
Abstract
Objectives:
The current study aims to report midterm results of patients treated with endovascular intervention, kissing stent, or covered endovascular reconstruction of the aortic bifurcation, for Trans-Atlantic Inter-Society Consensus C or D aortoiliac occlusive disease involving the aortic bifurcation.
Methods:
Eighteen patients who have intermittent claudication or chronic limb threatening ischemia with Trans-Atlantic Inter-Society Consensus C or D aortoiliac occlusive disease involving the aortic bifurcation enrolled to the study between January 2018 and January 2021. Kissing stents, Advanta V12 (Atrium, Getinge Group), were used in 13 patients, and the covered endovascular reconstruction of the aortic bifurcation technique was used in 4 patients to reconstruct the aortic bifurcation. The patients were followed for a median of 49 months (min. 2, max.58 months). Patency rates, mortality, morbidities, and reinterventions were recorded.
Results:
The mean age of the patients was 60.4 ± 10 years. Technical success was achieved in 94.4% of the patients, but one patient had to convert to open surgery. Primary patency rate of the remaining patients was 85.6% at 58 months. Target lesion revascularization rate was 11.7%. One patient had successful reintervention for in stent restenosis, and secondary patency rate was 93.3% at 58 months. Limb salvage rate was 84.6% during the follow-up. Two patients had myocardial infarction (11.1%) and one mortality (5.6%) occurred because of cerebrovascular event in the follow-up.
Conclusions:
Endovascular techniques can be used safely for reconstruction of the aortic bifurcation in Trans-Atlantic Inter-Society Consensus C or D aortoiliac occlusive disease in selected patients who have high risk for open surgery. Covered endovascular reconstruction of the aortic bifurcation is the only technique that showed patency rates approaching open surgery in treatment of aortoiliac occlusive disease involving the aortic bifurcation to date. Although promising patency results were achieved with kissing-covered stents, long-term patency rates were still lower than those achieved with open surgery. Further randomized controlled studies comparing the long-term results of these techniques are needed.
Keywords
Introduction
The treatment of peripheral arterial occlusive disease (PAOD) involving infrarenal aorta and its bifurcation is challenging. The conventional treatment modality, aortobifemoral bypass surgery, offers a 5- and 10-years patency rate up to 90% and 75%, respectively. The European Society for Vascular Surgery (ESVS) guideline recommended surgical therapies for Trans-Atlantic Inter-Society Consensus (TASC) D lesions in low-risk patients, however endovascular treatment was recommended for patients who have high mortality and morbidity risk for open surgery. 1 The Global Vascular Guidelines on the management of chronic limb threatening ischemia (CLTI) recommended endovascular treatments in the forefront for all suitable patients with aortoiliac inflow disease. 2
Kissing stents (KS) are used to treat aortoiliac occlusive disease (AIOD) for many years. In parallel with the developments in stent technology, KS are preferred in more complex lesions. Bilateral iliac stents are deployed parallelly in the aorta and inflated simultaneously while the stents’ proximal parts project into the distal aorta. Bare metal stents (BMS) were mostly used in former studies regarding KS, while covered stents such as self-expandable Viabahn® (Gore Medical, Arizona (AZ), USA), covered balloon expandable (CBE) Advanta V12® (Atrium, Maquet, Getinge Group, Merrimack, NH, USA) or BeGraft (Bentley InnoMed, Hechingen, Germany) have been used more in recent studies.3–5 The Viabahn stent that is highly flexible and The Lifestream stent (Bard, Tempe, AZ, USA) have Food and Drug Administration (FDA) approval for the treatment of patients with symptomatic iliac artery lesions. 6 The Lifestream® CBE stent is a stainless-steel stent encapsulated between two stretched polytetrafluoroethylene (PTFE) layers. 7 Another PTFE encapsulated stent, i Cover (i Vascular, Barcelona, Spain) recently received Conformite Europeene (CE) mark approval. Flexible stents can be advantageous in tortuous iliac vessels, whereas balloon expandable stents have greater radial force and allow precise stent placement. Encapsulated stents have minimal foreshortening after deployment. 6
Covered endovascular reconstruction of the aortic bifurcation (CERAB) technique was introduced in 2009. Basically, a bare or covered stent is placed in the infrarenal aorta, proximally ballooned to create a cone-shaped stent, and then two covered stents are placed in the distal conic segment at the level of the aortic bifurcation by inflating concomitantly. CERAB has the advantage of more physiological flow compared to KS because it ensures an optimal geometry that suits the aortic bifurcation. Initial studies related to CERAB technique showed a similar patency rate with KS, and midterm patency rate was approaching those of open surgical treatment. 8 Endovascular therapy may be considered as an alternative to open surgery in high-risk patient groups. 9 But there are limited studies specifically focused on lesions requiring aortic bifurcation revascularization.
