
Abstract
Sonographers assume an important role in providing accurate diagnosis for prompt patient management. The manual task of scanning competency is driven by a high level of cognitive function in the form of clinical decision making (CDM). It is therefore critical that sonography students are grounded in the CDM fundamentals as part of their sonography education. The aim of this article is to seek better understanding of student views on CDM learning to inform educators of strategies to better support student learning. The first part of the article describes how CDM for sonography students is being developed at The University of Auckland. The second part of the article explores student perspectives of CDM learning and the application of CDM in the workplace. Using purposive sampling, five clinical supervisors and two students participated in semistructured interviews. Focus groups with students were conducted at the end of each semester, between July 2014 and June 2016. Thematic analysis was used to analyze and make sense of the data. Based on these qualitative findings, the authors make recommendations to advance CDM within the sonography curriculum.
Introduction
Traditionally, in sonographer training and education, there has been an emphasis on the acquisition of psychomotor skills in sonography. Due to the initial steep learning curve, sonography students have to work to become skilled at combining anatomy recognition, hand-eye coordination, and probe dexterity. Considerable attention has been directed at assisting students to attain a minimum level of clinical scanning competency, with the emphasis on the completion of sonography examinations in a timely manner. However, attention must also be paid to the development of clinical decision making (CDM) competency.1,2
Clinical decision making has been defined as a multidimensional and complex cognitive process, requiring practitioners to evaluate and make decisions3–5 that will have a direct effect on patient outcomes and quality of care. 6 Clinical decision-making competency requires a high level of cognitive skills and is closely linked to critical thinking.1,2,5 Although there has been an abundance of literature on CDM in medical and nursing education,4,7 there is a paucity of literature on CDM in sonography. 8
Importance of CDM in Sonography
Sonography is a dynamic imaging procedure. Sonographers must constantly process information while scanning a patient, in order to evaluate and make decisions. This includes asking the appropriate questions to generate hypotheses and justify scanning protocols which includes continuously evaluating and re-evaluating images to reach the final findings.1,9 Whereas sonography is a practice-based discipline, the manual task of scanning competency is driven by a high level of cognitive function in the form of CDM. Such is the importance of CDM that Penny and Zachariason 2 have defined the professional practice of a sonographer as a “cerebral occupation.” High-quality emergency care is dependent on timely and accurate CDM. 6 Sonographers are part of the conduit in providing an accurate diagnosis for prompt patient management. It is therefore critical that sonography students are grounded in the CDM fundamentals as part of their sonography education.
Successful transition from university learning to clinical practice requires more than quality teaching. It is equally important to understand students’ views and approaches toward CDM learning so as to inform educators on strategies to better support and enhance student CDM learning. This article consists of two parts: The first part describes how CDM for sonography students is being developed by the authors. The second part of the article explores student perspectives of the sonography CDM model adopted as part of a university curriculum, CDM learning, and their application of CDM in the workplace. Based on these preliminary findings, the authors put forward recommendations that could advance CDM education in sonography.
Learning Clinical Decision Making Through Social Constructivism
Constructivist learning requires students to assume an active role in learning. 10 Instead of focusing on factual recall, students are required to make sense of their own learning by questioning, analyzing, and reconciling their existing knowledge with their newly acquired knowledge. 11 As a consequence, deeper learning results as students integrate past and current experiences with their current and new knowledge. 12 Constructivism as a learning approach is most suited for CDM learning. The focus here is on applied learning with students using their current understanding and creating “new” knowledge, in the context of sonography.
