
Abstract
Peripheral arterial disease (PAD) commonly results from progressive narrowing of arteries in the extremities because of atherosclerosis. More than 8 million people in the United States have PAD. The majority of individuals with PAD are seniors with one or more cardiovascular disease risk factors. Because patients with PAD may be asymptomatic, the true incidence of PAD may be underreported. Accurate and timely diagnosis of PAD is very important for optimal treatment.
Keywords
Introduction
Noninvasive physiologic studies such as the ankle-brachial index (ABI), segmental blood pressure measurements (with continuous wave Doppler or pulse volume recordings), and toe-brachial index (TBI) are widely used for the screening and initial diagnosis of individuals with risk factors for peripheral arterial disease (PAD) (hypertension, diabetes mellitus, hyperlipidemia, smoking, impaired renal function, and history of cardiovascular disease). The ABI (or the TBI) is one of the common first diagnostic steps for patients with intermittent claudication, decreased pedal pulses, and paresthesia. After the initial test, arterial duplex examination and computed tomography angiography (CTA) tend to provide significant data about the true extent of PAD, pinpointing the anatomic levels of the disease and grades of stenosis. These diagnostic methods are complementary to each other and have positive correlations between them.
Case Presentation
A 53-year-old patient was referred to an imaging center with complaints of severe pain and paresthesia (intense burning sensation) in the left lower leg and foot for 1 month. The patient’s risk factors included hypertension and smoking. In addition, there was a serious left foot injury 18 years prior, which resulted in the left first toe amputation. The patient had been diagnosed with PAD 3 years ago and had five vascular interventions in the past 1.5 years, including angioplasty with a stent placement in the left superficial femoral and popliteal arteries. On physical examination, the patient’s left foot was cold, the skin appeared to be glossy (especially of the toes), and the pulse in both left dorsalis pedis and posterior tibial arteries was barely detectable (Figure 1).

Photo of the patient’s feet. Note the shiny appearance of the skin of the left foot (with the first toe surgically absent) versus the normal right foot.
The noninvasive physiologic examination was completed using a Parks Vascular Mini-Lab 1059-C (Parks Medical Electronics, Inc., Aloha, Oregon). Because of the severe pain in the left leg, an ABI Doppler study was not attempted. The test started with measuring brachial arterial blood pressure (BABP) bilaterally. The right systolic BABP measured 135 mmHg; the left was 130 mmHg. This indicated a 5-mmHg difference between the arms, which is within the normal range of a maximum difference of 10 to 15 mmHg. 1 The highest value, 135 mmHg BABP, was used for the calculation of the TBI bilaterally. Photoplethysmography (PPG) was used for recording the waveform and measuring arterial blood pressure of the second toe bilaterally due to the absence of the left great toe. A Hokanson 2.5-cm toe cuff (Bellevue, Washington) and Riester RI-San aneroid sphygmomanometer (Germany) were used for the measurements of the toe blood pressure. The toe systolic pressures were obtained by placing a PPG probe on the distal plantar aspect of the right and left second toes. The probe was attached with double-sided adhesive tape. After recording a PPG waveform (at 5 mm/second speed), a toe cuff was placed proximally to the PPG probe. After inflating the cuff slightly above the pressure that had stopped the PPG waveform, the cuff was slowly deflated, and the toe pressure was noted at the moment of the waveform reappearing. The TBI was estimated by dividing each toe pressure by the highest brachial pressure. The right second toe pressure measured 115 mmHg, whereas the left second toe pressure was 25 mmHg. The right TBI was 0.85 and the left TBI measured 0.19 (normal TBI > 0.70) (Figure 2).