The aim of the present study is to investigate midterm results of patients treated with endovascular intervention (KS or CERAB) for TASC C or D AIOD involving the aortic bifurcation.
Methods
Study design
The current study is an observational study involving 18 consecutive patients who were admitted to our tertiary healthcare center (Manisa Celal Bayar University Hospital, Department of Cardiovascular Surgery, Manisa, Turkey) with intermittent claudication or CLTI and that were treated with endovascular intervention for TASC C or D AIOD involving the infrarenal aorta and its bifurcation between January 2018 and January 2021. The study protocol was approved by the Manisa Celal Bayar University Medical Faculty Local Ethics Committee (approval number: 20.478.486) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all the participants. According to the study protocol, patients over the age of 18 years would be included. Patients with a history of cancer therapy, radiation, and hematological disorders were not included to the study. All the interventions were performed by the same vascular surgeons in a hybrid operating room with local and sedation anesthesia, and 100 units of heparin/kg was administered to the patients.
Data collection
Patients’ characteristics (age, gender, hypertension, diabetes, hyperlipidaemia, coronary artery disease, cerebrovascular occlusive disease, chronic renal failure, vasculitis, pulmonary status, and functional status), ankle-brachial index (ABI), walking distance, Rutherford category, wounds, previous interventions, medications, technical success, postoperative complications related to intervention, access site and also procedure related systemic complications, mortality and morbidities, patency rates, reinterventions, amputations, and wound healing status were recorded according to reporting standards of the Society for Vascular Surgery for endovascular treatment of chronic lower extremity peripheral artery disease. 10
Statistical analysis
The data were analyzed using SPSS (version 21.0; IBM Corporation, Armonk, NY, USA). The frequencies of the quantitative variables were expressed as mean ± standard deviation and medians, and categorical variables were shown as n (%) in Table 1. Variables were analyzed at a 95% confidence level, and p-values <0.05 were considered significant. The Normality of the continuous variables was evaluated by the Kolmogorov–Smirnov test, and Wilcoxon signed-rank test was used in comparison of ABI measurements. Kaplan–Meier Analysis was used to predict survival, patency, and target lesion revascularization (TLR) rates.
Patients’ characteristics.

ABI: ankle-brachial index; CERAB: covered endovascular reconstruction of the aortic bifurcation; n: patient number; CTO: Chronic total OCCLUSION; max.: maximum; min.: minimum; PAOD: peripheral arterial occlusive disease; SD.: standard deviation; TASC: Trans-Atlantic Inter-Society Consensus II; TLR: target lesion revascularization.
