
Abstract
The Intersocietal Accreditation Commission (IAC) began accrediting echocardiography laboratories in 1996 to improve quality in diagnostic imaging facilities. With no existing data linking accreditation to improved outcomes, the aim of this study was to examine the perceived value of accreditation among individuals who have successfully achieved IAC echocardiography accreditation. An electronic survey was sent to accredited facilities soliciting demographic data along with questions regarding the perceived value of accreditation related to 15 quality indicators; 10.455 emails were sent with 999 responses (9.6%), and 63% of respondents reported improvement in results due to accreditation. Of the 15 quality indicators, the process was perceived as leading to improvement by a majority for 10 of the quality indicators. Nonphysicians tended to report more improvement compared with physicians (64% vs. 54%, P = .056). The perceptions from hospital-based respondents were more favorable than nonhospital-based respondents (67% vs. 59%, P < .001). More than 90% of respondents reported that maintaining accreditation was important for improved quality and better reimbursement. The study showed that IAC echocardiography facility accreditation is perceived by most facilities to improve operations for most quality indicators, particularly regarding study quality and reporting.
Introduction
The Intersocietal Accreditation Commission (IAC) began accrediting echocardiography laboratories in 1996 to improve quality in diagnostic imaging facilities by requiring adherence to the standards needed to provide high-quality care.
Echocardiography laboratory accreditation involves submission of documentation related to facility staffing qualifications, protocols, case studies, interpretive reporting procedures, and quality improvement activities.1,2 Laboratories can be part of a hospital, private practice, multispecialty clinic, freestanding imaging center, mobile service, or some combination thereof. Staffing involves physicians, sonographers, and nurses. Quality improvement activities include evaluation of variability in the performance and interpretation of a study, report completeness, correlation of findings with those from other diagnostic modalities or the operating room, and adherence to appropriate use criteria.
Despite nearly two decades of experience with accreditation, there are no data linking accreditation to improved outcomes since outcomes are difficult to assess for this process. Several studies have evaluated the attitude of health care providers toward accreditation, and a recent review highlights the limitations of accreditation, particularly in terms of the financial burden incurred by application preparation and processing fees.3,4 The IAC accreditation process is rigorous, and it is not known whether accredited facilities find the process worthwhile. Using the perceived value of accreditation among those who have successfully completed the process as a surrogate outcome of quality, the IAC performed a survey involving all accredited facilities with specific questions related to the importance of accreditation and its effect on specific quality parameters within the facility. 5 Survey results from facilities performing nuclear cardiology studies have been published, and they reveal that most physicians and other health care providers providing this service perceive an improvement in the delivery of care resulting from accreditation. 6 The results of the IAC survey, relating specifically to echocardiography, are presented in this study.
Methods
An electronic survey (SurveyMonkey™; SurveyMonkey, LLC, Palo Alto, CA) was constructed to assess the perceived effect of accreditation on quality improvement, within an IAC-accredited facility. All medical and technical directors as well as corresponding administrators at accredited echocardiography laboratories were contacted in September 2012 via email to participate in the survey. A follow-up email request was then sent a week later to all contacts who had not opened the original email invitation.
Due to the nature of the research, approval from an institutional review board was not needed as this survey was deemed an IAC continuous quality improvement project. As part of the IAC accreditation process, facilities consent to reporting of aggregate data for research purposes. The survey was sent to a list of physicians, sonographers, and administrators without intervention or interaction. Participation was voluntary, and participants were told that completion of this survey was not linked to their laboratory accreditation. No private or identifiable information was collected in the setting of anonymous participation, and the results were reported in aggregate.
