
Abstract
Spigelian hernias are a rare type of lateral ventral hernia that arises through a defect in the spigelian fascia within the anterior abdominal wall. This type of hernia can be either congenital or acquired. Herniation occurs due to weakness or a defect in the transversus aponeurotic layer between the rectus abdominis muscle medially and the semi-lunar line laterally. Due to difficulty in accurately diagnosing spigelian hernias and the risk of strangulation of herniated contents, surgical repair is often recommended. A spigelian hernia case is presented in which sonography was used in the assessment and diagnosis of the abnormality. The case report highlights important diagnostic features for differentiating a spigelian hernia from other forms of abdominal wall hernia so that proper diagnosis and surgical repair can be accomplished.
Introduction
Spigelian hernias are a rare type of abdominal wall hernia involving a break in the spigelian fascia, otherwise known as the transversus abdominis aponeurosis.1,2 Spigelian hernias account for 0.12% of abdominal wall hernias 3 and 1% to 2% of hernias presented in the emergency department. 4 The risk for a spigelian hernia can be related to previous abdominal surgery or stretching of the abdominal wall. 5 Spigelian hernias are a type of ventral hernia and may be asymptomatic or present with lower abdominal pain and/or a lower abdominal lump.4,5 Rather than simply diagnosing a ventral hernia, it is important to determine what type of hernia it is in order to specify treatment options and determine the type of surgical options available. Since spigelian hernias are difficult to diagnose due to lack of unique symptoms and clinical features, it is important to know the sonographic presentation.
Case Report
A 61-year-old female with a history of an epigastric ventral hernia, that had remained stable over the past 5 years, presented to the radiology department. She had complaints of lower abdominal pain and a palpable bulge in her right lower quadrant. The patient had an extensive history of abdominal surgeries, including appendectomy, cholecystectomy, exploratory surgery, and hysterectomy. A computed tomography (CT) scan of the abdomen and pelvis was initially completed. The CT revealed a diastasis that measured up to 3 cm at the lateral margin of the rectus abdominis muscle within the right anterior pelvic wall, which contained encapsulated peritoneal fat (Figures 1 and 2). Based on the clinical presentation and the CT findings, the patient was diagnosed with a probable spigelian hernia. The physician ordered a soft tissue sonogram of the right lower quadrant to confirm the diagnosis and further assess the area for surgical treatment.
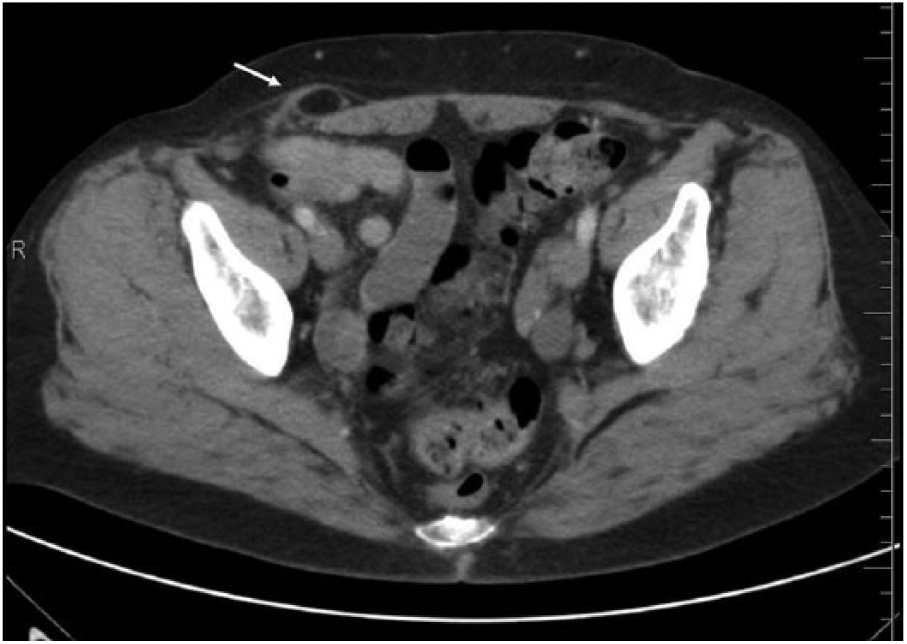
Axial computed tomogram of the pelvis showing a small pocket of encapsulated fat (arrow) visualized at the lateral margin of the rectus abdominis muscle within the right anterior pelvic wall.