Collaborative learning is an essential feature of social constructivism. Here, students learn from and learn with one another, negotiating and co-constructing their knowledge together. 12 Social constructivism recognizes that learning is a social activity and that learning must be contextualized within the social and cultural context of the profession. 13 By having students learn together, students are exposed to multiple perspectives that, in turn, broaden and deepen their understanding of shared practice.13–15 The role of the lecturer is to facilitate the collaborative construction of knowledge, with students assuming increasing responsibility of their own learning as they progress through their program of study.15,16
Using the Sonography CDM Model as Part of a University Curriculum
To sonography novices, CDM represents an elusive process that is seemingly ill-defined and poorly understood. 17 At the University of Auckland, as of July 2014, a CDM model for sonography was designed specifically to address this need by guiding students through the clinical reasoning process (Figure 1). An example of how the CDM model is used is illustrated in Table 1. During each weekly tutorial, students review three clinical request forms of varying complexity. The clinical scenarios were designed to create the ambiguity and complexity that students encounter in clinical practice.18,19 For the first 3 weeks of the semester, adhering to the CDM model, the sonography tutor role models the CDM process by making explicit his or her cognitive thoughts via the “think aloud” technique. The think aloud technique is a validated approach that has been used to capture the CDM thoughts of nurses and radiography and nursing students.20–22 Tutors verbalize their CDM thought processes, explain the reasons for their decisions, make explicit how they generate the hypothesis, and describe the conclusion of their findings. Thereafter, students take turns assuming the lead role in presenting their CDM, with the rest of the students participating via active questioning. The role of the tutor reverts to one of facilitation, prompting students on fundamental knowledge and encouraging students to think critically and to problem solve. 17 One major advantage of these tutorial sessions is the ability to provide immediate feedback on student progress and to correct student misconceptions.
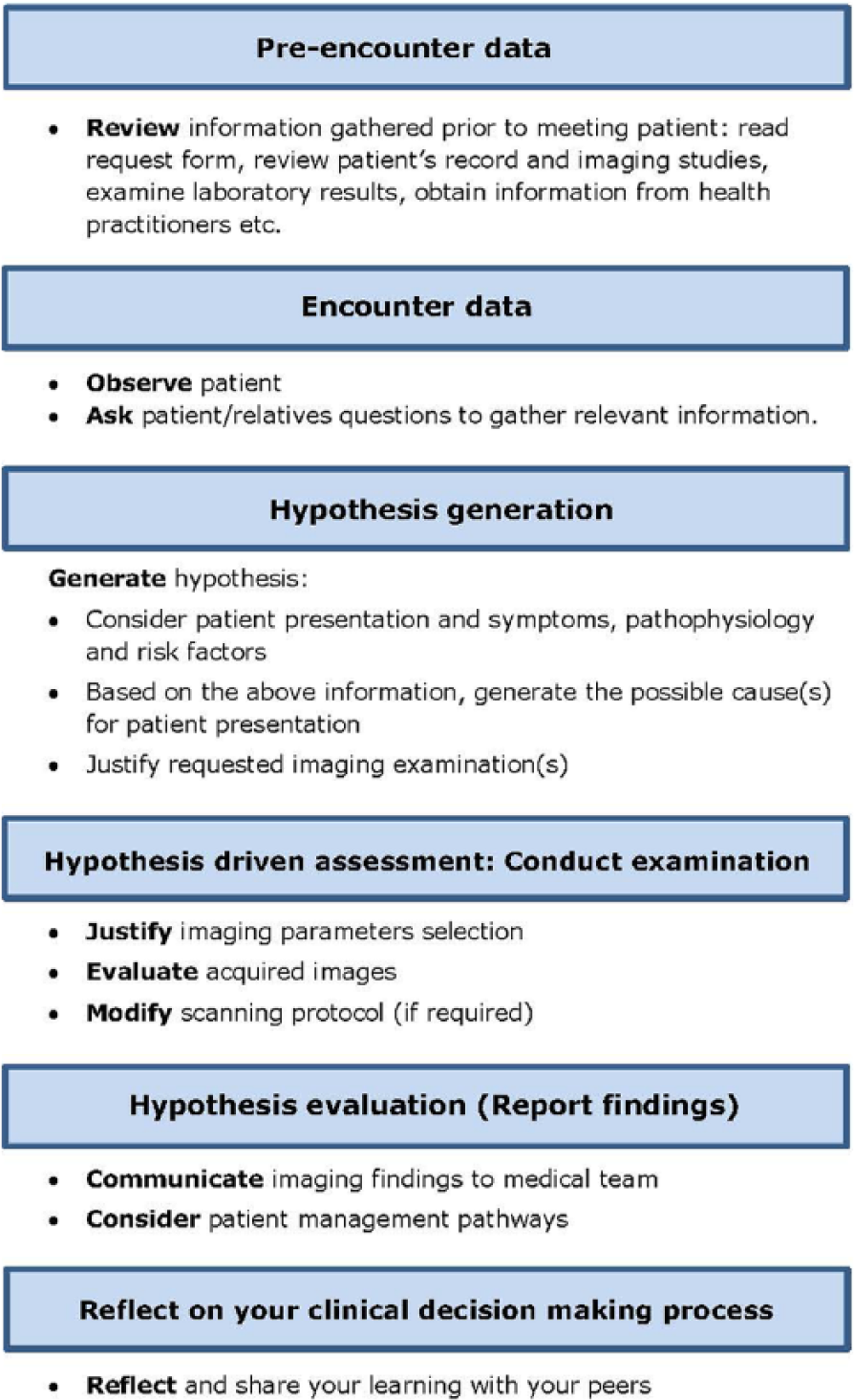
Clinical decision-making model for sonographers.