The survey consisted of five categories of data: (1) screening questions to establish appropriateness and eligibility of the respondent to participate in the survey; (2) demographic information related to the role of the respondent at the facility, type and location of the facility, and duration in years of accreditation for the facility; (3) quality indicators to assess the effect of accreditation on specific quality parameters; (4) perceived importance of accreditation with the ability to write a reason for the level of importance; and (5) suggestions for improvement (Table 1). The 15 quality indicators chosen were constructed from major accreditation requirements identified in the IAC standards for all imaging divisions. The indicators were divided into four categories related to study performance, study quality, reporting, and marketing. The participants were asked to respond to a set of 15 statements that allowed them to rate the effect of accreditation on a 5-point Likert-type scale: strongly agree, agree, neutral, disagree, strongly disagree, or not applicable. Strongly agree and agree were then aggregated into one rating category as agree, and disagree and strongly disagree were aggregated into the rating category disagree. Absent and not applicable responses were excluded from the analysis. Written responses regarding the importance of accreditation were then categorized as being related to quality, reimbursement, marketing, or “other” reason.
Survey Questions and Responses.
Abbreviations: CT, computed tomography; IAC, Intersocietal Accreditation Commission; MRI, magnetic resonance imaging; PET, positron emission tomography.
In the statistical analysis, all data were expressed as the number of respondents for a particular response divided by the total number of respondents (percentage of all respondents for an individual question). Comparisons involving the responses to the questions related to quality indicators were then made between physicians and nonphysicians, among the types of practice for each facility, based on the length of time since initial accreditation, and based on the geographic location of the facility. Comparison of groups was performed using chi-square test with Yates correction. A P value of ≤ .05 was set a priori for significance.
Results
After 10.455 email invitations to participate in the survey were sent in September 2012, a second email invitation was sent to the 8081 individuals who did not open the initial request. All 999 respondents (9.6%) who completed the survey were knowledgeable about accreditation and eligible to participate. A majority of these respondents (76%) were responsible for organizing and completing the accreditation application for their facility.