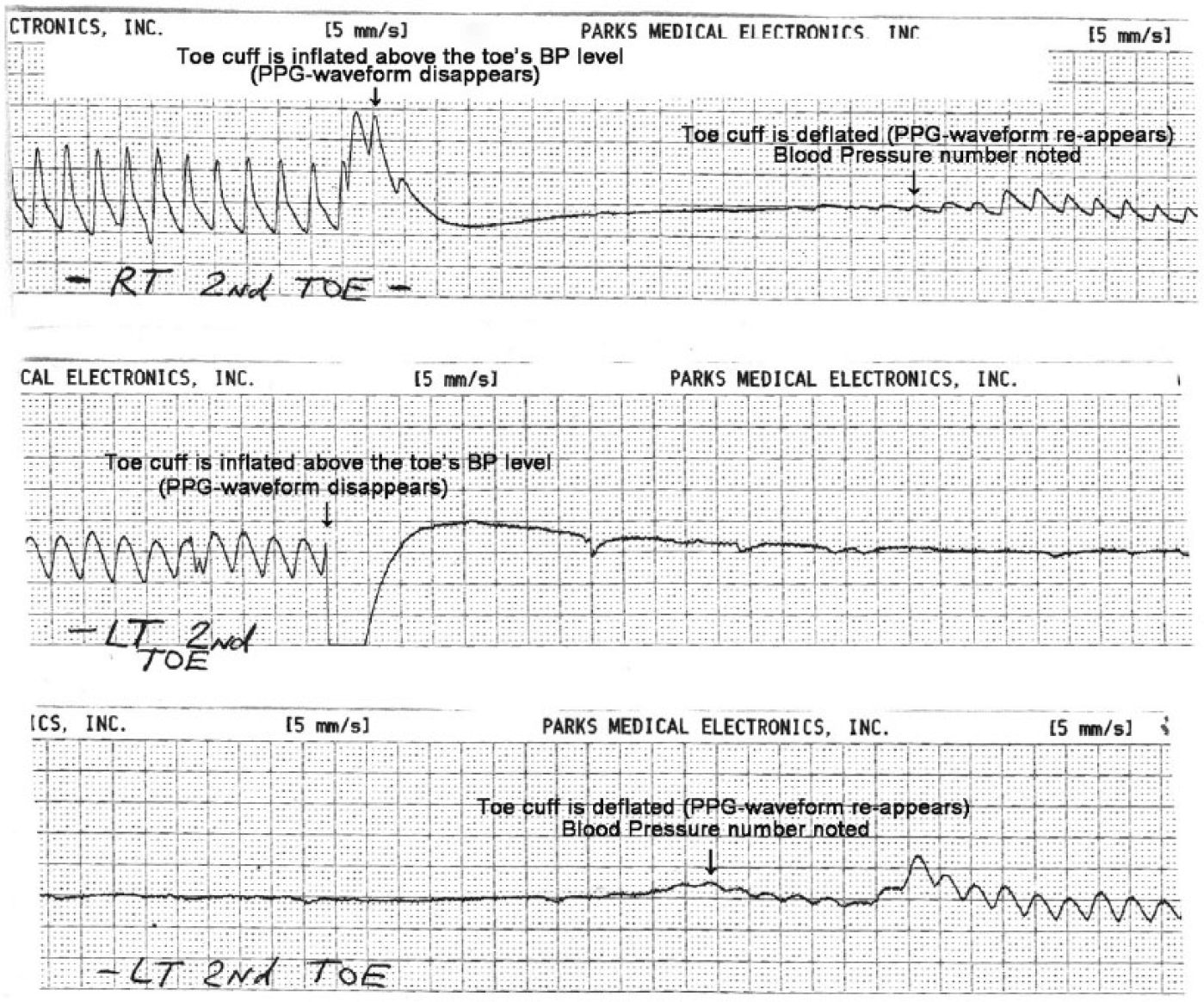
Photoplethysmography waveforms taken on the patient’s right and left second toes.
When reviewing the PPG waveforms (Figure 2), notice the difference in the amplitude, upstroke, peak, and downslope of the pre-cuff-inflation waveform between the normal-appearing right and abnormal-appearing left toes. In addition, it took much longer to detect the reappearing PPG waveform in the left toe; therefore, there are two left printouts instead of only one on the right side.