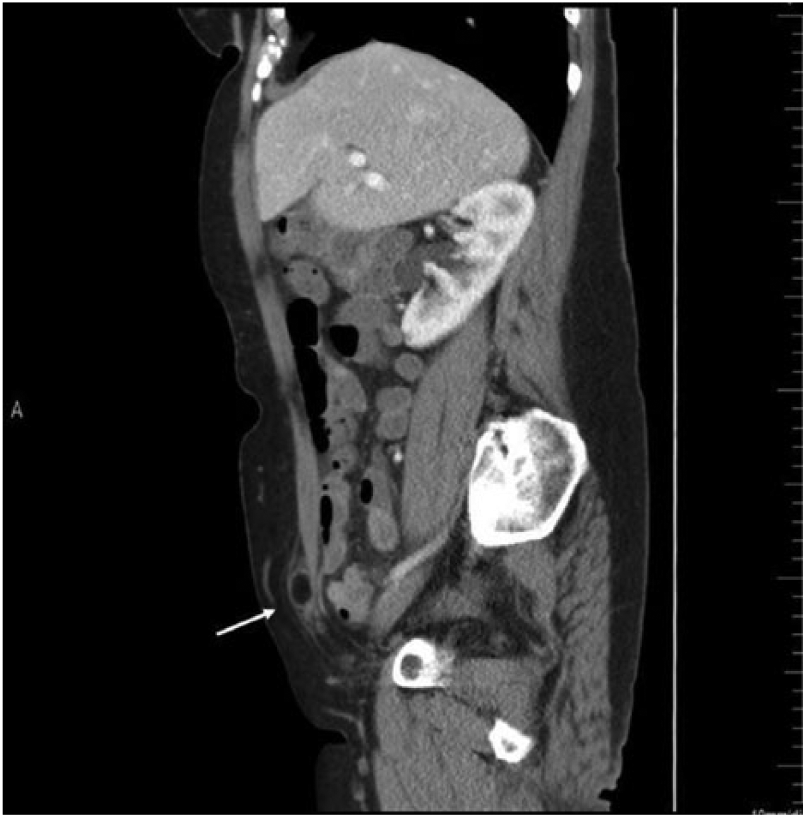
Sagittal computed tomogram of the abdomen and pelvis showing a small pocket of encapsulated fat (arrow) visualized at the lateral margin of the rectus abdominis muscle within the right anterior pelvic wall.
A soft tissue sonogram of the right lower quadrant was performed with a Philips iU22 ultrasound machine and a 12 MHz linear array transducer (Philips Ultrasound, Bothell, Washington). At the time of the sonogram, the patient denied experiencing pain in the area of the suspected hernia. Sonographic evaluation of the area of the palpable bulge revealed an interruption in the inferior margin of the transversus abdominis aponeurosis, or spigelian fascia, measuring 0.706 cm (Figure 3). The defect in the spigelian fascia demonstrated no notable vascularity with color Doppler (Figure 4). The patient was instructed to perform a Valsalva maneuver, which demonstrated the movement of the hernia contents through the defect. The lack of peristalsis within the herniated contents excluded the presence of bowel. Echogenic material was visualized within the hernia, which correlated with the encapsulated peritoneal fat shown on the prior CT. The herniated contents protruding through the defect measured 2.34 cm (Figure 5). Color Doppler evaluation of the contents demonstrated no notable vascularity (Figure 6). Based on the clinical presentation and imaging findings, the diagnosis of spigelian hernia was confirmed. Per the ordering physician’s request, the location of the spigelian fascia defect was marked using sonographic guidance, and the patient was referred for surgical repair.