Demographics
Among the respondents, a majority (82%) were sonographers, followed by physicians (12%). Facility type was evenly distributed with 44% in a hospital-based echocardiography laboratory and 43% in a private practice setting. The majority of respondents (81%) came from facilities that have been accredited for more than 3 years. Only 4% of respondent facilities were newly accredited (< 1 year). The geographic distribution of the respondents was equally dispersed across the United States, with 33% in the south, 27% in the midwest, and 26% in the northeast. Only 13% of respondents were from the western United States.
Quality Indicators
Study performance
For the three statements related to study performance, less than 50% of the respondents agreed that accreditation resulted in improvement (Figure 1): 49% reported improvement in patient safety, 45% reported improvement in laboratory efficiency, and 42% reported a decrease in inappropriate studies as a result of accreditation.
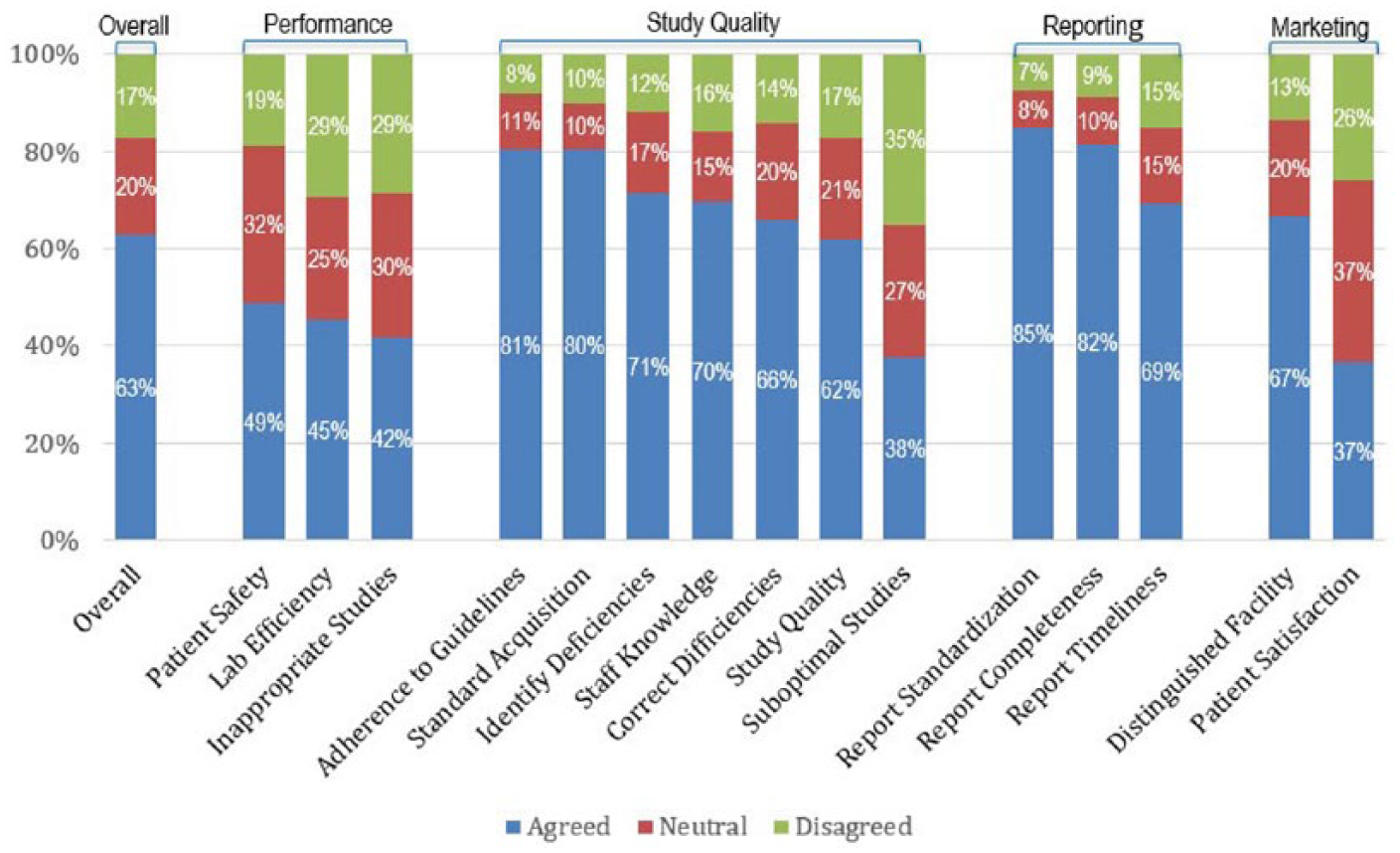
Perception of facility improvement for each quality indicator.
Study quality
Of the seven statements related to quality in image acquisition, the majority of respondents felt that improvements were related to only six of those statements (Figure 1): 80% reported increased adherence to published guidelines and standards in study acquisition, 71% reported better identification of laboratory deficiencies, 70% reported increased staff knowledge related to the procedure, 66% reported increased correction of laboratory deficiencies, and 62% reported improved image quality. It is interesting that only 38% of the respondents reported that accreditation helped to decrease the percentage of suboptimal studies.
Reporting
For all three statements related to quality in reporting, the majority of respondents agreed that accreditation resulted in improvement (Figure 1): 85% reported improvement in report standardization, 82% reported improvement in report completeness, and 69% reported improvement in report timeliness.
Marketing
For the two statements related to marketing, the majority (67%) reported that accreditation distinguished the laboratory as a quality provider for marketing purposes, and 37% reported enhancement of patient satisfaction as a result of accreditation (Figure 1).
