
Abstract
Germ cell (yolk sac) tumors are rare tumors that often have a poor prognosis because they are not usually found until metastases have occurred. The diagnosis of yolk sac tumors is usually a multimodality diagnosis in conjunction with a biopsy of the lesion. This case study outlines the initial stages of diagnosing and treating a 22-month-old male patient who was found to have a widespread malignant yolk sac tumor in his abdominopelvic cavity. Sonography was used as the primary imaging modality due to the patient’s age, but it was soon determined that a follow-up with computed tomography was necessary. Because of the complicated nature and progression of the tumor, a surgical biopsy was then performed. During the procedure, it was also noted that the mass was hypervascular with extensive blood flow throughout the mass. Excision was not an option and chemotherapy treatment was recommended.
Introduction
The prevalence of extragonadal germ cell tumors in the pediatric population is rare. Statistically, they account for less than 3% of all germ cell tumors in children less than 15 years of age, including germ cell tumors in the reproductive organs. 1 Current reported survival rates vary with the staging of the germ cell tumor. Pediatric survival rates range from 90% with a stage I germ cell tumor diagnosis to 82% survival rate with a diagnosis of stage IV germ cell tumor. 2 Sonography can be highly effective in the diagnosis of yolk sac or germ cell tumors when used in conjunction with other imaging modalities and biopsy procedures. While the etiology of yolk sac tumors is unknown, what is known is that such tumors can be malignant or benign, and consist of germ cells, which are the cells that develop in the embryo and become the cells that make up the male and female reproductive system. This case study gives details on a 22-month-old male with an extragonadal germ cell tumor and the presentation, lab values, treatment, and imaging components of this case.
Case Report
The patient presented to the emergency department (ED) with weight gain, abdominal distention, and pain for the previous five weeks. Prior to coming to the ED, the parents had consulted with their pediatrician and the patient had been treated for constipation, as it was believed to be the cause of his abdominal pain and distention.
Upon arrival at the ED, the patient was febrile and uncomfortable, but consolable. It was noted that a large, palpable mass was present within the right upper quadrant of the abdomen. Lab tests revealed that his alpha-fetoprotein (AFP) tumor markers were >150 000 ng/ml and his ferritin was 214. Both values are indicative of a malignant tumor within the body. Reference range for this pediatric population is a mean of 8ng/ml, as compared to the normal AFP reference range for men and nonpregnant women of <5.4 ng/ml. 3 If AFP rises above 500 ng/ml in the presence of a tumor, the tumor is unlikely to be benign. When levels rise above 1000 ng/ml, there is a strong correlation to hepatocellular carcinoma.
The patient was brought to the sonography department for an abdominal sonogram. The sonogram demonstrated a large, approximately 13 cm heterogeneous complex mass in the right upper quadrant with numerous liver masses and possible small satellite masses. Figures 1 and 2 show a heterogeneous vascular mass within the RUQ containing both solid and cystic components. A mild amount of ascites was noted within the abdominal cavity. It was unclear as to the origin of the mass and if it originated from within the liver or from the mediastinum.