CDM Flow Chart. a
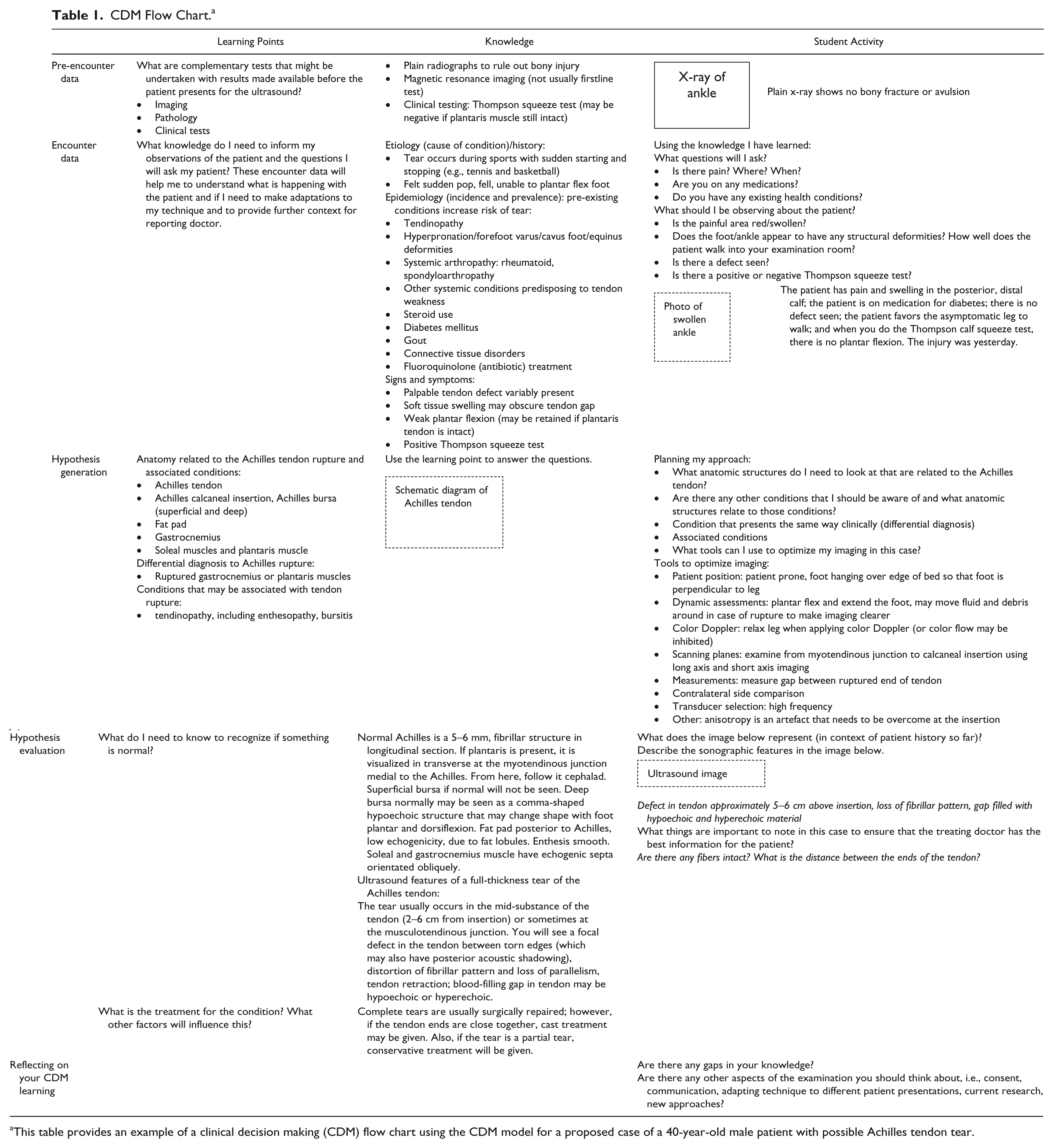
This table provides an example of a clinical decision making (CDM) flow chart using the CDM model for a proposed case of a 40-year-old male patient with possible Achilles tendon tear.
