
Abstract
Urethral stricture in a woman is a difficult diagnosis to establish due to its rarity and clinical resemblance to bladder outlet obstruction. Imaging is used to differentiate between the various bladder, urethral, and extrinsic causes of obstruction with the standard voiding cystourethrographic examination but with little success in female patients. The following case presents complete urethral stricture in a woman, which was detected with transvaginal sonography. Transvaginal sonography is not a common modality used to assess female urethral anatomy. The urinary bladder is comfortably distended, unlike in transvaginal sonography for gynecologic indications. Urethral evaluations can be carried out while the patient strains in an attempt to void the urinary bladder. As the normal proximal urethra distends with the antegrade flow of urine during straining, the urethral caliber and wall can be evaluated to assess the level, cause, and severity of obstruction. Sonography provides the unique ability to capture a dynamic assessment of the urethra for a reasonable length of time, without the use of ionizing radiation.
Introduction
Urethral stricture is defined as an anatomic narrowing between the bladder neck and the urethral meatus, preventing catheterization with more than a 14 French catheter. 1 Usually, it is not considered clinically until it presents in a woman at risk of developing a urethral stricture. Female patients sustaining some form of urethral injury, such as multiple urethral dilatations, urethral or periurethral surgery, trauma during child birth, external beam radiation therapy for any pelvic malignancy, or history of recurrent lower tract infections, are at risk of developing urethral stricture. Surgeons have established a nonspecific diagnosis of bladder outlet obstruction based on history of a voiding problem, high residual urine in the bladder detected on sonography, and abnormal uroflowmetry findings. These can be confirmed on endoscopic (urethrocystoscopic) examination. 2 Voiding cystourethroscopy (VCUG) is the standard imaging investigation performed, although at times it may not prove useful because of failure to demonstrate the cause of obstruction. Direct visualization of the entire extent of the female urethra on transvaginal sonography (TVS) can be exploited to extract information at the site (bladder neck or urethra) and cause of bladder outflow obstruction. An attempt can be made to evaluate the urethra using TVS in women presenting with bladder outlet obstruction, especially when VCUG fails to delineate the site and cause of obstruction.
Case Report
A middle-age woman presented to the surgical emergency department with urinary retention and anuria. Catheterization of the urinary bladder was unsuccessful. The patient had a history of cervical carcinoma and had been treated with radiation therapy. The patient was asymptomatic until she developed voiding difficulties 3 years posttreatment. Previous episodes of urinary retention had been successfully treated with urethral catheterization. Because the bladder was not palpable on manual examination, a transabdominal sonography examination was obtained. Transabdominal sonography revealed a small urinary bladder with generalized thickening (posterior bladder wall thickness = 6.7 mm) and irregularity of the bladder wall with no intraluminal echogenic contents. The bladder neck had a normal appearance. Urethral catheterization was unsuccessful, even using the smallest size Foley catheter available. A suprapubic catheter was placed to decompress the bladder. The urine collected was sent for routine analysis, culture, and sensitivity to rule out presence of any infection. The urine examination was reported as normal. In lieu of the history of radiation therapy for cervical carcinoma and inability to place a Foley catheter, a clinical diagnosis of urethral stricture was considered. A VCUG was ordered to confirm the clinical diagnosis. The suprapubic catheter was clamped, and diluted nonionic iodinated contrast was infused into the urinary bladder until the patient had the urge to urinate. Voiding cystourethrography demonstrated a small-capacity bladder (Figure 1) with mild irregularity suggestive of chronic cystitis. This corresponded with transabdominal sonographic imaging findings. An attempt to visualize the posterior urethra on a straining cystogram failed. Reflux was not visualized. Subsequently, a transvaginal sonogram was obtained to image the urethral region. Transvaginal sonography revealed a small urinary bladder with a mild irregular wall thickening (Figure 2). The urethra was seen as a tubular structure with a hypoechoic central line in the proximal portion. The patient was instructed to strain for micturition and thereby distend the urethra to the level of the obstruction. The transvaginal sonogram showed a distended proximal urethra with an abrupt narrowing and nonvisualization of the distal urethral lumen (Figure 3). The normal central hypoechoic line corresponding to a normal collapsed urethra was absent and, instead, a vague hyperechogenicity, suggestive of a stricture, was noted in the distal urethra (Figure 3). The proximal distended urethra measured 7.1 mm (Figure 4). A sonographic diagnosis of chronic cystitis with urethral stricture was confirmed. Thus, TVS provided the necessary diagnostic information that had not been provided on standard VCUG. In this particular case, the transvaginal sonogram proved an excellent demonstration of a urethral stricture that caused complete urinary retention in this patient.