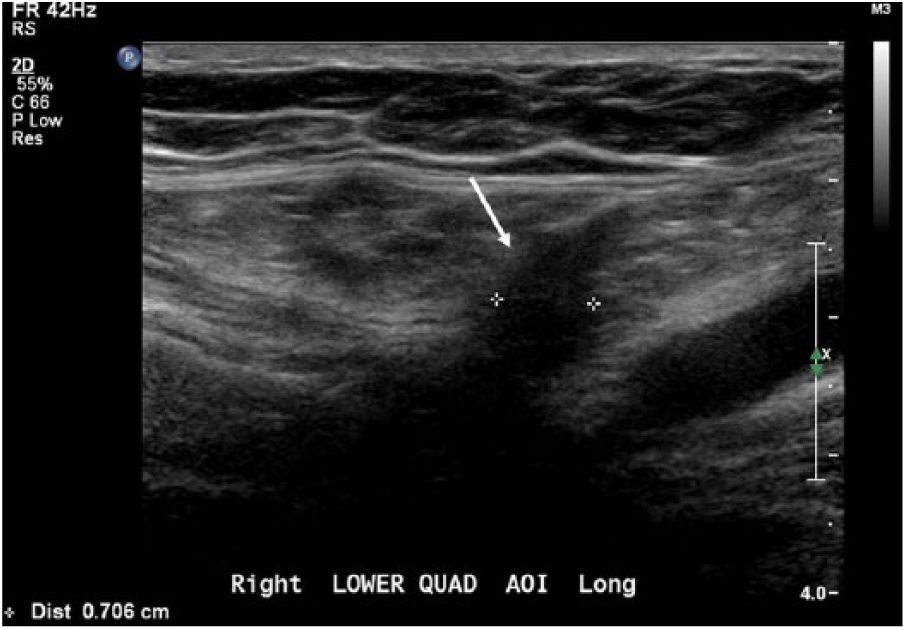
Longitudinal gray-scale sonogram of the right lower quadrant showing the interruption in the inferior margin of the spigelian fascia (arrow) measuring 0.706 cm.
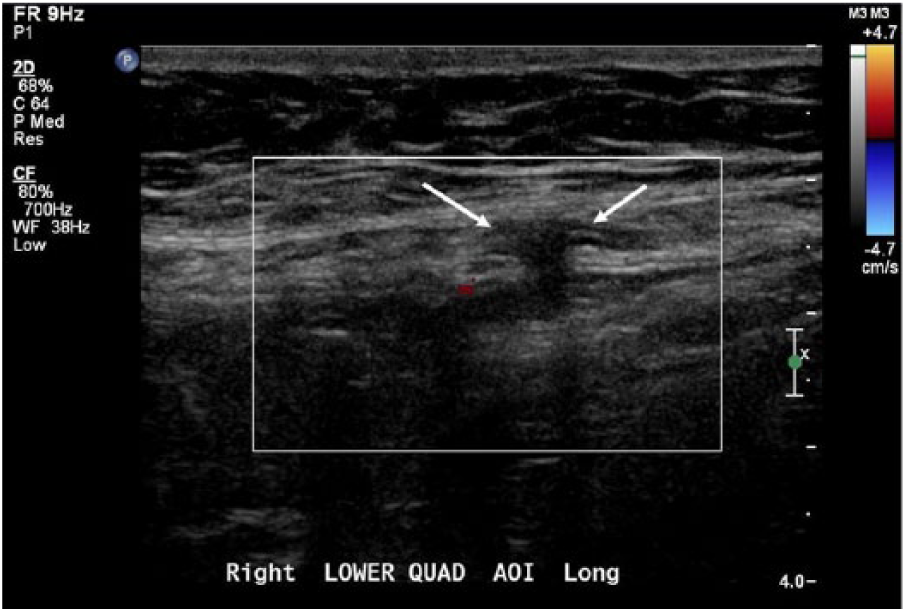
Longitudinal color Doppler sonogram of the right lower quadrant showing the defect in the spigelian fascia (arrow) demonstrating no notable vascularity.
