
Abstract
Ovarian embryonal cell carcinoma is an uncommon ovarian germ cell tumor. This case study is a report of a patient referred for sonography based on abdominal pain and abnormal levels of alpha-fetoprotein (AFP) and β-human chorionic gonadotropin (β-hCG). A large heterogeneous pelvic mass was characterized by sonography and was surgically proven to be a malignant ovarian embryonal cell carcinoma.
Malignant ovarian germ cell tumors consist of a broad spectrum of cell types that can be classified into six different types: dysgerminoma, yolk-sac tumor, embryonal carcinoma, polyembryoma, choriocarcinoma, and teratoma. 1 Germ cell ovarian tumors are very uncommon, as they make up less than 10% of all ovarian cancers, with only 2% to 3% being malignant. 2 Embryonal carcinomas are extremely rare and represent only approximately 4% of malignant ovarian germ cell tumors. 3 Embryonal carcinomas primarily occur in younger patients; therefore, sonography is the imaging modality of choice for visualization.4–6 A case of ovarian embryonal cell carcinoma is presented and discussed, illustrating the important role of sonography.
Case Report
A 13-year-old female presented to the emergency room complaining of right upper and lower quadrant pain over the past two weeks. A urine pregnancy test was positive along with a beta human chorionic gonadotropin (β-hCG) level of 535 mIU/mL. The patient denied any history of sexual activity. Abdominal and pelvic sonography were ordered because of abdominal distention and the increased β-hCG level. Both were done using a Philips iU-22 ultrasound system (Philips Medical, Bothell, Washington) with a 5- to 8-MHz curvilinear transducer. Fluid was seen in Morrison’s pouch and within the pelvis (Figure 1), along with an 11.3 × 5.7 × 5.6-cm heterogeneous pelvic mass with cystic and solid components (Figure 2). Color Doppler imaging showed the mass to have internal blood flow (Figure 3); spectral Doppler showed the internal arterial flow to be of low resistance (Figure 4). The mass (arrowhead) was superior to and separate from the uterus (arrow, Figure 5). These findings were thought to be most consistent with a dysgerminoma. The differential diagnosis included a ruptured ectopic pregnancy or a teratoma.
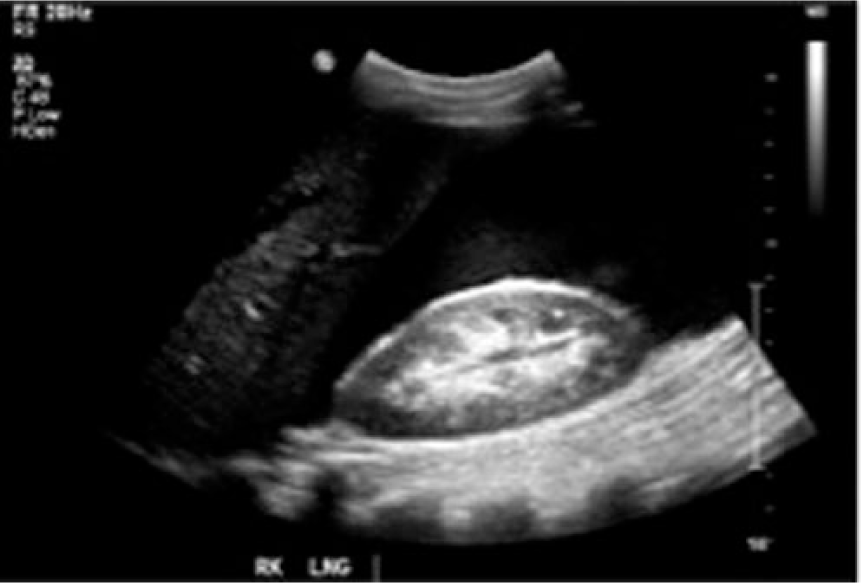
Longitudinal gray-scale image showing significant ascites in the right upper quadrant.

Longitudinal gray-scale image showing the heterogeneous pelvic mass noted to be primarily solid with minor cystic components.