Duplex sonographic examination of the lower extremity arteries was performed after the TBI measurements, using a GE-Logiq S8 (General Electric Medical Systems, Milwaukee, Wisconsin) system with a linear 9L transducer. The protocol used included bilateral scanning of the common femoral artery (CFA), profunda femoris artery (PFA), superficial femoral artery (SFA), popliteal artery (PA), tibio-peroneal trunk, anterior tibial artery, and posterior tibial artery on multiple levels. Bilateral multifocal atheromatous plaques were visualized. There was 40% diameter reduction of the proximal right PFA. High-grade stenosis (more than 70% based on diameter reduction and elevated peak systolic velocity) was detected at the distal right anterior tibial artery. These diagnostic criteria were lab specific and based on the patient outcomes in that locale. No flow was visualized within the distal left SFA. A stent was present within the distal aspect of the left SFA and left PA (proximal segment), which was occluded. The proximal and mid segments of the left PA were also occluded. There was a reconstitution of blood flow at the level of the distal segment of the left PA via the left superior lateral geniculate artery. The left lower extremity’s distal arteries (both the anterior and posterior tibial) demonstrated reconstituted arterial flow from the distal segment of the PA (Figures 3 and 4).
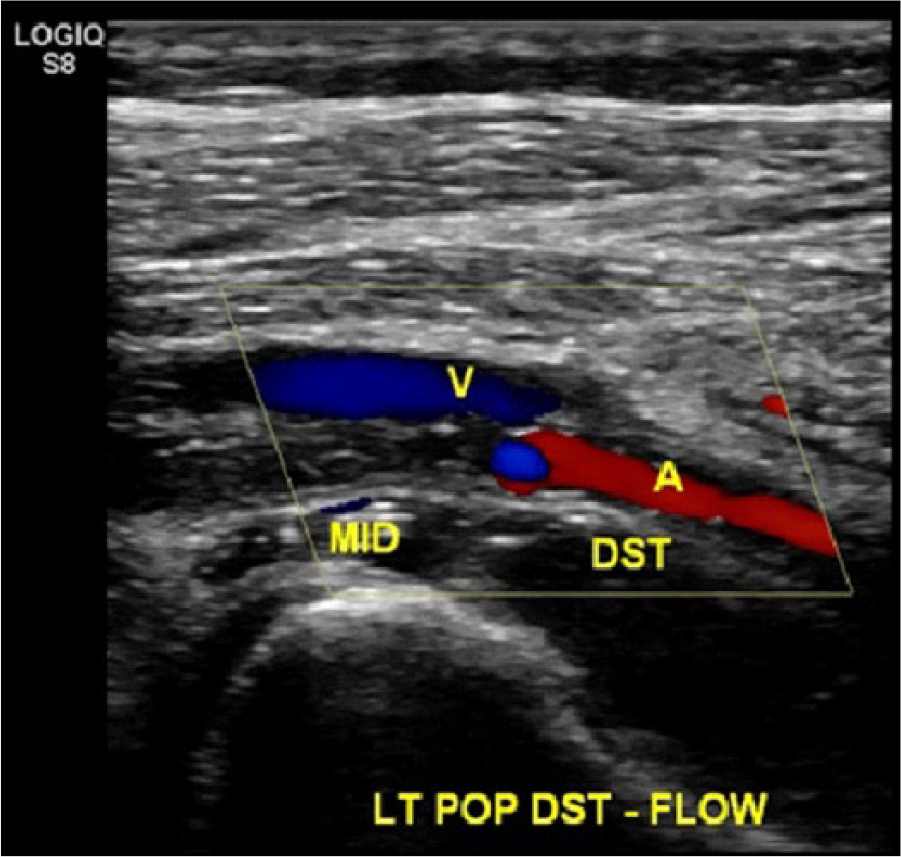
Color Doppler demonstrates a lack of blood flow in the occluded mid segment and reconstituted flow in the distal segment of the left popliteal artery. A, popliteal artery; DST, distal segment of the popliteal artery; MID, mid segment of the popliteal artery; V, popliteal vein.