Endovascular procedures
The diagnosis, planning of the intervention, and stent sizing were done according to computed tomography angiography (CTA). Patients with chronic total occlusion (CTO) or >50% stenosis of infrarenal aorta/common iliac artery(ies) or >70% stenosis in bilateral common iliac artery based on CTA were included into the study. A routine retrograde approach from both femoral arteries was performed, and for achieving intraluminal recanalization a brachial artery access was added when needed. CBE KS, Advanta V12®, was used in 14 patients and CERAB technique was used in 4 patients to reconstruct the aortic bifurcation (Supplemental Videos 1 and 2). Stent selection was determined based on lesion characteristics. We generally selected same-sized stents based on the maximal diameter of the reference common iliac artery entrance for KS interventions. The KS protruded into the aorta for 10–20 mm. We preferred to use CERAB technique for patients who require longer protrusion into the distal infrarenal aorta. We used a bare metal self-expandable stent (Wall Stent, Boston Scientific, Massachusetts (MA), USA) in infrarenal aorta and two CBE stents (Advanta V12®) that were implanted simultaneously into Wall Stent®. The majority of the recent studies recommend using a covered stent for infrarenal aorta. But, due to restrictions in insurance policies and availability problems in our country, we used a 12 or 14 mm Wall Stent for the aortic segment. Also, bare stents in this segment allow to preserve inferior mesenteric artery flow. We performed postdilation at the proximal part of the Wall Stent to give a funnel shape.
Technical success was defined as residual stenosis <30% at completion of angiography and the completion of the procedure without complications. A pressure gradient of <10 mm Hg across the lesion was considered a hemodynamically successful result. An ABI increase of at least 0.15 was considered a clinical success. Tibial runoff score was described as good (two or three patent vessels) or poor (one or no patent vessels). The runoff vessels were considered to be patent if they had less than 50% stenosis. TLR was defined as any reintervention of target lesion or target vessel. The patients received at least 3 months of dual antiplatelet therapy and statins. The patients were followed for a median of 49 months (min. 2, max.58 months). The follow-up intervals were at 1, 3, 6, 12 months, and then yearly visits after that. Symptoms, walking distance, ABI measurement, wounds were evaluated in every visit. An arterial doppler ultrasound or CTA scan was performed when the patients have recurrent symptoms or a decrease in ABI (>0.15) was detected.
Results
A total of 14 males and 4 females enrolled in the study. The mean age of the patients was 60.4 ± 10 years. Patients’ characteristics were shown in Table 1. Most of the patients had CLTI and rest pain while three patients had ischemic wounds. Four of the patients had previous interventions due to PAOD for the aortic bifurcation or common iliac arteries. Five patients had poor distal run-off including multiple below-the-knee lesions. Technical success was achieved in 94.4% of the patients, but one patient had to convert to open surgery (aortobifemoral bypass) in the same session because reentry could not be obtained by the endovascular approach. Primary patency rate of the remaining patients was 85.6% at 58 months (Figure 1). The TLR rate was 11.7%, one patient had successful reintervention for clinically driven in stent restenosis. An intraluminal narrowing of more than 50% treated with percutaneous transluminal angioplasty with a drug-coated balloon. One patient needed aortobifemoral bypass at the sixth month of the follow-up period because of unsuccessful reintervention for in stent restenosis of a CTO lesion. Secondary patency rate was 93.3% during the follow-up (Figure 2). There was a significant improvement in ABI measurements (p < 0.001) in the follow-up, with a median reduction of two Rutherford categories (min.0, max. 4). Clinical improvement was observed in all patients, but one patient had a major amputation (5.5%) and one patient had a minor amputation (5.5%) in the follow-up. Limb salvage was achieved in 84.6% of the patients with critical limb ischemia (Table 1).

Primary patency rate of endovascular therapy in TASC C or D AIOD involving the aortic bifurcation was 85.6% (Kaplan–Meier Analysis).