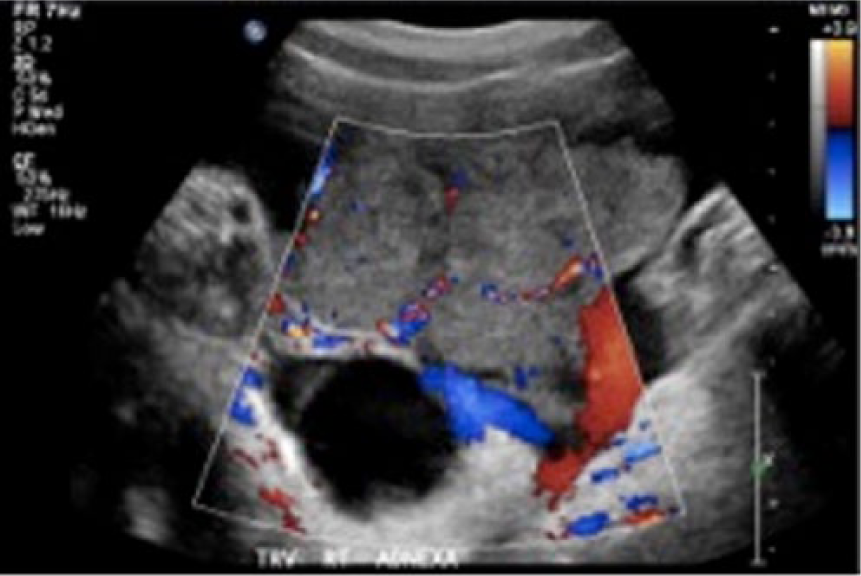
Transverse color Doppler imaging of the pelvic mass showing extensive internal arterial and venous blood flow.
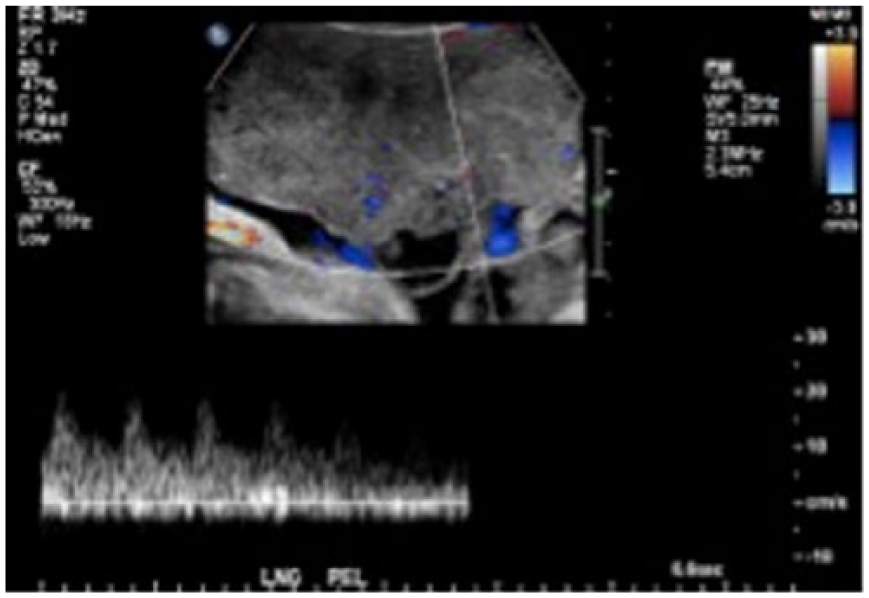
Longitudinal spectral Doppler image showing low resistance arterial blood flow in the pelvic mass.
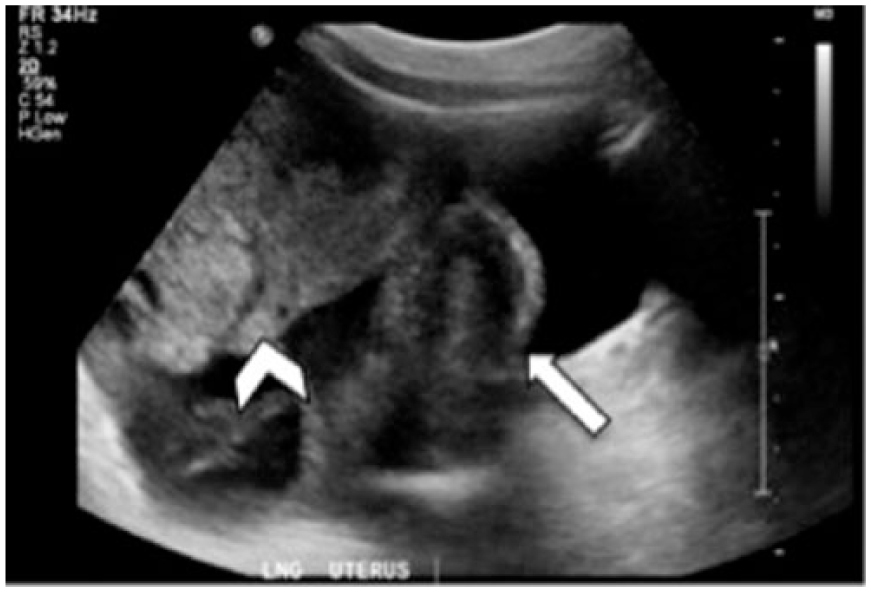
Longitudinal gray-scale image of the mass (arrow head) which is seen to be superior and separate from the uterus (arrow).