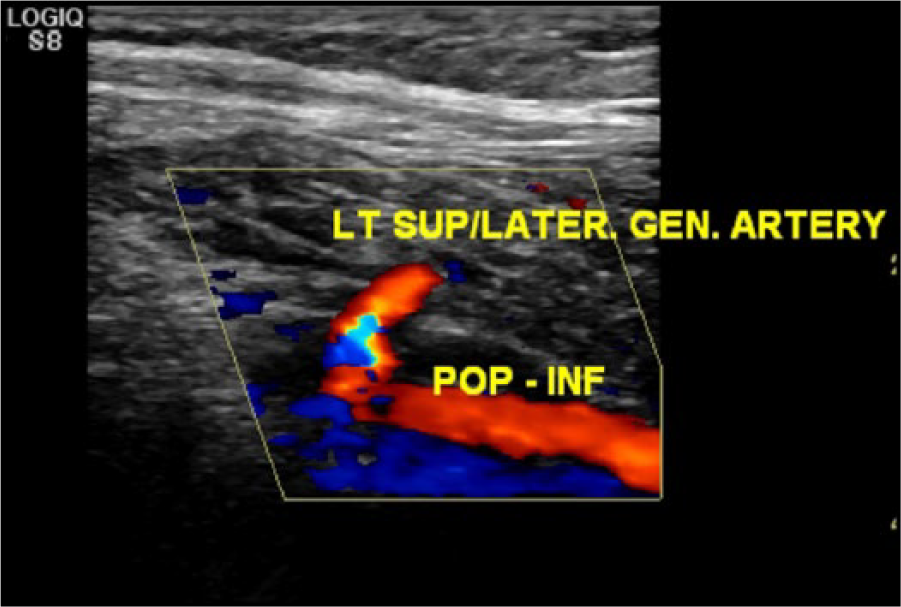
Color Doppler image of the left superior lateral geniculate artery (LT SUP/LATER. GEN. ARTERY) junction with the distal segment of the left popliteal artery (POP-INF), restoring blood flow below the knee.
Three weeks prior to the noninvasive physiological study and duplex examination, the patient had a CTA runoff study with and without contrast. Computed tomography angiography of the lower extremity arteries was performed on a GE Discovery STE (General Electric Medical Systems) following the intravenous administration of 175 mL of Optiray 350 (Mallinckrodt) contrast. The images were obtained in the axial plane followed by coronal and sagittal maximum intensity projection reconstruction and 3D volume rendering. The total dose length product was 2381 mGy.cm and the total computed tomography dose index was 31 mGy. The CTA finding showed that the proximal to mid left SFA was diminutive in appearance. There was a stent present in the distal left SFA extending to the left PA, which was occluded. Just above the level of the stent, the left SFA was occluded. The proximal and midportion of the PA contained a stent, which was occluded. There was distal reconstitution of blood flow via the superior lateral genicular artery (Figures 5 and 6). There was three-vessel runoff to the left mid calf and two-vessel runoff to the left ankle.

Computed tomography angiography sagittal view of the left knee region showing the occluded stent in the proximal and mid segments and reconstituted blood flow in the distal portion of the left popliteal artery.

Computed tomography angiography volume rendered 3D reconstruction. Frontal view of the lower extremity arteries at the distal thigh–knee and just below the knee levels. The interruption of contrast is clearly visible in the proximal–mid left popliteal artery, whereas the left superior lateral genicular artery provides collateral flow to the left distal popliteal artery.