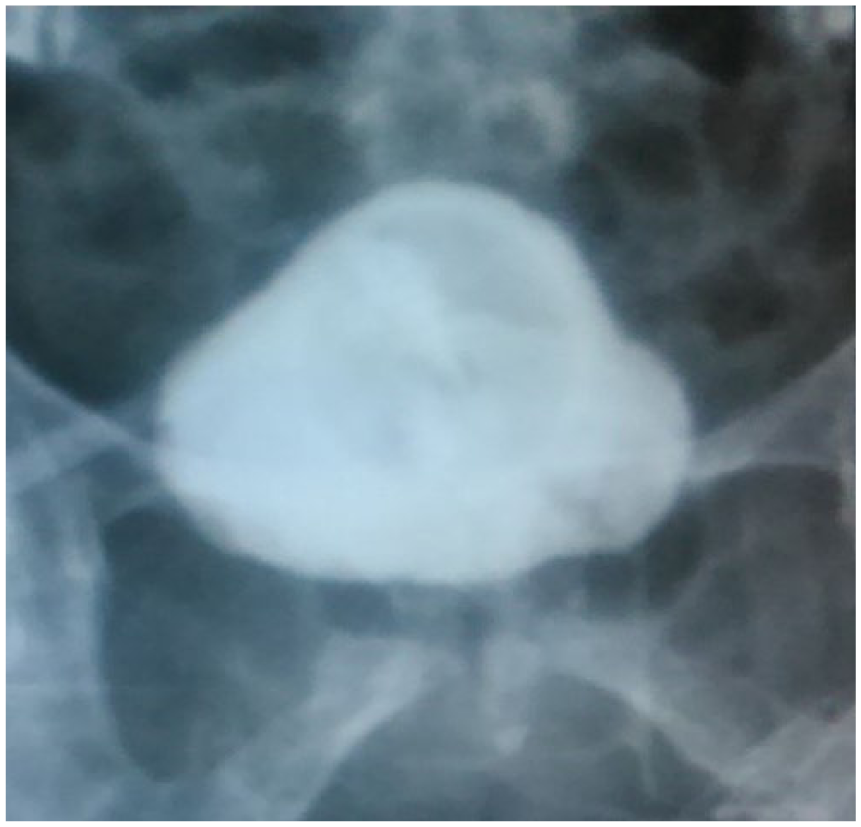
Straining cystogram showing a small-capacity bladder with a Foley catheter bulb. An irregular bladder outline is also noted. No urethra was visualized on this straining radiograph.