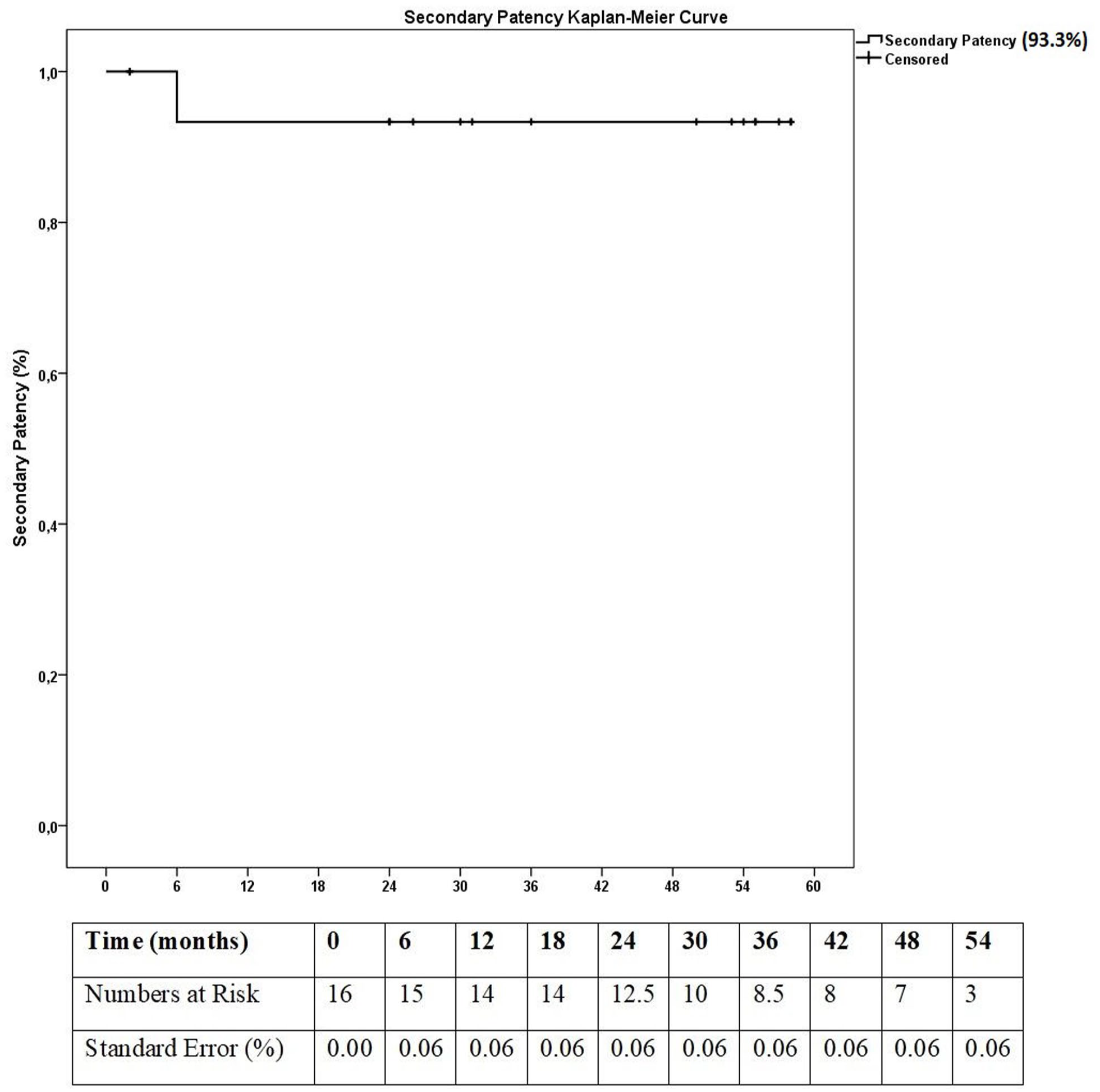
Secondary patency rate of endovascular therapy in TASC C or D AIOD involving the aortic bifurcation was 93.3% (Kaplan–Meier Analysis).
There was no in-hospital mortality and morbidity such as bleeding, pseudoaneurysm, groin hematoma, dissection, rupture, distal embolization, restenosis, stent dislocation, wound infection, contrast allergy, renal failure, and cardiovascular events. Two patients had myocardial infarction (11.1%) in the follow-up. All-cause mortality rate was 5.56% and cumulative survival was presented with Kaplan–Meier Analysis (Figure 3). A single death occurred because of a cerebrovascular event in the follow-up.