In total, students are presented with 34 clinical request forms across the semester, repeating learning activities that follow a structured framework that assists students to internalize their learning. 23 As “learning is a function of repetition,” 23 (p75) having students repeat each clinical scenario facilitates a revisiting of the CDM model, which ensures that students have multiple opportunities to practice and develop their CDM competencies. With each successive week, students create new learning by building on their previous knowledge. These repeated cognitive exercises assist students to internalize their learning. 23 As students become more familiar with the process, it enables them to focus less on the process and more on the cognitive tasks of analyzing, evaluating, and creating a repertoire of CDM pathways.
Discussion
Aside from the CDM tutorials, students are also required to complete two CDM assignments. The grades, across three semesters between 2015 and 2016, ranged from distinction to unsatisfactory (A– to D+). Of the 30 assignments submitted, 11 students (74%) improved their grades from the first to the second CDM assignments, averaging a 3.5% increase in marks. Four students (26%) scored a lower grade in their second assignments, with an average of 5% drop in performance. For the lower end of the spectrum, clinical reasoning was deemed to be “mostly sound,” albeit with relatively weak writing structure and gaps of knowledge.
To gain a better understanding of students’ views toward CDM learning, focus groups with students were conducted at the end of each semester between July 2014 and June 2016. In addition, purposive grouping resulted in a focus group of five clinical supervisors and two students who participated in semistructured interviews. Themes emerged from the analysis as a result of making sense of the data. Ethical approval was obtained by the university internal review board (Reference: 013182).
Student Feedback on the CDM Model
The CDM model adopted depicts a linear approach to CDM and, in so doing, fails to capture the multidimensional complexity of the CDM process (Figure 1). However, students concurred that the model, as a conceptual framework, serves as an effective scaffold to guide them in their CDM learning, directing them to the information required for decision making. A sample of the qualitative feedback provided is listed below:
It [the CDM model] sets a good sequence of thought processes for us. (Focus Group 1) It [the CDM model] gives you a place to start with your thought process. (Focus Group 4) It [the CDM model] does help us think laterally. . . . It is quite nice to have one little thing that’s structured, and certainly when we’ve been doing our assignments, that gives us a structure and a pathway to do that, so I think it’s great. (interview with a sonography student)
This scaffolding was especially useful during the students’ first few weeks of sonography training, assisting them to approach the patient in a holistic manner:
To discuss specific pathology, you actually have to think about the whole process. It [the CDM model] definitely was helpful early on when we had no idea. (Focus Group 4) It [the CDM model] made you think of their symptoms and their lab results and what those patients do, if they smoke or something else and what could those be, so it sort of helped you to add it all up. (Focus Group 4)
The structured approach provided by the model was particularly useful when operating under time constraints in clinical settings:
But you can always go back in that model to think about it, so we can have something to structure our thinking on, instead of just thinking anything. (Focus Group 2)
Another felt that the CDM model assisted in expanding her approach toward ultrasound examination:
This [the CDM model] is good for incorporating epidemiology as well because, before, I would never consider the patient’s age or gender as a factor as to what I might find, whereas now I would. It’s a bit more applicable in ultrasound as opposed to x-ray but, yeah, I never would have considered it before. (Focus Group 1)
The value of the CDM model was shared by a clinical supervisor, who also assumed the role of a clinical tutor at the university:
I don’t know that the students would see the benefit of it until they went back into their workplace, but I think it was really good [sic] structured, and it gave some structure to how they approach things and how they went about their learning which they could use, and a good little base of tools, then, they could take on and just adapt when they went back to their workplace. So I thought it worked actually really well. (clinical supervisor A-cum-sonography tutor)
Students’ Experiences on CDM Learning
Students expressed difficulty in synthesizing their learning into a meaningful whole. In their view, this is compounded by the fact that they did not have the opportunity to put their CDM learning into practice when scanning volunteers on campus. A sample of this qualitative feedback is provided:
And the other thing is trying to link everything as well. That’s [Getting the full picture] hard as well because [of the fragmented information,] trying to picture what you see is a challenge.