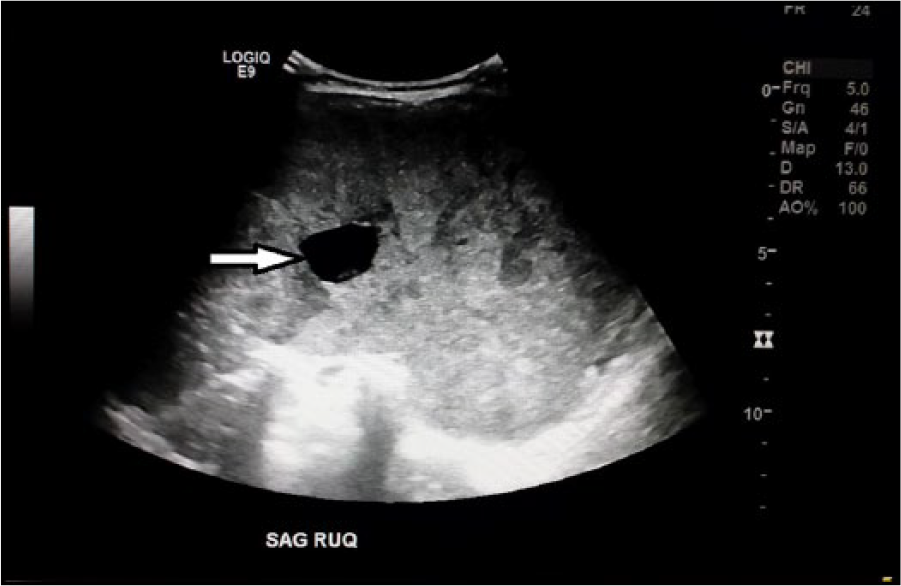
Sagittal right upper quadrant sonographic image demonstrating heterogeneous liver with fluid filled component (see arrow).
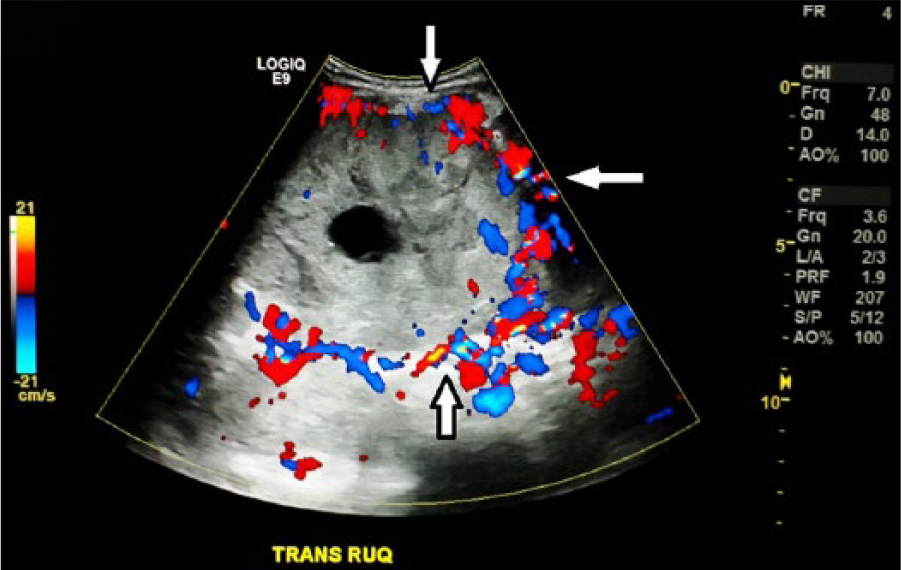
Transverse right upper quadrant sonographic image demonstrating heterogeneous liver with increased peripheral vascularity (see arrows).
The normal sonographic appearance of a young child’s liver is homogenous with midlevel echoes. The hepatic vessels should be well visualized and liver segments easy to identify. Additional sonographic images demonstrated the extent to which the metastatic lesions had infiltrated the liver parenchyma (Figures 3, 4, and 5). The initial differential considerations included a retroperitoneal immature teratoma, a pedunculated undifferentiated embryonal sarcoma or a pedunculated hepatoblastoma, or a lymphomatous mass. Given the large size of the mass, computed tomography (CT) scan or magnetic resonance imaging (MRI) examination was recommended for further evaluation.

Transverse right upper quadrant sonographic image demonstrating heterogeneous liver with fluid-filled structures throughout (see arrows).