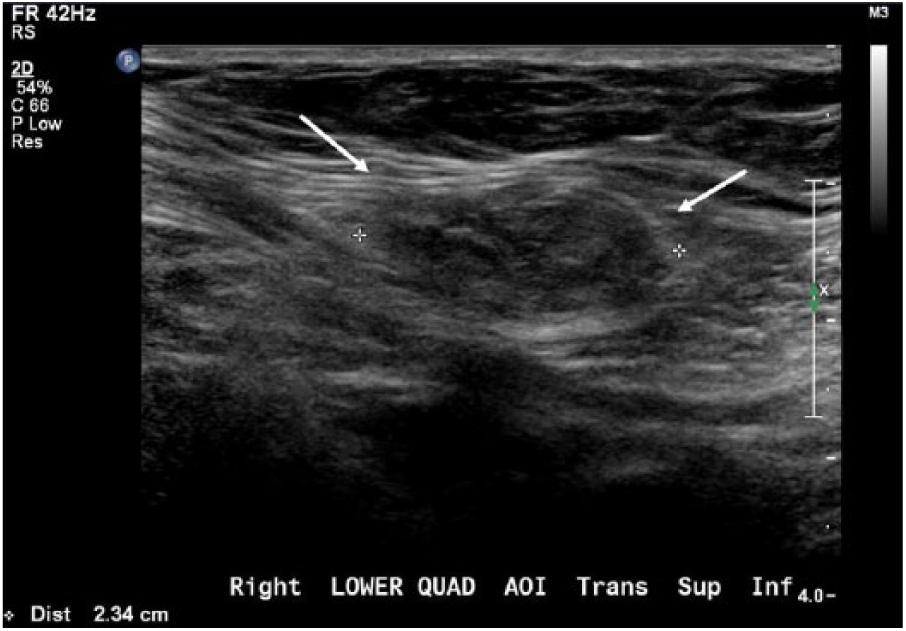
Transverse gray-scale sonogram of the right lower quadrant showing herniated contents (arrows) protruding through the spigelian fascia measuring 2.34 cm.
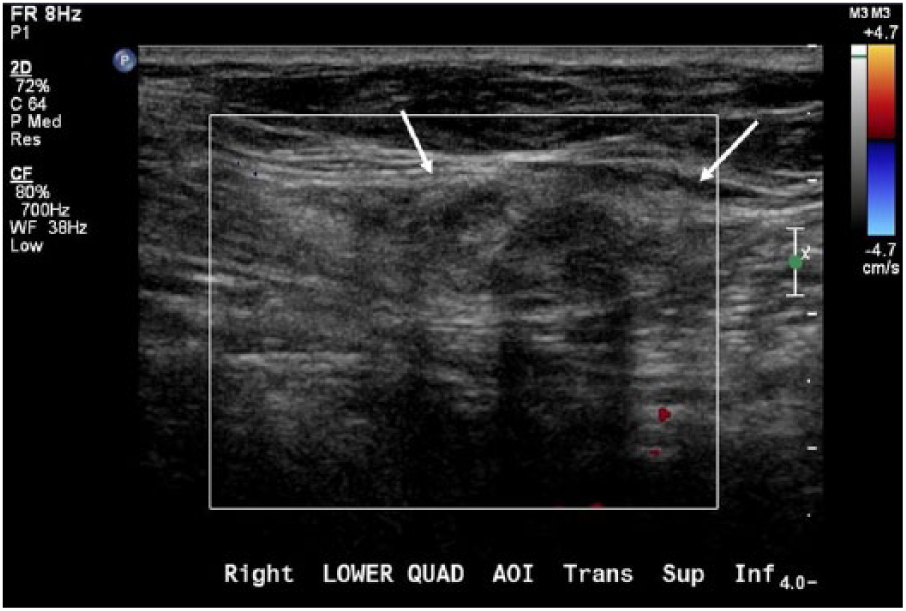
Transverse color Doppler sonogram of the right lower quadrant showing the herniated contents (arrows) demonstrating no notable vascularity.
An extraperitoneal surgical repair was performed with reduction of the incarcerated right paramedian spigelian hernia defect with mesh. During the repair, incarcerated omentum and preparitoneal fat was identified in the spigelian hernia. The fat was cut away from the hernia defect, which was then closed with a running 0 Ethibond suture. The defect was then reduced into the preperitoneal plane, and a segment of mesh was placed in the preperitoneal plane beneath the fascia. The fascial defect was closed with running interrupted 0 Ethibond sutures incorporating the fascia in the closure, which completed the repair. The external oblique aponeurosis was closed with a running 00 Dexon suture, Scarpa’s fascia was reapproximated with interrupted 000 Dexon suture, and skin was closed with subcuticularly placed interrupted 000 Dexon. Dermabond was applied as a dressing coverage. The patient tolerated the procedure well and was scheduled for a follow-up appointment 3 weeks later. The 3-week postsurgical follow-up assessment demonstrated a healed incision, and the patient reported no further problems. The patient was released for work with a lifting restriction of 40 pounds for the next 3 weeks, after which she would be unrestricted.
