
Abstract
A Spigelian hernia is an uncommon type of abdominal wall hernia that is often difficult to diagnose clinically due to its subtle presentation and deep anatomical location between layers of the abdominal wall. It is a rare type of abdominal hernia that allows abdominal contents to push through a fault in the Spigelian fascia. As such, primary care providers should consider imaging when clinical findings are inconclusive. Sonographers and sonologists should always keep a Spigelian hernia as one of the differential diagnoses for superficial masses, within the anterior abdominal wall. The present case provided is of a 65-year-old woman with a 5-year history of intermittent left lower quadrant abdominal pain. She was referred by her primary care provider, initially misdiagnosed until sonographic assessment confirmed a Spigelian hernia. This case report underscores the diagnostic value of dynamic sonography in detecting Spigelian hernias, which are often overlooked or missed.
Keywords
Spigelian hernias (SHs) account for just 1% to 2% of all abdominal wall hernias and occur more frequently in women, which can pose diagnostic challenge, due to the location and often vague clinical presentation.1 –5 It has been reported that 6 out of 10 patients, diagnosed with SH, in a specific healthcare center were women and in the sixth decade of life. 6 The term SH derives from a Belgian anatomist named Adriaan van den Spieghel, who described the semilunar line; however, the condition itself was first reported by Joseph T. Klinkosch.2,7 The semilunar line is a musculoaponeurotic band that extends from the eighth or ninth costal cartilage superiorly, to the pubic tubercle inferiorly, and lateral to the rectus muscle. 8 Spigelian fascia is formed by the aponeuroses of the internal oblique and transversus abdominis muscle in the linea semilunaris line, which marks the lateral border of the rectus abdominis muscle.7,9 The term Spigelian aponeurosis has been used in place of Spigelian fascia, due to the anatomical origin of the aponeurosis from the muscle, through which the hernia protrudes. 2 The Spigelian fascia and Spigelian aponeurosis refers to the same structure. For this case report, the term Spigelian fascia rather than Spigelian aponeurosis was chosen.
Although the fascia is generally robust, structural weak points, especially along the path of perforating epigastric vessels, can predispose it to herniation.10,11 It has been suggested that the weak spot in the Spigelian fascia, or aponeurosis, can be due to the banding of the internal oblique and transverse abdominis muscle fibers, thereby giving rise to an SH.8,12 Most SH are located within the “Spigelian hernia belt,” which is a 6-cm transverse zone above the interspinal plane (ie, the transverse plane through a line connecting the 2 anterior superior iliac spine) and below the umbilicus.2,13 –15 Spigelian hernia is also commonly known as the spontaneous lateral ventral hernia, hernia of semilunar line, hernia of the conjoint tendon, interstitial ventral hernia, interparietal, intermuscular or intramural hernia.2,8,14 The contents of SH vary and may include fat, bowel loops, omentum, or rarely even organs such as the ovary, gallbladder or appendix.16,17 Therefore, it is important to document this pathology to avoid the detrimental consequence of incarceration of the hernial contents.
Case Report
A 65-year-old woman was referred by her family physician to the ultrasound department in a tertiary care facility. She presented with longstanding left lower quadrant pain and a presumed left inguinal hernia. The patient described a dull, intermittent ache for 5 years that worsened with bending and stretching of the left lower quadrant of the abdomen and improved with rest. There was no reported history of trauma or prior abdominal surgery.