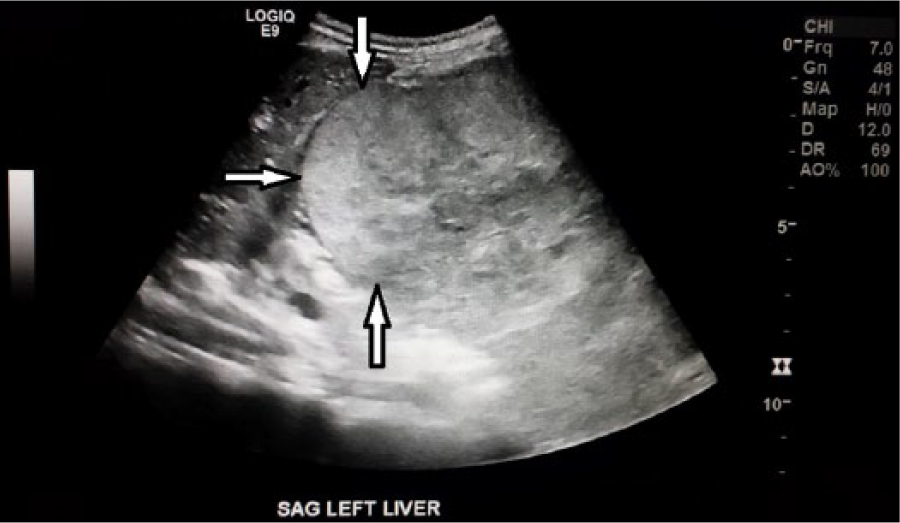
Sagittal left liver sonographic image demonstrating the appearance of a distinct heterogeneous mass. It is unclear as to whether this mass was adjacent to or part of the left lobe of the liver (see arrows).

Transverse right upper quadrant sonographic image demonstrating heterogeneous liver.
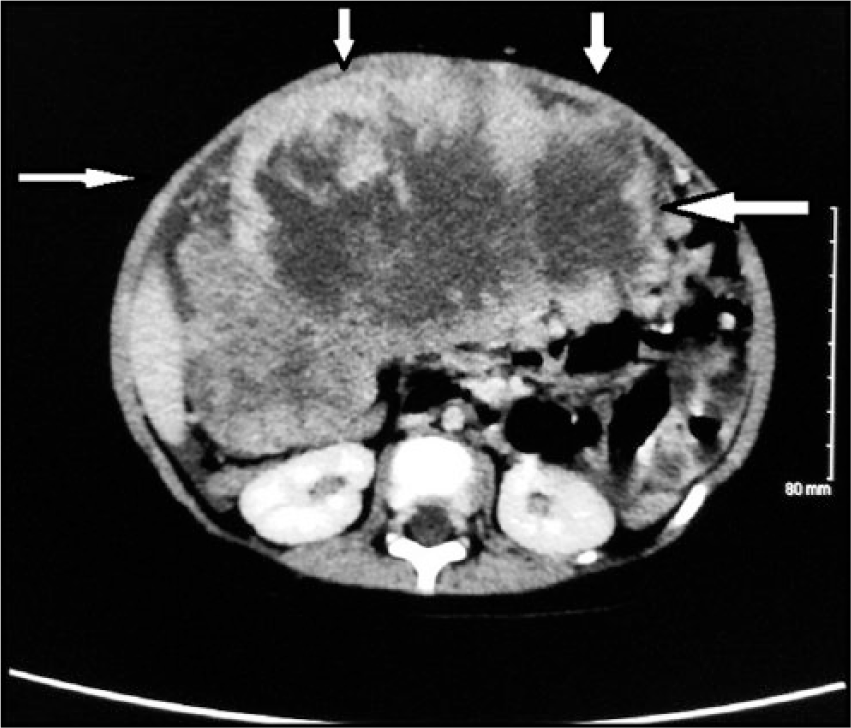
Later that day a CT was performed that revealed a large abdominal mass with liver metastases and satellite lesions and/or peritoneal spread. There was associated ascites noted, evidence of portal hypertension, multiple portal venous collaterals, and a right pleural effusion. The IVC was not well evaluated due to the extent and size of the abdominal mass as well as the phase of contrast enhancement obtained on the examination (Figures 6, 7). CT images reveal the extent to which the mass infiltrates the abdomen, as well as the lesions seen throughout the liver (Figures 8, 9, and 10).