Discussion
The abdominal wall aids as a barrier to keep bowel within the abdominal cavity and is composed of layers of fascia, aponeuroses, peritoneum, and muscles. 6 Specifically, the transverse abdominis is a layer of muscle that lies within the anterior lateral aspect of the abdomen and deep to the internal oblique muscle.1,6 The transverse abdominis aponeurosis is also known as spigelian fascia and is involved in spigelian hernias. Normally, this fascia prevents the protrusion of bowel or fat through the area. However, when there is a break in the abdominal wall and fat or bowel protrude through the defect, an abdominal hernia is formed. Abdominal wall hernias are a common clinical problem, occurring in at least 2% of men. 7 While physical findings can diagnose a hernia, the specific type of hernia can be difficult to diagnose based on clinical presentation alone. The characteristics of specific hernias can also impact treatment options. The most common type of abdominal wall hernia is an inguinal hernia, which comprises 75% of hernias. 8 Femoral hernias are difficult to diagnosis due to their deep location within the femoral canal. Midline hernias include hernias through the linea alba and umbilical hernias. Incisional hernias form at surgical scar sites, therefore can be variable in location. Spigelian hernia is a protrusion through the linea semilunaris, which lies between the rectus abdominis muscle and internal oblique muscle. Spigelian hernias are a type of ventral abdominal wall hernia. They can be congenital or acquired but are still rare and account for less than 1% of ventral hernias. 3 When there is a defect in this muscle layer along the semilunar line and fat or bowel herniates through this break, a spigelian hernia is formed. Defects in fascia are formed by stretching of the abdomen, which results in the weakness of abdominal muscles. 4 Therefore, risk factors for spigelian hernias include prior abdominal surgeries or weight gain, which would cause stretching. Approximately 50% of the patients who are diagnosed with spigelian hernia have a history of abdominal surgeries. 4 Spigelian hernia incidence occurs more commonly in females between the age of 40 to 70 years. This type of hernia comprises 0.12% of all abdominal hernias. 5 While a spigelian hernia can present with lower abdominal pain and a palpable lump, it can also be asymptomatic, making it hard to diagnose based on its lack of unique characteristics.3,5 Nonetheless, spigelian hernias have a high incidence of strangulation, where circulation is arrested, which is irreducible, therefore proper diagnosis is essential. 8
Diagnostic imaging modalities can aid in accurate diagnosis when correlated with clinical presentation. Computed tomography and sonography are effective in aiding in the diagnosis of spigelian hernias. Evaluation with contrast-enhanced CT enables bowel content within the herniation to be identified. 5 However, sonography offers real-time imaging with patients in various positions and during maneuvers that stimulate their symptoms. The American College of Radiology’s Appropriateness Guidelines for imaging a palpable abdominal mass highly recommends a contrast-enhanced CT but does suggest sonography for pediatric and pregnant patients. 9
The sonographic appearance of a hernia includes a well-defined hernia orifice or abdominal wall defect, bowel loops or fat protruding through defect, and exaggerated movement of contents through defect with Valsalva. 5 Valsalva is an important technique used while imaging hernias due to hernias having a mobile characteristic. With Valsalva, the hernia should widen while the contents move distally, then upon release the sac will narrow.1,8,10 Spigelian hernias often pass through the abdominis transversus and the internal oblique aponeuroses, spreading out beneath the external oblique muscle or in the rectus sheath, along the rectus muscle. 5 Normally, the muscle layers would not demonstrate a visible defect; however, the peritoneal fat and bowel would be located deep to the abdominal wall. Because incarceration and strangulation of herniated contents is common with spigelian hernias, it is important to recognize the sonographic features of strangulation. The appearance of strangulation demonstrates a thickening of the sac and bowel wall, loss of normal peristalsis, and absent blood flow along with echogenicity. 8 Together, the CT and sonography offer a wealth of diagnostic information to help practitioners reach an accurate diagnosis and facilitate proper treatment for the patient. If left untreated, the risk of strangulation of the herniated contents increases, which can lead to more serious complications.