A computed tomogram (CT) of the abdomen and pelvis confirmed these findings. Bilateral pleural effusions and an enlarged right-sided retroperitoneal lymph node were also seen. In addition to the large mixed solid and cystic multilobulated mass found in the pelvis, smaller masses were present in the left adnexal region.
Less than a week later this patient underwent surgery to remove the right ovarian mass. The surgical pathology report indicated that the pelvic mass was an ovarian malignant germ cell tumor, specifically a pure embryonal carcinoma. Metastatic embryonal carcinoma was found in the bladder, omentum, and a para-aortic lymph node. Based on these findings, the patient was diagnosed with a stage IIIC malignancy, using the 2014 International Federation of Gynecologists and Obstetricians (FIGO) staging system for ovarian tumors. 7 A few months following surgery, a CT of the abdomen and pelvic regions was repeated. No residual or recurrent pelvic masses were identified.
Discussion
Ovarian germ cell tumors originate from primitive germ cells and progressively differentiate to mimic developmental tissues of embryonic origin and extra-embryonic tissues. 2 Embryonal carcinoma is a rare ovarian germ cell tumor that is highly malignant and contains a disorganized array of many somatic and extra-embryonic cells. 8 It is often associated with an abnormal hormonal manifestation such as irregular bleeding or dysmenorrhea because of β-hCG stimulation. The mean age at presentation is 15 years, with Asian and African American ethnicities having a higher incidence. 2
An ovarian embryonal carcinoma tumor presents with abdominal pain in 87% of cases. 4 Ascites occurs in 20% of cases and vaginal bleeding occurs in 10%. A palpable abdominal mass and abdominal distention are also common findings. Fever is present in 10% to 25% of cases. Symptom duration is usually short, with a median duration of two to four weeks prior to diagnosis, indicating rapid tumor growth. Tumor markers are important for the diagnosis of malignant germ cell tumors. Elevated alpha-fetoprotein (AFP) and β-hCG levels are generally indicative of a malignant ovarian germ cell tumor. Embryonal carcinoma may produce both β-hCG and AFP, with β-hCG being most common. 9
Sonography can be used to define the size and complexity of ovarian tumors.3,6 Sonographic characteristics suggestive of a malignant ovarian germ cell tumor include an irregular solid tumor, the presence of ascites, papillary projections within the mass, a diameter greater than 100 mm, and internal blood flow. 5 Previous case reports have shown embryonal carcinoma on sonography to be predominantly solid and hypervascular, with some cystic components. Gray-scale imaging of malignant ovarian germ cell tumors may show irregular septa dividing the tumor tissue into a lobelike pattern. Color Doppler evaluation shows bidirectional flow suggesting arterial and venous blood flow within the mass. 10 The absence of a separate or normal ovary ipsilateral to the mass can help distinguish this mass from one of extra-ovarian origin. 2 The differential diagnosis of an ovarian embryonal carcinoma on sonography includes teratoma, choriocarcinoma, yolk-sac tumor, or ruptured ectopic pregnancy.
Diagnosis of an ovarian embryonal cell carcinoma includes appropriate history, clinical signs and symptoms, and sonographic findings as well as tumor markers and CT examination. Staging is based on the 2014 FIGO classification system. 7 Each of the four stages can be furthered subdivided into separate categories based on histologic spread (Table 1).
International Federation of Gynecologists and Obstetricians (FIGO), Ovarian Cancer Staging (Effective January 1, 2014).