Discussion
Approximately 8.5 million people in the United States have PAD, including 12% to 20% of individuals older than 60 years. The vast majority of individuals with PAD have one or more cardiovascular disease risk factors. 2 General population awareness of PAD is estimated at 25%, based on prior studies. 3 The prevalence of this disease seems to increase significantly with age. Patients with PAD may be asymptomatic or have atypical symptoms, and the true incidence and prevalence of PAD may be greatly underestimated. Accurate and timely diagnosis of PAD provides an opportunity for earlier medical intervention and helps prevent future morbidity and mortality.1,4
According to published data, PAD can be determined with high sensitivity and specificity using the ABI. Peripheral arterial disease is suggested when an ABI is lower than 0.90 in either leg. 2 However, many diabetic patients with PAD also have medial artery calcification (MAC) that results in an increased stiffness of the arterial wall, which often affects distal arteries. As a result, patients who have both disorders, PAD and MAC, could have false negative results with an ABI, because of the falsely high blood pressure measurements at the ankle (it requires more pressure to compress the hardened arterial walls). Therefore, according to the report of the National Health and Nutrition Examination Survey, the presence of PAD is defined not only by an ABI < 0.9 but also with values > 1.4. 2
The TBI is one of the alternative methods of noninvasive vascular assessment. The TBI is a ratio of the systolic toe pressure divided by the highest systolic brachial pressure. A normal value for the TBI is 0.7 or higher. The TBI has high sensitivity and specificity for detecting PAD in patients with MAC (because the digital arteries usually are not as calcified as the calf arteries), including those with diabetes-related PAD, with neuropathy, and on hemodialysis for end-stage renal disease. According to recently published data, the TBI has higher sensitivity (71%) for the presence of PAD than the ABI (45%) in patients with MAC. However, the ABI had higher specificity (93%) than the TBI (79%).5,6
The standard for the performance of physiologic evaluation of extremity arteries developed jointly by the American College of Radiology, American Institute of Ultrasound in Medicine, Society of Interventional Radiology, and Society of Radiologists in Ultrasound states that “there are no absolute contraindications for this examination,” without any further clarification on whether those contraindications related only to the ABI or to all other physiologic tests. 7
At some imaging facilities, a segmental pressure examination may be contraindicated in patients with stents, arterial bypass grafts, and arterio-venous fistulas/grafts at the knee level and below. The concern often in these facilities is the risk of damaging those structures by a blood pressure measuring cuff when it is inflated and then deflated. Other possible contraindications for an indirect arterial examination include open skin wounds or cellulitis below the knee, as well as severe pain due to critical limb ischemia (CLI) and acute deep venous thrombosis. 8
The patient’s leg, shown in Figure 7, had undergone numerous arterial bypass and angioplasty surgeries; the most recent one was performed 2 months prior to the requested examination. The patient had undergone a bypass graft from the left CFA to the mid-calf peroneal vein. There were also open skin ulcers in the distal calf. An indirect examination with cuffs is contraindicated for this patient because of the arterial graft in the mid-calf and the skin ulcers. The TBI was used instead and measured 0.4 (normal > 0.7).

Left leg of a patient with severe peripheral vascular disease.
In addition to measuring the ABI and TBI, there are other methods of nonimaging physiologic arterial testing. Those additional tests include an ABI with exercise, multisegmental limb blood pressure measurements, pulse volume recordings, and transcutaneous oxygen tension measurements. It is noted that varied combinations of these examinations are provided in different diagnostic centers.
The most common arterial stenosis site in lower extremities is the distal SFA (in the adductor canal). When it is occluded, the lateral genicular artery (re-routing blood from the descending trunk of the PFA) usually provides collateral flow to the PA. 9
Duplex sonography (DS) is a valuable method for the detection of high-grade stenosis (> 50%) or occlusion, with 86% sensitivity for aorto-iliac lesions and 80% for femoro-popliteal disease and a specificity of 96% or greater for both. 10 When DS was compared with four-row CTA, there was an excellent agreement for the diagnosis of graft stenosis, aneurysmal changes, and arteriovenous fistulas. There was no difference between DS and CTA when compared with digital subtraction angiography. The sensitivity of CTA for high-grade stenosis (> 50%) or occlusion was 95% with a specificity of 96%. However, the diagnostic performance of CTA in tibial disease is lower, compared to the aorta-iliac and femoral levels, particularly in the setting of heavily calcified vessels. 10
It is important to remember that CLI develops in approximately 1% of all PAD cases. 11 Critical limb ischemia is associated with a greater risk for cardiac ischemic events, leading to increased morbidity and mortality rates from coronary artery disease. One of the diagnostic criteria for CLI is toe pressure < 30 mmHg. Another important diagnostic factor for CLI is the status of microcirculation. Microcirculation is the system of the smallest vessels, including the arterioles, capillaries, venules, and lymphatic vessels. Skin microvessels are valuable for evaluating systemic vascular diseases, including CLI. 12
Traditional plethysmography methods measure volume changes in limbs in response to arterial blood flow. Among the common plethysmography techniques are air plethysmography, impedance plethysmography, and strain-gauge plethysmography. Photoplethysmography is a similar procedure, but instead of measuring volume changes in the extremity, PPG detects variations in cutaneous (superficial microcirculatory) blood flow. 13 Photoplethysmography is usually used for measurements of arterial blood pressure of fingers and toes and for the evaluation of the severity of venous reflux. A PPG sensor transmits infrared light through the skin and detects the reflected beam. In the process, the infrared rays collide with blood cells circulating in the superficial capillaries, which partially absorb and reflect the light back to the sensor. When measuring arterial digital blood pressure, a PPG waveform is recorded continuously and allows detections of the disappearance and reappearance of the signal corresponding to the inflation and deflation of a toe/finger pressure cuff. Photoplethysmography uncovers changes in the amount of blood flow in the distal parts of the digits underneath the PPG sensor, but it does not evaluate blood flow direction. A normal PPG waveform starts with a sharp upstroke and then briefly descends toward the baseline, followed by the second short upstroke and a final return to the baseline. All of these phases could be documented at a 25 mm/second speed printout with an indirect arterial machine but not so clearly at a 5 mm/second speed (used for this case study), which is commonly used for the measurement of digital pressures (Figure 8).