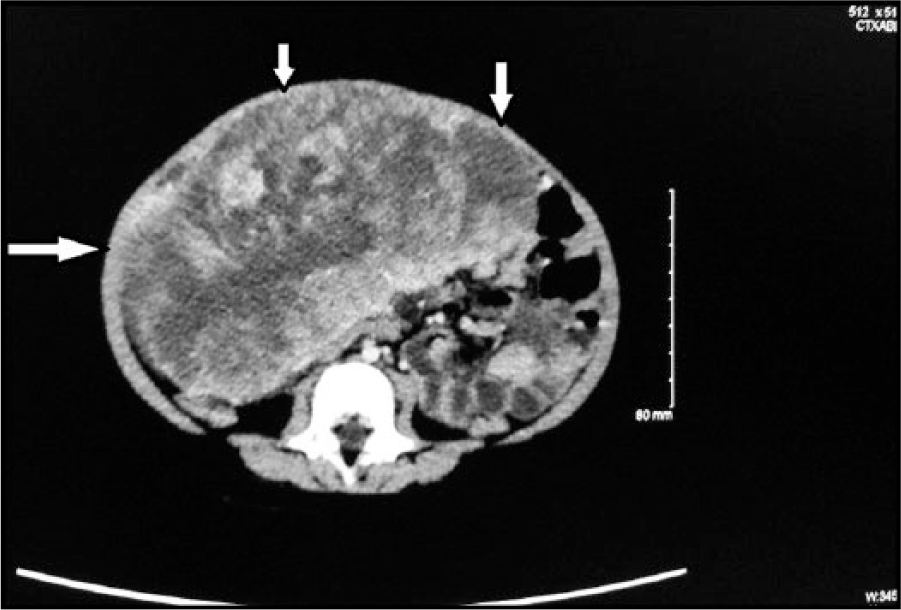
Axial computed tomography image demonstrating abdominal mass.

Axial computed tomography image demonstrating the extensive nature of the abdominal mass.
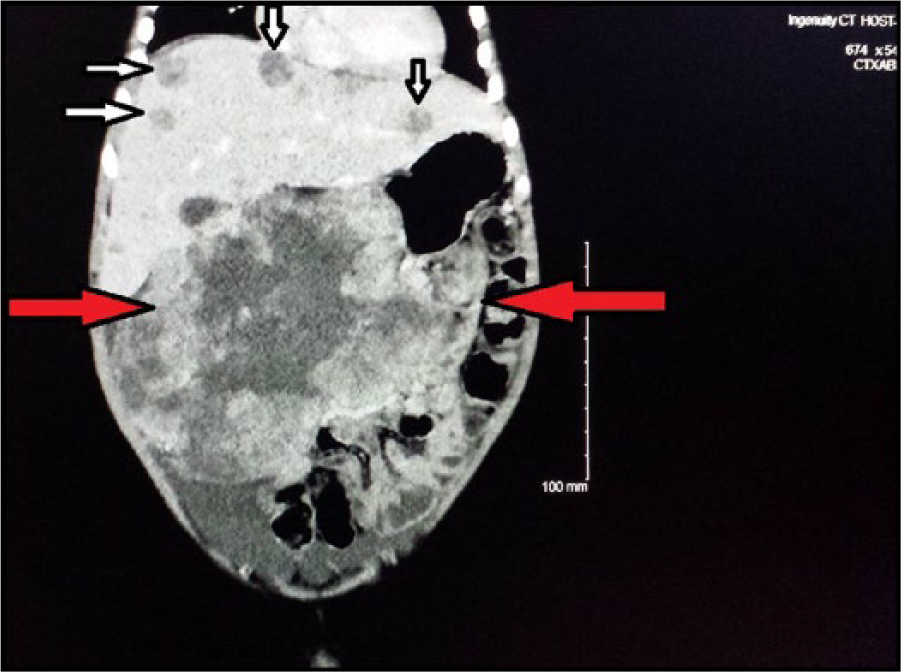
Coronal computer tomography image demonstrating the extensive nature of the abdominal mass. White arrows indicate areas of metastases to the liver. Red arrows indicate the abdominal tumor.