Cumulative survival (including all-cause mortality) of the study group was 94.4% (Kaplan–Meier Analysis).
Discussion
The current study showed good midterm results for endovascular treatment of patients with TASC C or D AIOD involving the aortic bifurcation. Primary and secondary patency rate of our study was 85.6% and 93.3%, respectively, for a median of 49 months follow-up. In a pooled data analysis involving 1390 patients with KS in TASC C or D lesions, technical success was 98.7% and primary patency rate at 12, 24, and 60 months was 89.3%, 78.6%, and 69%, respectively. Complication rate of this patient cohort was 10.8% which was higher than our study. 11 Pseudoaneurysm, groin complications, and distal embolization were the three most common complications. In our study, we did not observe these complications and achieved good midterm results in a small patient group. The use of CBE stents as KS may provide better patency rates in the long term. Additionally, CBE stents have the advantage of reducing distal embolization and controlling the bleeding when a rupture occurs. Some studies reported that self-expandable stents were more suitable in long tortuous iliac lesions, and balloon expandable stents were preferred in short and calcified lesions.3,11,12 In a recent review, the primary and secondary patency rates of KS at 60 months were 73% and 89%. respectively. Previous endovascular interventions were a predictor for loss of secondary patency. 13
Initial studies declared good endovascular results for TASC B or C lesions.12,14 Patency rates of self-expandable or balloon expandable stents were found similar. 15 Although there are some opponents, many recent studies comparing the results of BMS with CBE stents in AIOD, reported better primary and secondary patency rates with CBE stents, continuing up to 3 years.12,16 The use of CBE stents appears to improve patency rates. Covered stents help in excluding the thrombotic or friable plaque from the arterial flow and forms a barrier preventing neointimal tissue ingrowth. Thereby the risk of restenosis and embolization reduces.7,17 There are limited high-quality evidence related to use of CBE stents in TASC C and D lesions involving the aortic bifurcation.18,19 The first randomized controlled COBEST trial comparing BMS and CBE stents, reported that CBE stents showed superior patency in TASC C and D lesions at 18 months and showed similar patency for TASC B lesions. 17 The recent guideline of the Society for Cardiovascular Angiography and Interventions strongly recommended to use balloon expandable BMS and CBE stents over self-expandable BMS in the treatment of aortoiliac bifurcation lesions. 6 Also, CERAB technique was reported to be beneficial for the treatment of complex aortoiliac bifurcation lesions. 6 Besides these techniques, off-labeled use of Endologix Unibody stent grafts in AIOD may preserve the anatomical aspect of the aortic bifurcation and allow future endovascular interventions and crossover procedures, especially in multilevel lesions. The stent graft is protective against rupture in heavily calcified lesions. The major disadvantages of the technique are greater cost and large profile delivery system. The procedure is a challenging endovascular intervention that requires operators’ experience.19,20
Flow separation and shear stress occurring with aortoiliac KS lead to increased neointimal proliferation and thrombus formation. CERAB technique was presented as a more physiological and anatomical way of reconstruction of the aortic bifurcation. 21 Incomplete contact between stents and vessel lumen in KS configuration at the aortic bifurcation causes a mismatch area called radial mismatch. CERAB technique performed more favorable geometry than KS, showed better flow patterns in the bifurcation, and minimized the radial mismatch area.22,23 Some authors indicated a negative relationship between mismatch area and patency rates.12,23 The first large study reporting CERAB technique results, which contained mostly TASC D lesions, showed one- and two-year primary patency rates of 87.3% and 82.3%, respectively. 24 Taeymans et al. reported similar primary patency rate for CERAB at 12 and 36 months, 86% and 82%, respectively. Reintervention was required in 14% of the patients and mostly performed in the first year. Secondary patency rate in 3 years was 97%. 25 Besides, a chimney CERAB technique can be used to preserve inferior mesenteric artery flow in lesions just distal to the renal arteries. 26