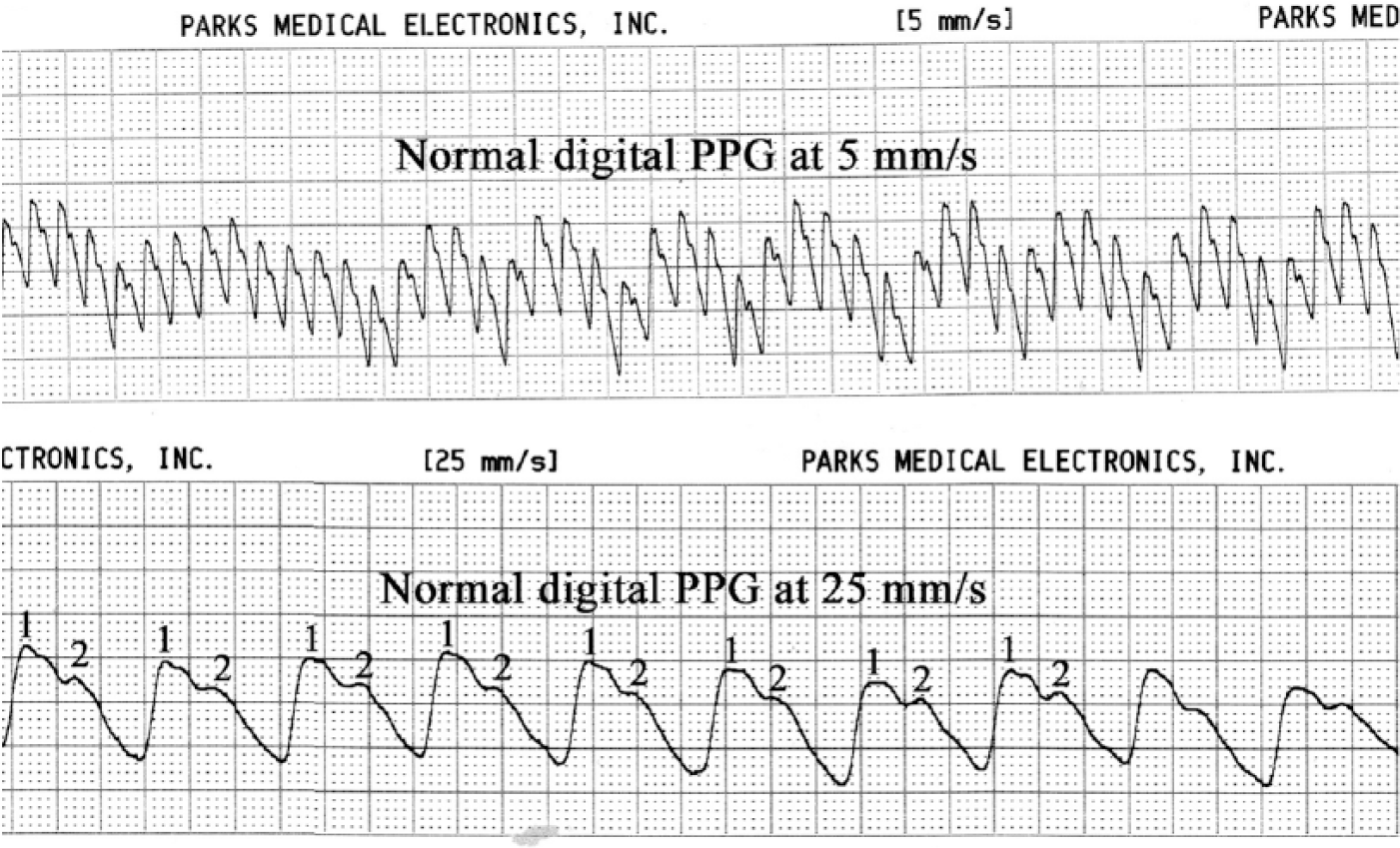
Normal digital photoplethysmography waveforms at a 5 mm/second speed above and 25 mm/second speed below. The two peaks of each wave cycle are clearly seen on the faster recording.