Coronal computer tomography image demonstrating the extensive nature of the abdominal mass. The red arrow indicates the area of the abdominal tumor.
Axial computed tomography image demonstrating the extensive nature of the abdominal mass.
On day 2, the patient continued to be consistently febrile. An echocardiogram was performed and the results were within normal limits. The patient’s lab results showed an LDH level of 1698. The patient was prepped for an open surgical biopsy and port placement to begin treatment. During the surgical biopsy, it was noted that there was a large, vascular, friable, necrotic tumor within the abdomen. The ventral aspect of the tumor at its superior margin was adhered to the line alba. There was a bridge of tissue posteriorly from hepatic segments 3 and 4b to the tumor. The tumor had multiple vessels on its surface. Multiple biopsies were taken. A right subclavian infusaport was placed in anticipation of fluid management and possible chemotherapy cycles.
On day 3, the patient remained intubated and sedated within the pediatric intensive care unit (PICU) while awaiting the pathology results and the treatment plan. Lab values were taken with most results within the normal limits. Red blood cells, hemoglobin, and hematocrit were mildly low, while platelets and glucose were mildly elevated.
On day 4, the pathology results were in and the tumor was identified as a yolk sac tumor with Schiller-Duval bodies. Chemotherapy was initiated. The patient remained intubated due to the mass effect of the tumor on his lungs. Given the vascularity of the tumor, surgical debulking or ascitic fluid drainage were determined to not be additional treatment options due to the friability of the tumor. Due to the metastases to the liver, the tumor was staged as a stage IV malignant germ cell tumor.
The patient continued to receive chemotherapy treatment in the PICU in an attempt to decrease the size of the tumor.
Discussion
To understand the origins of a germ cell tumor, the focal point to examine is the ovaries in females and testes in males. In the healthy growing body a germ cell, through its natural evolution, will develop into either eggs in the female or sperm in the male. From a biology perspective, a germ cell has a single set of 23 chromosomes containing half the usual amount of DNA and half the usual number of genes. Under the appropriate conditions cells have the ability to unite with one from the opposite sex to form a new individual; a gamete and a new life is formed.
When a germ cell does not follow its usual pathway of evolution, the cell structure can migrate from the reproductive organs and take up host in various areas of the body. They can form malignancies in areas extragonadal in locations that include, the liver, brain, lung and abdominal wall.
Pediatric germ cell tumors can have histological variation and staging capacity, which is why it is important to gather critical imaging information to determine the course of medical and surgical management. These germ cells grow in the reproductive and extragonadal regions, as well as the brain. For this case study the focus will be on germinomatous and nongerminomatous germ cell tumors.
Germinomatous (seminotous) are slower developing germ cell tumors and are subclassified as follows: dysgerminoma, which is a germ cell tumor of the ovaries; seminoma, which is a germ cell tumor of the testicles; and gerninoma which has the same histology as the seminoma and dysgerminoma, but occurs in a location within the central nervous system including the brain.
Nongerminomatous (nonseminomas) are faster developing germ cell tumors and are subclassified into four categories. The first category is yolk sac tumors, which are most often malignant ovarian and testicular germ cell tumors in the pediatric population. Second, embryonal carcinomas are those tumors wherein the malignant cells are primarily located in the testicles, however they can migrate to other locations in the body. Third, teratomas are germ cell tumors seem primarily on the sacrum and coccyx. Last, choriocarcinoma is a rare malignant, trophoblastic cancer occurring in the reproductive organs. 4
As the diagnosis of germ cell tumor is clarified, the next determination would be the level of staging at the time of identification. The staging level of the mass will direct the treatment planning and prepare the child and family for expectations through the progression of treatment. The discussion of this case study is extragonadal germ cell tumors.