As the semester progressed, the clinical scenarios became more complex. This explains why students felt that they were always doing the catch-up game on CDM learning. The feeling of falling behind partly accounted for their lack of confidence toward CDM throughout the semester:
I think maybe we’re just very slow at the [CDM] process at the moment, like, we see something and think we are on the right track and then are we missing other things. (Focus Group 4)
Although realizing that it will take considerable time before they will feel confident and competent in CDM, this same group of students expressed their apprehension at the level of difficulty required to master CDM:
Also, people don’t realize how hard all of this is. Like, this is not a walk in the park. We were told it was hard. It’s far harder than we thought it was—honestly, it is—and so, yeah, even asking us at the end of the 2 years that same question, we may still not be fully confident, you know. (Focus Group 4)
However, some students did not perceive CDM to be too difficult, as they were already performing the pre-encounter, encounter, and hypothesis generation during their radiography days:
Yeah, as a radiographer, the first thing I would do when I was a radiographer was to look at previous imaging, and most of us had access to Concerto [clinical workstation] and you could look up what is it?—pregnancy or what were the blood results? (Focus Group 3)
The same student commented that he did not start the clinical reasoning from the pre-encounter stage. Rather, he was already thinking of technical factors and generating hypotheses well before he received the patient from the waiting room. This student’s comment stood in contrast to the anxiety expressed by students from a different cohort regarding mastery of CDM competency.
Students’ Background and CDM Learning
Not surprising, students’ professional background prior to their entry to sonography training influenced their perception of the CDM model. A student who had experiences in laboratory work found the laboratory readings required in the pre-encounter stage to be easy.
In contrast, another student from a radiography background described the pre-encounter stage to be one of the most challenging:
I mean, what do I need to look at? We’re still in the process of learning. Okay, someone said the LFT range is “this range,” but what does that mean? Where can I even look for that? So it’s one of those things I’m still trying to even gear my thought process to. (Focus Group 4)
A student who was a nonradiographer felt that the CDM model was extremely useful in developing her CDM competency. The model also assisted in providing her with a structured approach to her CDM assignment writing. This is because she was never required to make any diagnostic reasoning in her previous healthcare role, as all information was provided by the time the patients arrived for treatment:
I think it’s slightly different for me coming from [my previous role] because I didn’t do this before. . . . Yeah, the [physician] has already told us what to do and what needs to be done, so this [CDM model] for me was quite good. (Focus Group 3)
The same student went on to comment on the value of the CDM tutorials, in particular, in reference to the importance of clinical information:
I think it’s really important because I’ve never been exposed to what lab results mean or the abbreviations of all the different things that you guys [sonography trainees with radiography background] are used to. I’ve never been exposed to any of that kind of stuff, so having that [CDM tutorials] let me ask questions or for those things to come up for me to even know what they were. I think they were really good. (Focus Group 3)
Applying CDM Learning in Clinical Workplace
The value of the think aloud technique adopted during the tutorials was highlighted when students noted that in the clinical workplace, the sonographers “do it [the clinical decision making] in their head and don’t necessarily voice anything so you don’t actually know what they are thinking” (Focus Group 4).
Clark et al.
24
identified social cultural context of the workplace as one of the key factors affecting the success of CDM. This is because CDM occurs against the backdrop of social and human interactions.