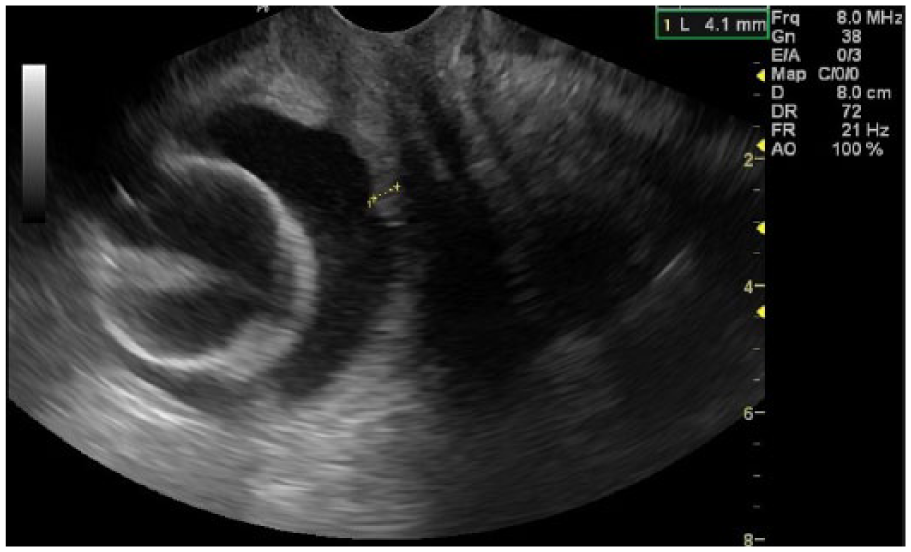
Longitudinal image on transvaginal sonogram showing a thick-walled (calipers) small-capacity urinary bladder with a Foley bulb of the suprapubic catheter seen within it. The urethra is visualized as the central hypoechoic line only in the proximal part, which terminates distally into a vague echogenicity.
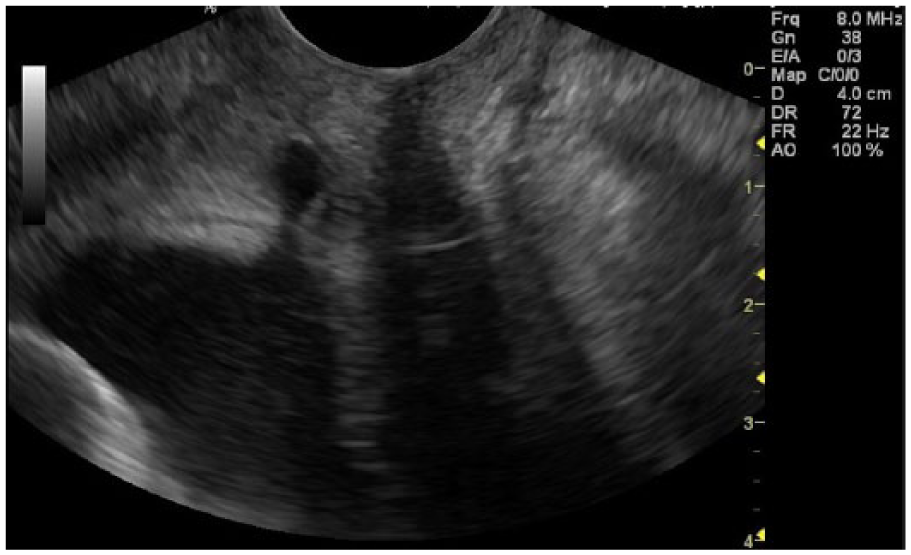
Longitudinal image on transvaginal sonogram as the patient strains, demonstrating a distended urine-filled proximal urethra, terminating as a convex bulge into a vague echogenicity, distally suggestive of fibrosis of the distal urethra. The image represents a complete stricture in the distal part of the urethra.