The staging of extragonadal germ cell tumors are broken down into four distinct stages. To be classified as a stage I tumor, the germ cell cancer is in one place and can be completely removed by surgery. For tumors at the base of the sacrum and coccyx (tailbone), the cancer and tailbone are completely removed by surgery. Typically, tumor marker levels return to normal after surgery. Stage II occurs when the germ cell cancer has spread to nearby tissues and/or lymph nodes and is not completely removed by surgery. The germ cell cancer remaining after surgery can be seen with a microscope only. Tumor marker levels do not return to normal after surgery and may be elevated.
When the cancer has reached the level of stage III, it has metastasized to lymph nodes and is larger than 2 centimeters in diameter. At stage IV, the germ cell cancer has metastasized to various parts of the body, including, but not limited to the liver, lungs or abdomen. If fluid is present within the abdominopelvic cavity, a paracentesis can be performed to remove this fluid for testing to confirm how far the cancer has progressed.
Clinically identified pediatric patients have been seen with a predisposition for genetically related issues that may put them at a higher risk of developing germ cell tumors. These include Klinefelter’s syndrome, in which males develop with an extra X chromosome, Turner’s syndrome, a genetic condition where females develop with a missing X chromosome, and cryptorchidism, undescended male testicles. 5
As in this case study, rapidly developing germ cell tumors will begin to manifest clinical symptoms as they compromise regular body function. The pediatric patient will present with signs and symptoms consistent with the body regions affected. The parent may report they have seen the child experience increases in abdominal pain, chest pain or breathing difficulty, cough or fever, digestive issues or changes in bowel habits and patterns, fatigue, and/or difficulty walking.
The typical sonographic and CT features of germ cell tumors vary depending on the location and progression of the disease. When occurring in the abdomen, most of these tumors are found in the anterior mediastinum or the retroperitoneum. 6 Sonography will show abdominal or hepatic masses ranging in appearance from homogeneous to heterogeneous. Heterogeneous masses may include cystic areas or calcifications. Such masses may appear to invade the liver or stomach, sometimes with associated ascites. The sonographic findings may be very similar to those of a hepatoblastoma.
On CT, germ cell tumor lesions may appear multilobulated, solid and heterogeneous. Hepatic lesions with hypodense components and possibly calcifications may be noted with heterogeneous enhancement of the tumor with contrast-enhanced CT and the liver often shows extensive metastatic disease. Pronounced lymph nodes within the surrounding area are often identified and ascites may be noted.
In this case study, both sonography and CT proved to be reliable and valid imaging choices. Sonography identified the large mass within the abdominopelvic cavity, as well as the metastatic hepatic lesions and associated ascites, but was unable to determine the exact origin of the tumor. Further imaging by CT was required to determine a more detailed account of the tumor and its origin, and to evaluate the size and adjacent anatomical structures within the identified area.
Due to the varying appearance of extragonadal germ cell tumors, the initial differential considerations may include hepatoblastoma, retroperitoneal immature teratoma, retroperitoneal leiomyosarcoma, undifferentiated embryonal sarcoma, rhabdomyosarcoma, or a lymphomatous mass. Many of these differentials were considerations in this particular case study.
To supplement the clinical presentation and the imaging studies, blood levels of significance importance include alpha-fetoproteins (AFP), beta-human chorionic gonadotropin (β-HCG), and lactate dehydrogenase (LDH). These three laboratory values will have significance when diagnosing and treating yolk sac tumors, embryonal carcinomas, and choriocarcinoma. 7
As a treatment plan is formulated, the health care team must review all data accumulated through the diagnostic work-up. A careful review of the pediatric patient’s clinical examination, history and physical, biopsy tissue analysis, laboratory trends and diagnostic imaging are required. At this juncture, full disclosure and transparency with the family is key to what will be ahead for the treatment of this form of cancer.