24
Whereas Clark et al. focused on physicians’ CDM,
24
the same consideration of workplace culture is true of CDM in sonography. There was a consistent thread, especially within a specific cohort, expressing doubt that they may not be able to apply their CDM learning upon their return to the clinical workplace. Reasons cited included time constraints and the sonographer denying them the opportunity to perform their own CDM:
But the fact is in clinical placement, for me personally, is you got a lot of limitation on time. . . . Time is quite a luxury, ah what’s the word? Precious? (Focus Group 2) But I did think it [the CDM model] is great, but I just don’t know in the real world, when you’ve got lots of pressure time, whether you actually really have time to do that. (interview with ultrasound student)
A student provided an example of her encounter when she was back in the clinical workplace during the mid-semester break:
I just wanted to do that, like, oh, just have a quick look at previous imaging or ultrasound report, and I was just told, no, you don’t have to, just go get the patient, you know, it’s like rushed into it and wasn’t given the opportunity to even look at if they’d had any imaging done because the sonographer has already looked. But I wanted to see it for myself, or just read the report and then they would come ‘round the back and just say, this is what we’re looking at. But I’m being told by someone rather than me, myself, doing it or even reading the form. (Focus Group 2)
Another potential barrier is sonographers’ expectation of students’ involvement in CDM. Some students rightly identified the different manner in which sonographers approach CDM. Whereas most students would start CDM from the first stage of pre-encounter, they noted that sonographers, due to their experience, were able to grasp the key points without having to progress through the entire model. However, sonographers’ expectation was that students should likewise be able to follow a truncated version of the CDM process:
So a lot of the time, sonographers are actually not following the whole structure, but probably they did not get the chance to learn the structure themselves; they just learn it from the experience and they kind of, like, look at the most essential thing instead of, like, the whole structure. And for us, we tend to do the whole thing to start with, but that’s not matching what they expect us to do, so it’s kind of a conflict going on over there. (Focus Group 2)
However, for students who had the opportunity to apply their CDM learning in the workplace, feedback received on students’ performance was positive:
I had an example . . . completely unsolicited feedback, from one of the consultant radiologists we were working with, about how they thought she had an excellent approach to how she had approached the particular case and her thought processes around what she did and the conclusions that she reached. (clinical supervisor A cum sonography tutor) And I think it was quite refreshing to see especially when students came back into the workplace that they could use those [CDM] skills that they had learnt in the university. . . . So I thought that was really good. (clinical supervisor B)
Clinical supervisor C echoed the same sentiment of another student ability “to interpret the information that was given to them and also just the confidence she had with talking to radiologists.”
Student performance on CDM was summed up by another clinical supervisor:
But I think that when it came to the clinical decision making, the University of Auckland students probably had more insight. (clinical supervisor D)
Conclusion
The CDM model developed by the authors aims to facilitate the development of CDM competency in sonography. Feedback indicates that the model was successful in providing the framework to scaffold student CDM thinking, especially during the first 3 months of training. Students who did not have a radiography background rated the usefulness of the model more highly than their radiography peers. Although this finding is understandable, it follows that sonography educators will have to develop strategies to better support nonradiography students in their CDM development. There also appears to be a variation of CDM competency and confidence level even among students at the same level of training. A number of students expressed anxiety, whereas others felt sufficiently confident in their CDM learning. It is therefore essential for teaching staff to be cognizant of student motivational and affective aspects of their learning. This is because students’ positive or negative feelings toward learning are known to promote or inhibit learning.25–27
Students also expressed their concerns at their inability to apply CDM learning in their workplace. The CDM model forms part of the strategy in facilitating student transition from university learning to clinical practice. However, for a program to be of value, students must be able to apply the learning they acquired from the university at their clinical workplace. 28 The lack of opportunity to apply CDM learning at the workplace points toward the need to better support clinical supervisors to assist student learning. 8 This calls for a collaborative approach between academic institutions and the clinical workplace in order to provide a conducive environment to enable students to continue to develop their CDM competency. The qualitative analysis of these teaching approaches is a first step toward better understanding how CDM could be integrated into a sonography curriculum.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.