The conventional treatment for TASC C and D AIOD is aortoiliac bypass surgery because of satisfactory durability. Patency rates of the open surgery range from 75% to 80% at 10 years, while secondary patency rates are higher (80%–98%). 5 Surgery has a higher mortality risk than endovascular therapy 3%–4.4% and the morbidity risk ranges between 8% and 15%.16,27,28 Lun et al. compared the midterm results of aortoiliac stenting and surgical therapy. They found a lower technical success with stenting, but a longer hospital stay and higher morbidities with open surgery. 29 Recent studies reported endovascular patency rates approximating those of open surgery for type C or D lesions.18,19,30–33 Hinnen et al. reported long-term results of KS in aortic bifurcation. Primary, primary assisted and secondary patency rate was, 70%, 81% and 91% respectively at 5 years, and 67%, 81%, and 91% at 10 years. These rates were lower than those of bypass surgery, but most of the stents were self-expandable in this study. Younger age and previous aortoiliac intervention were the major causes of reduced primary patency. TASC C and D lesions showed worse secondary patency. 3
Endovascular treatment has the advantage of avoiding abdominal incision and complications such as pulmonary disfunction, renal failure, multiple organ failure, cardiovascular events, bleeding, and wound infections. Endovascular treatments shorten hospital stay and costs, recovery time, and enable better quality of the life for the patients. 16
Study limitations
The major limitation of this study was having a small number of patients from a single-center experience. A power analysis was not performed to calculate sample size. This study was based upon retrospective data analyses of consecutive patients treated with endovascular therapy for AIOD including aortic bifurcation. Difficulty of planning randomized controlled studies causes a lack of strong evidence regarding the use of CBE stents in AIOD involving the aortic bifurcation. In addition, fixed payment policy of the social insurance system in our country, makes it difficult to calculate costs and compare it with Western countries. The approximate cost of KS application was ranging between 1000 and 1200 USD while the cost of CERAB procedure was ranging between 1200 and 1600 USD in our country.
The decision of endovascular or conventional surgery in TASC C or D AIOD should be based on individual patient evaluation regarding age, life expectancy, comorbid diseases, and limb salvage. Despite the durability of conventional surgery, there is a shift toward endovascular treatment for more complex AIOD in recent years. Our study focused on the endovascular therapy in TASC C or D aortoiliac occlusive lesions involving the aortic bifurcation and showed successful midterm results with CBE stents in KS and CERAB configuration, with patency rates approaching conventional surgery. In the present study, the CERAB technique was preferred only in patients who have serious thrombus or calcification in the infrarenal aorta; most of the distal aortic lesions could be treated with KSs projecting to the aorta at 10–20 mm.
Conclusions
Endovascular treatment of complex AIOD involving the aortic bifurcation can be performed successfully by experienced interventionists in selected patients with good technical success and low morbidity and mortality rate. CERAB is the only technique that showed patency rates approaching open surgery in treatment of AIOD involving the aortic bifurcation to date. Although promising patency results were achieved with kissing-covered stents, long-term patency rates still lower than open surgery. Further randomized controlled studies comparing long-term results of these techniques are needed.
Footnotes
Author contributions
DAS was involved in proposal and designing the study. DAS, FY and BB were participated data collection and analysis. DAS, FY, BB, ATK and OT were involved the write up of the manuscript. All authors revised the manuscript and approved the final version of the manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Manisa Celal Bayar University Medical Faculty Local Ethics Committee (Approval number: 20.478.486) and the study was conducted in accordance with the Declaration of Helsinki.
Informed consent
Written informed consent was obtained from all subjects before the study. And an approval from the director of Manisa Celal Bayar University Hafsa Sultan Hospital for archive research was obtained.
Trial registration
Not applicable. Because it is a retrospectively designed research.
Data availability
The data can be obtained from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.