The patient was examined with a LOGIQ E10 (GE HealthCare, Wauwatosa, WI) ultrasound equipment system that had a linear ML4-20 (4–20 MHz) and hockey stick (greater than 24 MHz) transducers. The musculoskeletal and superficial system presets were applied to appropriately image the region of interest. The initial sonographic evaluation of the inguinal region did not reveal any evidence of a hernia. However, the patient identified a point of tenderness slightly superior to the left inguinal region, which was exacerbated with repeated bending. This region was felt to be lateral to the left rectus abdominis muscle, in the Spigelian belt area, therefore the sonographer suspected this to be a possible SH. When the patient was asked to bend or rotate her torso, these dynamic real-time sonographic maneuvers revealed a hypoechoic mass, protruding through the Spigelian fascia, at the linea semilunaris (see Figure 1). Transducer pressure on this hypoechoic mass did not reproduce the subjective tenderness experienced by the patient. The neck of the hernia measured approximately 7 mm in diameter (see Figure 2). The hernia was best visualized in the transverse imaging plane. The sonographer did not measure the hernial sac during the examination; however, the sonologist measured it and reported the sac to be around 3.2 cm. Color Doppler did not reveal any internal vascularity in the hernial sac. Unfortunately due to technical reasons, Doppler images were not retrieved from the picture archiving communications system. The contents of the SH appeared to be peritoneal fat rather than composed of discrete intestinal contents, due to absence of peristalsis and without the distinctive gut wall sonographic signature. Muscle herniation was also dismissed due to lack of striations in the hernial sac. The lesion was mobile, through the linea semilunaris (see Video 1, Supplemental material), reducible, and there were no signs of strangulation. The location of the lesion was crucial in differentiating this pathology from an inguinal hernia, inferiorly. Given the convincing findings, a diagnosis of a peritoneal fat-containing SH, in the linea semilunaris, was proposed; therefore, further imaging with a computed tomography (CT) was not deemed necessary. The patient declined to undergo surgery at that time and after having a discussion with her primary care provider, the patient elected to reschedule for sonographic surveillance.
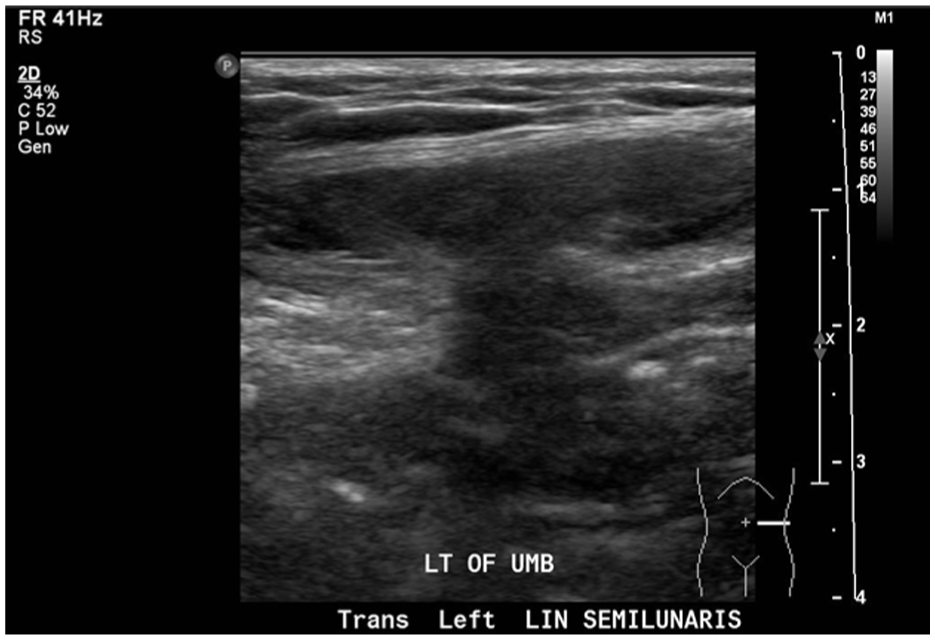
A transverse sonographic image across the patient’s abdominal wall. Note the hypoechoic peritoneal fat traversing through the defect in the abdominal wall. The defect was determined to be through the left linea semilunaris.

A transverse sonographic image across the area of the suspected hernia. A narrow neck of 7 mm, associated with the Spigelian hernia, is seen through the linea semilunaris.