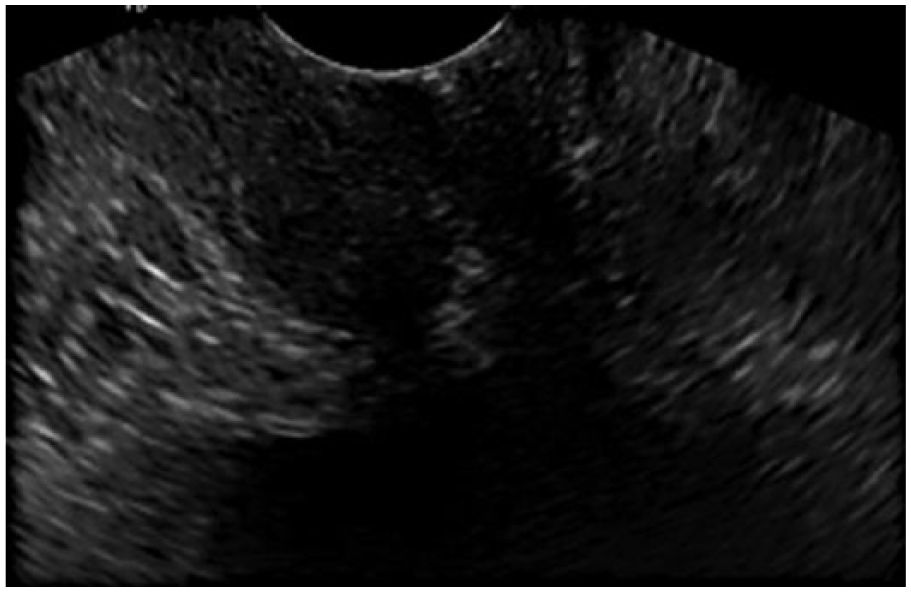
Transverse image on transvaginal sonogram as the patient strains, showing the distended urine-filled proximal urethra. The urethra measured 7.1 mm at the widest part.
Discussion
Urethral stricture is a rare diagnosis in a woman, with a variable reported prevalence of 2.7% to 29%. 3 Occasionally, female patients with urethral stricture present to the surgical emergency department with retention of urine. However, the usual clinical diagnosis is bladder outflow obstruction. A study by Groutz et al. 4 in 2000 found a prevalence of 6.5% of urodynamic outlet obstruction and 13% prevalence of urethral strictures.
Urethral stricture is an uncommon occurrence in female patients. Due to the urethra’s shorter length and straighter course, it is less prone to trauma. Greater mobility and protection by the bony pelvis also aid in reduction of trauma. 5 Very rarely, congenital stenosis could be the cause for this clinical manifestation. Acquired strictures are mostly due to trauma, infection, or inflammation 6 and commonly occur due to fibrous stenosis in the distal urethra. Stenosis usually occurs following urethral trauma due to a prolonged second stage of labor or subsequent to hormonal changes in the postmenopausal period. 2 Because the clinical diagnosis is not solely based on the patient’s reported symptoms, imaging is essential to detect the underlying cause in cases of anatomic obstruction. The bladder outflow tract may be obstructed due to pathology in the bladder, urethra lumen, or bladder wall, or even due to an extrinsic pathology within the perivesical or periurethral region. Besides urethral stricture, obstruction can also be caused by other urethral conditions such as urethral value, calculus, stenosis, caruncle, periurethral gland cyst, abscess, or urethral diverticulum. Extrinsic causes such as urethral or vaginal carcinoma, cervical fibroid, ovarian mass, ectopic ureterocele, or vaginal or paravaginal cyst may also present with lower urinary obstruction. Bladder pathologies such as bladder neck fibrosis, bladder calculi, malignancy, or a cystocele associated with uterine prolapse should also be considered. Eliciting a good history and performing a local examination are important aspects of obtaining a holistic patient history. In the clinical setting, the diagnosis of urethral stricture can be established based on voiding difficulty combined with significant residual urine detected on transabdominal sonogram and abnormal uroflowmetry. 2 Further assessment through video urodynamic studies and direct visualization on cystourethroscopy is required to confirm the diagnosis, assess the pathoanatomy in detail, and plan the management. A conventional urethrogram (consisting of retrograde urethrogram and voiding cystourethrogram) is the most common imaging investigation performed for a suspected urethral pathology. A retrograde urethrogram is difficult to do in a female patient because of anatomic and technical constraints due to a short urethral length and the diminished image resolution noted between a contrast-filled urethra and the surrounding soft tissues. 4 Therefore, the urethra is evaluated only on standard VCUG examination. A cystogram helps in evaluating the bladder for position, capacity, shape, size, outline, and lumen. In contrast, a voiding cystourethrogram helps in assessing the bladder neck and the urethral lumen. It is unfortunate that these conventional techniques are useful in only one third of the women who present with urodynamically demonstrable obstruction. 4 Nondiagnostic tests are frequently encountered due to nonvisualization of the urethral contrast resulting from air–soft tissue interface artifacts during micturition in the sitting position. 