Treatment for this form of tumor is largely dependent on the staging as previously mentioned; a more targeted regime has demonstrated significantly improved outcomes. Chemotherapy (some being platinum-based) involves the infusion of three compounds over a cycle period; these include intravenous cisplatin, etoposide, bleomycin. Radiation therapy is not routinely used for initial therapy, except in some instances of germinoma, instead of chemotherapy.
The treatment plan sequencing for the patient is determined by the stage and location of the tumor. For stage II-IV testes, stage II-III ovary, and stage I-II nontestes or ovary, a cisplatin, etoposide, and bleomycin regimen is administered intravenously every 3 weeks for 3 cycles. For stage IV ovary, stage III or IV nontestes or ovary, a cisplatin, etoposide, and bleomycin regimen is administered intravenously every 3 weeks for 4 cycles. In all stages, surgical intervention will depend primarily on the location and the treatment response to the chemotherapeutic infusion. 8
After the chemotherapy regimen has been completed, surveillance imaging will be necessary to determine the effectiveness. If residual tumor persists, surgical resection may be recommended to decrease risk even further. Response to the initial chemotherapy treatment will be a determining factor, when deciding if a second round of chemotherapy is required. Current remission rates are approximately 90% for stage I, 90% for stage II, 87% for stage III, and 82% for stage IV germ cell tumors. 9
Patients who demonstrate a reoccurrence after their first round of chemotherapy may still achieve a cancer free state. A more aggressive approach must be taken with the secondary utilization of additional agents. The infusion of paclitaxel, ifosfamide and carboplatin is commonly employed and then an autologous stem cell transplantation is completed as the patient can tolerate. This second phase does not come without risk. Bone marrow suppression and Immune system suppression subject the patient to an opportunist infection. If not carefully observed, the patient could easily develop a life-threatening, overwhelming infection.
Autologous stem cell transplantation involves harvesting the patient’s blood or marrow stem cells, followed by very high dose chemotherapy with carboplatin and etoposide. After the administration of the carboplatin and etoposide, the patient’s own stem cells are transfused to reestablish bone marrow function and blood cell production. This is a very complex process that requires careful monitoring and hospitalization. In some cases the bone marrow suppression and stem cell transplant may be repeated a second time. This emotional and financial burden can be very overwhelming to the patient and the family. Without treatment, survival rates are very small due largely to the aggressive nature of this form of cancer. 8
Conclusion
Research on this type of cancer tells us that significant surveillance must be maintained following successful treatment and emphasis must be placed on the postsurgery, chemotherapy, and stem cell transplant phases. Careful attention must be paid to multiple organ systems to see their response to possible chemotherapy toxicity. Renal function, pulmonary function, and auditory testing should be assessed and monitored postinfusion. Alpha-fetoproteins and beta-human chorionic gonadotropin will need to be followed to measure a clinical reoccurrence and presence trend of the cancer.
Supportive imaging will also be necessary to spot any early detection of a return of the germ cell tumor. This includes but is not limited to follow-up chest radiograph, CT, and sonography. The patient in this case study illustrates how well most patients respond to treatment and have limited to no residual side effects. The struggle that greatly affects outcome is the aggressive nature of the disease and the severity of the treatment plan. Supportive measures to the family are just as important to the success of the treatment. Many families demonstrate significant stress reactions during this long difficult process. Providers must be aware of this as they experience parents who may lash out in frustration when they are watching their child undergo this process. Many parents are faced with the harsh reality that their child may be in the statistical percentage of children that succumb to this form of cancer. Knowledge and understanding will help make interaction and care with this patient population a significant part of the overall treatment and healing plan.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.