Discussion
Spigelian hernias are often underdiagnosed, due to nonspecific symptoms and their deep location between muscle layers. Clinicians might not be able to palpate the SH, due to the overlying normal aponeurosis of the external oblique musculature. 18 Sonography and CT are commonly regarded as the preferred non-invasive diagnostic techniques for documenting an SH. 8 The dynamic nature of sonography, its low cost, and lack of ionizing radiation are the added benefits, compared to CT. Some consider sonography to be the first line diagnostic technique and reserve CT, as a confirmation of SH. 6 While CT is often preferred for its high specificity, high-resolution sonography, particularly paired with dynamic maneuvers such as Valsalva or position changes, offers excellent sensitivity for small hernias.9,19,20 Having the patient bend and demonstrate the Valsalva maneuver, when upright or standing, tends to increase abdominal wall pressure and can reveal subtle abdominal defects, not visible when supine or during a physical exam. 21 Diagnostic laparoscopy may rarely be considered in the patient cases that have equivocal sonographic and CT results.22,23
SH can be classified by size, as small (eg, < 2 cm), medium (eg, 2-4 cm), and large (eg, > 4 cm). 24 The European Hernia Society classifies the size of primary abdominal hernias based on the greatest width of the hernia sac, or the protruding contents. 24 They are also categorized based on their location relative to the inferior epigastric vessels. 25 Those located above are classified as high SHs, and those below are classified as low. Low SH may often be mistaken for inguinal hernias, although they are less commonly seen in clinical practice.14,25 It is unclear whether the frequency of high SHs are more prevalent than the low SHs, based on physical examination or imaging alone. In the present case, the SH was felt to be medium in size (3.2 cm) and above the epigastric vessels, thereby being classified as high SH. Spigelian hernias have also been misdiagnosed with various pathologies including a rectal sheath hematoma, appendicitis, and abdominal wall tumors. 26
Patients typically present with intermittent pain unrelated to meals, and a palpable mass is not always present. 13 A larger body habitus can obscure detection of smaller SH clinically, making the use of diagnostic imaging crucial. In this case, the hernia went undiagnosed clinically, based on physical examination, until a targeted sonogram was performed. The intensity of the patient’s pain is dependent on the contents of the SH. 7 An incarcerated bowel loop, in the SH contents, is thought to be a more pain-provoking event, compared to a nonvascular adipose tissue, in the hernial sac. Owing to its rarity in clinical practice, the diagnosis of SH might not often be considered in the differential diagnosis. 7
The cause of an SH may be either acquired and congenital. 4 Known risk factors include obesity, aging, collagen disorders, rapid weight loss, multiple pregnancies, chronic respiratory disease, trauma, iatrogenic, previous open and laparoscopic abdominal surgeries, and genetic predisposition.11,27,28 In children, a congenital origin is often suspected. 21 Due to the small neck of many SHs, there is a high risk of incarceration or strangulation.2 –4 Some have reported that in the absence of strangulation or irreducibility, symptoms tend to be activity-related and exacerbated by abdominal wall contraction. 9
Surgical repair remains the definitive treatment for an SH. 14 Since Carter et al performed the first laparoscopic SH repair in 1992, minimally invasive surgery has become the preferred approach in many centers. This is due to the fact that there is a reduced infection rate, faster recovery, decreased incidence of recurrence, low post-operative complications, and the ability to look for an incidental contralateral SH.13,29 –31 Larger SH size coupled with the increase risk of incarceration and the worsening symptomatology in the patient might be the deciding factors for an urgent surgical approach.
Conclusion
The sonographer and sonologists need to be aware of the anatomy and clinical symptomatology of SH. A patient may go undiagnosed for years, if an SH is not included in the differential, for those presenting with unexplained lower quadrant abdominal pain. This may be further complicated when symptoms vary with the patient’s movement or position. Dynamic sonography is a valuable diagnostic tool to document these types of cases. A missed or delayed diagnosis of SH can lead to prolonged patient discomfort and potential complications. Appropriate diagnostic imaging, and coordinated care between the primary and specialty providers are essential to achieving optimal health outcomes.
Footnotes
Acknowledgements
The authors would like to thank the management, radiologists, and sonographers for giving their support in publishing this manuscript with JDMS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from Research Improvements through Harmonization in Manitoba (RITHIM), dated August 5, 2025. (Harmony Project ID:0327)
Informed Consent
Written informed consent was obtained from the subject(s) before the release of the report for review.
Peer Reviewer Guarantee Statement
A member of the JDMS Editorial Board is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editorial Board member had no involvement in the decision-making process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.