The most common treatment method for treatment is surgical repair, with several different surgical approaches available to repair a spigelian hernia. 5 The conventional approach uses a transverse incision over the defect, and the external oblique aponeurosis is incised in the direction of its fibers in order to gain access to the peritoneal sac. The sac can then be inverted, and the hernia orifice will be closed with sutures or prosthetic patch that will be placed in the preperitoneal space or above the fascia. Transabdominal preperitoneal repair reduces hernia contents along with an attempt to completely reduce the sac. A peritoneal flap is raised and is dissected about 5 cm around the hernia defect. Prolene mesh is placed in the dissected extraperitoneal space and is fixed with the use of tacks. 5 Total extraperitoneal repair creates a space by open access and a balloon. The hernia sac is identified and completely reduced. Then the peritoneum is dissected above the arcuate line to have a 5 cm margin around the defect for mesh overlap. Prolene mesh is then used to cover the hernia defect. Mesh is fixed to the anterior abdominal wall with spiral tacks. 5 In a study done regarding the diagnosis and management of spigelian hernia, 4 out of 10 of the patients followed used either the transabdominal preperitoneal or total extraperitoneal repair, all of which had successful repair and no further complications. 5
Differential diagnoses include the different types of abdominal wall hernias. Sonography helps differentiate other abdominal wall hernias from a spigelian hernia by showing the specific fascia where the defect is present. Most hernias are diagnosed by sonography. 5 In the case of a spigelian hernia, sonography will reveal a defect in the spigelian fascia along the semilunar line. This confirms a diagnosis of spigelian hernia rather than a simple abdominal wall hernia. The diagnosis of spigelian hernia relies on the hernia orifice located in the spigelian aponeurosis. 11 The key to diagnosing any abdominal wall hernia is to show movement of contents through the defect, with real-time imaging. The Valsalva maneuver helps to demonstrate widening of the defect with contents moving distally as well as narrowing of the defect with contents moving back into the abdomen, during relaxation. It is important to use sonography to assess the hernia contents in order to assess possible complications and determine appropriate treatment for the condition. 5
A previous case of spigelian hernia was diagnosed with point of care sonography. 12 A 72-year-old female with history of upper midline incision presented to the emergency department for abdominal pain and a left lower quadrant mass. An abdominal radiograph revealed dilated loops of small bowel. An emergency sonogram identified the mass as a hernia sac, within the abdominal wall. Bowel was shown to protrude through the defect and was diagnosed as incarcerated spigelian hernia. An urgent CT of the abdomen confirmed the diagnosis. Laparotomy was done, and herniated bowel was reduced in a successful repair of the hernia. 11 Another case was diagnosed with a point of care sonogram in a 60-year-old female who also presented with left lower quadrant pain. 11 The pain resolved upon examination, and the sonogram did not reveal any abnormality at the time. The patient returned 2 months later presenting with generalized burning pain in her lower abdomen. A physical examination showed a definable mass. The sonogram that was performed revealed a defect in the spigelian fascia. Spigelian hernia was diagnosed and was repaired using conventional surgical approach. 11
Conclusion
A spigelian hernia is formed when there is a weakness or defect in the spigelian fascia. This patient demonstrated a palpable bulge in the right lower quadrant. Sonography was able to confirm the probable diagnosis of a spigelian hernia by revealing the defect in the spigelian fascia in the inferior right rectus abdominis muscle along the semilunar line. Sonography also confirmed the contents of the hernia, which was encapsulated peritoneal fat. Under sonographic guidance, the spigelian hernia location was externally marked for surgical assessment, which resulted in successful surgical repair and good patient outcome.
This rare case of spigelian hernia is provided as a review for sonographers and points out the need for diagnostic information that aids in the accurate assessment and diagnosis. It is also important to determine the diagnostic features used to differentiate spigelian hernias from other types of abdominal wall hernias. Awareness of the sonographic characteristics of spigelian hernias and the use of real-time assessment and marking of the pathology enables proper repair of the defect in the specific fascia.
Footnotes
Acknowledgements
The authors thank Mary Bleckler, RDMS, RVT, for her assistance in obtaining images and information for this case study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.