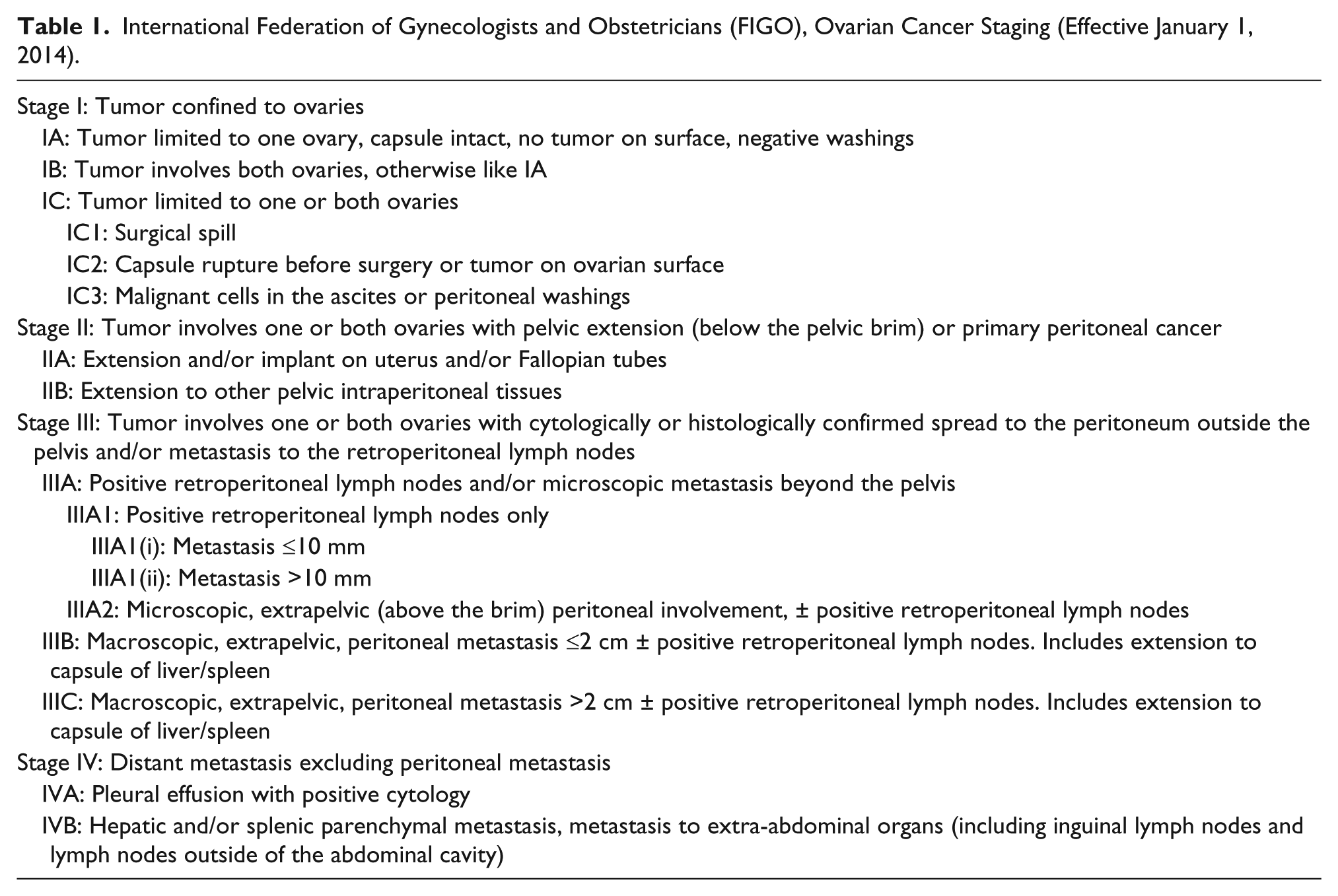
Stage I: The tumor is confined to the ovaries.
Stage II: The tumor affects one or both ovaries and extends to the pelvis or implants outside the ovary.
Stage III: The tumor affects one or both ovaries, with histologically confirmed peritoneal implants outside the pelvis (metastasis to liver, small intestine, or omentum is equivalent to a stage III) and/or metastasis to the retroperitoneal lymph nodes.
Stage IV: The tumor affects one or both ovaries and shows distant metastasis (excluding peritoneal metastasis).
Definitive diagnosis of ovarian embryonal carcinoma is made by histology. At the time of diagnosis, stage IIIC is the most common stage, accounting for approximately 70% of cases. 11 Management of most embryonal carcinomas and other malignant ovarian germ cell tumors includes complete surgical excision. Because of the young age of the population primarily affected by these tumors, fertility-sparing surgical treatment is preferred. 2 Treatment for advanced-stage disease is hysterectomy with bilateral adnexectomy. Chemotherapy may also be administered in advanced disease. Prognosis for these tumors depends on FIGO staging, size, and histology.1,4,9 Patients in stage 1 have high cure rates with surgery alone. Other stages require surgery and chemotherapy with close surveillance. Most patients with a malignant germ cell tumor are successfully treated; however, recurrence is reported in 20% to 30% of patients. 1
Conclusion
Embryonal carcinoma is a rare malignant germ cell tumor. Sonography is the imaging modality of choice because of the prevalence of embryonal carcinoma in younger patients. The specific diagnosis of this tumor ultimately is made by histology. The prognosis and the treatment of these tumors are variable. Although specific differentiation of malignant germ cell tumors by sonography is not possible, sonographic characteristics, along with clinical and pathologic findings, can aid in making a correct diagnosis. Sonography can also aid in the monitoring of these patients after treatment.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.