Since PPG registers volume changes in the microvascular bed of tissue under the skin, it is a valuable and safe method for CLI diagnosis (Figure 9).
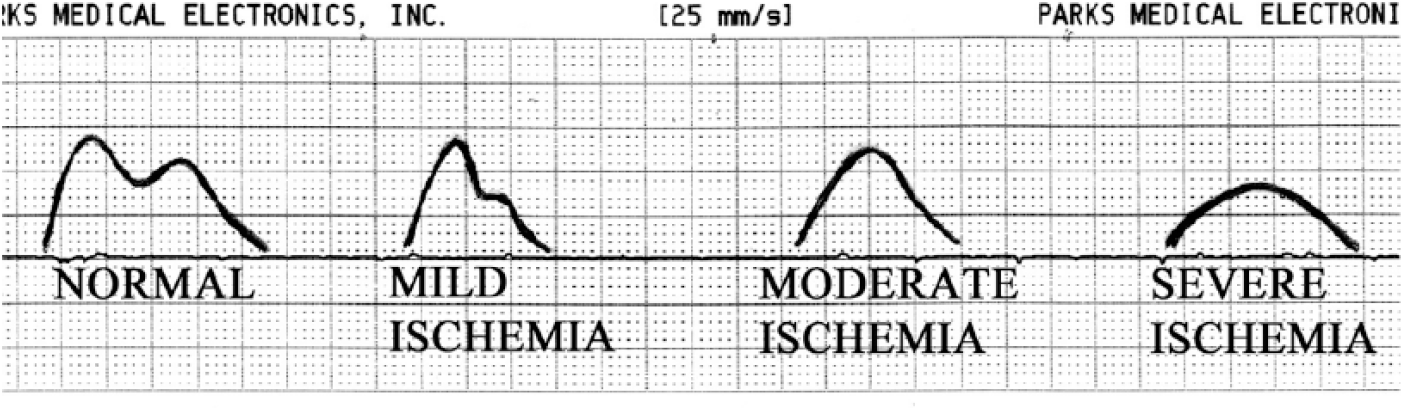
Normal and abnormal digital photoplethysmography waveforms. Adapted with permission from Kaufman and Lee. 9
Conclusion
Despite being very accurate in depicting the anatomy and often the imaging test of choice prior to surgical intervention, CTA does not reflect the functional status of the leg that is obtained via physiologic testing. Arterial duplex and physiologic noninvasive interrogations of the lower extremities provide clinicians with complementary data about the status of the arterial perfusion of the lower extremities, leading to more efficient and timely treatment of patients with advanced PAD. Regardless of being widely accepted as a screening test for PAD, the ABI has certain limitations (low sensitivity in patients with diabetes and end-stage renal disease) and possible contraindications for segmental pressures (e.g., presence of arterial grafts or fistulas below the knee, cellulitis or open wounds, and severe pain due to CLI and acute deep venous thrombosis). The referring clinicians and vascular sonographers should be aware of these possible limitations. The TBI is a valid alternative to the ABI physiologic examination, which may be used for screening purposes for the monitoring of patients with an established PAD diagnosis, especially in patients with diabetes and chronic renal disease. Considering that the evaluation of microcirculation by PPG is used for the toe blood pressure measurements (as part of the TBI test), this approach is valuable for the clinical assessment of patients with CLI.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.