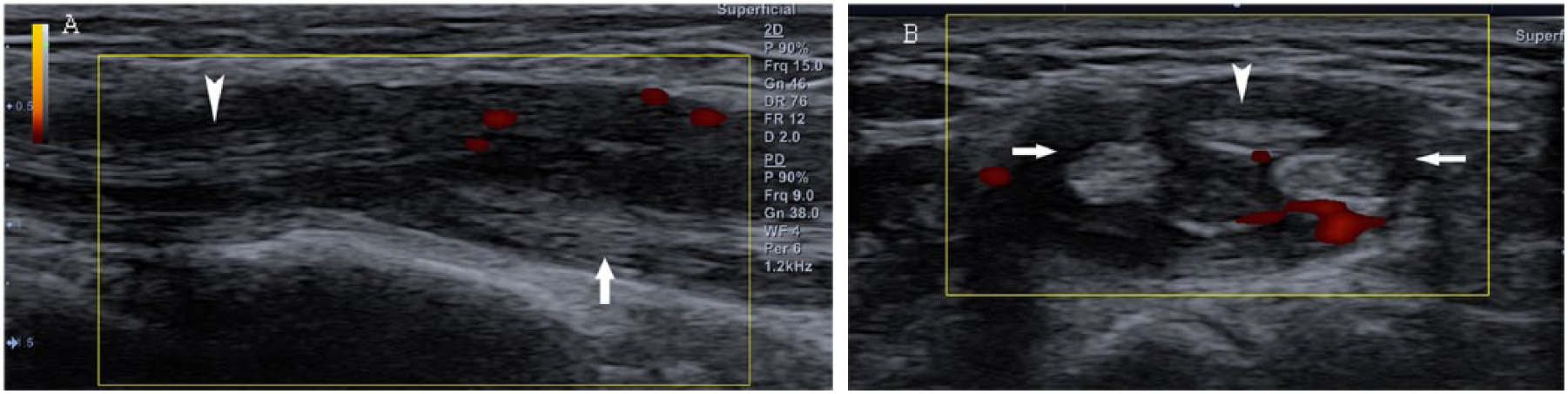
Hyperemia in the second and third compartments at the distal intersection. (A) Longitudinal power Doppler image shows vasculature in the thick hypoechoic area of the third compartment (arrowhead) crossing superficially the second compartment (arrow). (B) Transverse power Doppler image shows vasculature in the second compartment deep to the third compartment.
Thick hypoechoic area surrounding the tendons in the fourth compartment. (A) Transverse view. (B) Longitudinal view. (C) Transverse power Doppler image shows hyperemia in the fourth compartment.
Discussion
Inflammation of the synovial sheath investing the tendon is called tenosynovitis. 6 It can have many etiologies or be idiopathic. This condition is most commonly due to repetitive strain from overuse of the tendon. Another relatively common cause is arthritis (e.g., rheumatoid arthritis), which can cause inflammation of both the joint and the tendon sheath. 6 Acute tenosynovitis usually results in an abnormal amount of fluid encircling the tendon. In the subacute and chronic stages, tenosynovitis demonstrates not only increased fluid but also thickened synovium, which on gray-scale sonography appears as an increased width of peritendinous anechoic or hypoechoic rim. Thickened tendons in the sheath can also be seen in this stage. 6 Since tenosynovitis is an inflammatory condition, power Doppler demonstrated hyperemia in the rim of the sheath.
The current case demonstrated a sonographic increased width of the peritendinous hypoechoic rim and mild hyperemia in the rim in both the second and third compartments. These sonographic findings suggest tenosynovitis in the two compartments, which is the reason for swelling and tenderness in the radial third of the wrist around Lister’s tubercle. This patient’s symptoms, prolonged history, and sonographic presentation of tenosynovitis in the second and third compartments support the diagnosis of distal intersection syndrome in a chronic stage.
An additional finding that makes this case special is that the fourth compartment also displayed tenosynovitis. The tenosynovitis of all three compartments caused the radial two-thirds of the dorsal wrist in this patient to display swelling and tenderness, and any movement of the wrist or fingers to induce pain.
The wrist pain and swelling of distal intersection syndrome should be differentiated from intersection syndrome and de Quervain disease. Intersection syndrome is a local inflammatory disorder of the dorsal distal forearm at the cross point between the first compartment and the second compartment.7–9 It is usually related to acute or chronic overuse of the upper extremities, which may cause constant friction between the two compartments, leading to synovial sheath injury and followed by inflammation.7–9 Local trauma may also be a reason for the syndrome. 7 Its clinical presentation of pain, swelling, and tenderness is usually located in the dorsal distal forearm. However, some patients may also present with pain in the wrist, which is similar to distal intersection syndrome. The most common pathologic change of intersection syndrome is the tenosynovitis of the second compartment at the intersection. Sonography of intersection syndrome may include tendon thickening or tenosynovitis of the compartments, especially the second compartment.5,7–9 de Quervain disease is the pathologic condition of stenosing tenosynovitis occurring in the first dorsal compartment of the wrist. It is characterized by radiating pain on the radial side of the wrist with movement of the thumb or wrist, associated with slight swelling in the area of the radial styloid process. 10 Sonography demonstrates a thickened and hypoechoic retinaculum, synovial thickening, and effusion in the sheath of the first compartment. Occasionally, focal enlargement of the tendons can also be found. 10
The term distal intersection syndrome was first proposed by Parellada et al. 1 in 2007 based on the magnetic resonance finding of tenosynovitis centered at the cross point of the second and third compartments near Lister’s tubercle in the dorsal wrist. This syndrome may originate from the tenosynovitis of the third compartment but also possibly from the second compartment. Since the two compartments can communicate through a foramen between them, the inflammation in one compartment can spread to the other compartment.11,12 The overuse of the thumb or wrist causes constant friction at the distal intersection between the second and third compartments, which may result in tenosynovitis in the compartments. In the dorsal wrist, Lister’s tubercle serves as a pulley for the third compartment as it changes course from parallel to the second compartment to the radial aspect toward the base of the thumb. 5 The tenosynovitis of the extensor pollicis longus of the third compartment may also be caused by the attrition related to the pulley effect of Lister’s tubercle, blunt trauma, or a nearby radial fracture. 1 According to the current patient’s injury history, which had the thumb hyperflexed and abducted, the extensor pollicis longus might be overstretched over Lister’s tubercle. This may be the cause of the tenosynovitis of the third compartment. The communication between the second and third compartments might lead to the inflammation spreading from the third compartment to the second compartment. The coexisting tenosynovitis of the fourth compartment in this patient may have also been caused by the inflammation spread from the third compartment, because a communication may also exist between the fourth compartment and the third compartment. 12
The treatment of distal intersection syndrome usually starts with conservative measures, which are effective in most cases. Immobilization with a splint is a very important method of conservative treatment. 3 It eliminates the irritation arising from the friction between the two compartments. In the meantime, nonsteroidal anti-inflammatory drugs help to reduce the inflammation. Surgery is indicated only when conservative treatment fails.
Conclusion
Distal intersection syndrome is a rare disorder. The coexistence of the fourth compartment tenosynovitis with the syndrome is unique. It may originate from the tenosynovitis of the third compartment by being overstretched over Lister’s tubercle and then spread to the second and fourth compartments.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.