4 Often, procedural failure is attributed to a patient’s inability to micturate. Moreover, the exact cause of the obstruction may not be demonstrable. In this case study, the VCUG did not establish the cause of obstruction. Imaging techniques such as magnetic resonance imaging (MRI), which can directly visualize the soft tissue structures around the bladder neck and the urethra, can be useful in showing the specific cause of obstruction. Due to the unmatched contrast resolution, MRI has become the gold standard imaging choice for characterization of both extrinsic and intrinsic urethral pathology in female patients. 7 This is, however, balanced against the cost of MRI and its availability. Alternatively, TVS also offers high-resolution images of the bladder neck and the urethra to detect the anatomic changes of the lower urinary tract. 8 Direct imaging allows TVS to determine the cause to be extrinsic (fibroid, prolapsed uterus, tumors), in the wall (stricture or stenosis, diverticulum, caruncle), or luminal (calculus, tumor, foreign body). The level of obstruction can be determined, as was demonstrated in this study. The unique ability of dynamic scanning offers the advantage of assessment of the lower urinary tract during micturition and an enhanced opportunity to detect the cause of the voiding problem. In instances where the patient is unable to void, application of mild abdominal pressure on the distended bladder may facilitate antegrade filling of the proximal urethra 9 and therefore aid in sonographic evaluation. Other advantages of TVS are its nonionizing and noninvasive nature, patient tolerance, availability, and repeatability. A normal female urethra should be easily identified on transvaginal sonogram and appears as a tubular structure with a hypoechoic center representing the normal urethral mucosa. A hyperechoic appearance corresponding with the nondistensible urethral segment indicates a fibrotic stricture. 10 Histologically, the hyperechoic part consists of spongiofibrosis.10,11 Associated increase in color flow in the region indicates an inflammatory stricture. Another differential of urethral stenosis does not cause loss of the normal hypoechoic appearance of the urethral lumen but does affect its luminal diameter.
Brannan 12 suggested that a urethral narrowing of less than a 20 French catheter would warrant treatment. The treatment of urethral stricture includes urethral dilation, internal urethrotomy, and urethral reconstruction. 6 Dilation is the initial and most common treatment instituted for urethral stricture; however, single dilatation has a high failure rate. 13 Dilatation aims to stretch the fibrotic tissue gradually without causing trauma, to prevent inciting further fibrosis. Clinically, the stricture is mechanically dilated until minimal bleeding occurs at the site. Huang and Yang 14 have published their experience with the use of TVS in conjunction with cystourethroscopy to treat urethral strictures. The dilator is positioned in the proximal dilated urethra, under cystourethroscopic guidance, and can be further advanced into the strictured segment, under sonographic guidance. High-resolution imaging with TVS helps in visualizing the tissue planes during dilation to prevent perforation or formation of a false passage or fistula. Sonography positively contributes to an increased chance of successful dilatation.
Long-term clean intermittent self-catheterization is also a valid treatment option for partial strictures after urethral dilatation. 1 Surgical reconstruction is a difficult and less preferred option, as it is very complex and may traumatize the sphincter mechanism and cause incontinence. 15 However, surgical options are considered valid in patients with complete stricture.
Conclusion
Transvaginal sonography conducted during the straining/voiding phase of micturition is useful to capture a dynamic delineation of the urethra as it distends with urine. It can also demonstrate the presence, level, and cause of an obstructive lesion. This imaging technique offers a dynamic urethrographic examination to evaluate the female urethra, which may be difficult to evaluate on VCUG examination.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.