Comparisons Among Groups
Respondent role
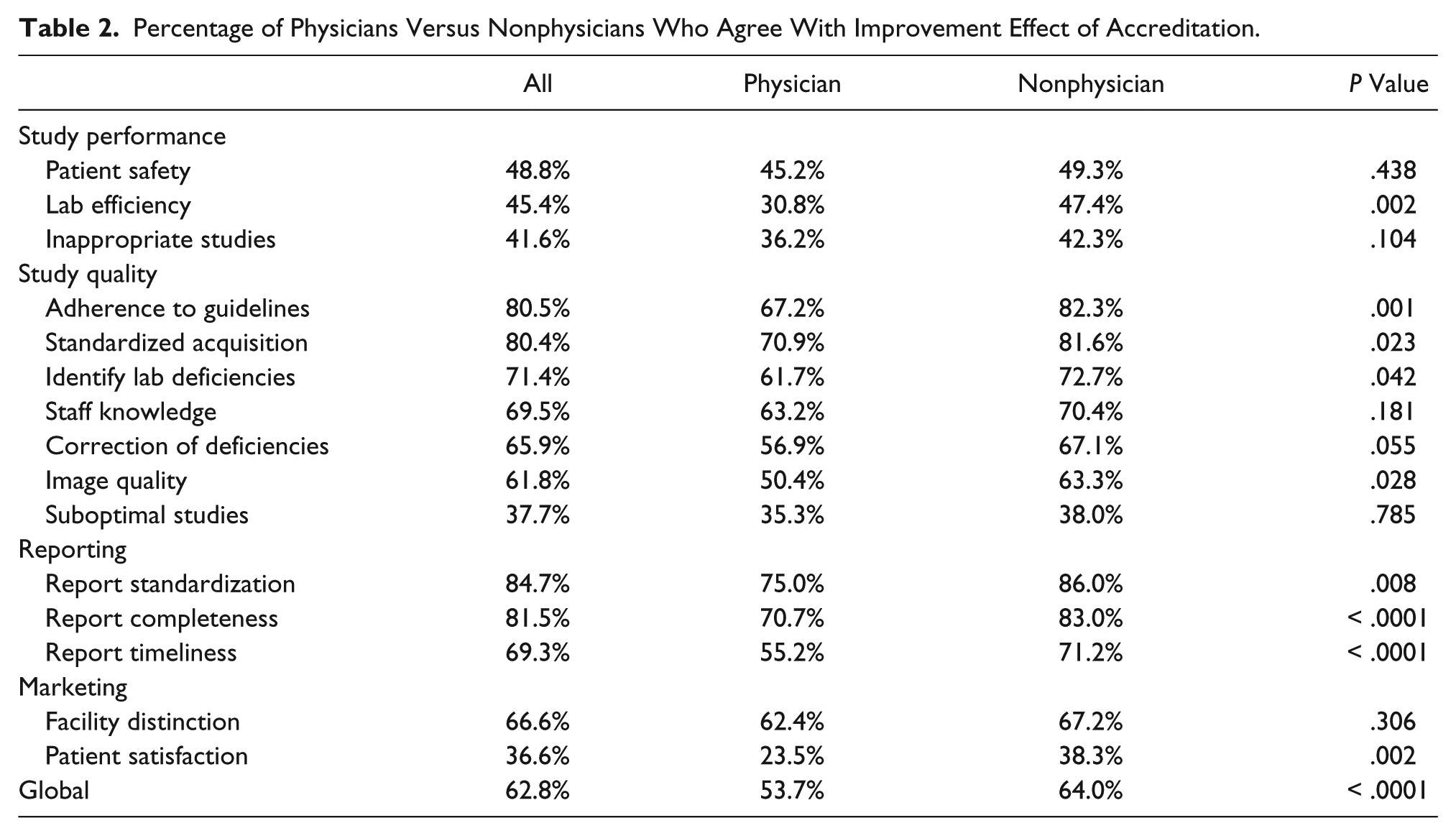
When comparing the responses based on the role of the respondent at the accredited facility, there was no significant difference between physicians and nonphysicians; however, it is worth noting that nonphysicians reported an improvement as a result of accreditation (64% for nonphysicians vs. 54% for physicians, P = .056) (Table 2). Significant differences were seen when looking at each statement within the four quality indicator categories, with more nonphysicians reporting improvement in all of the reporting indicators and most of the study quality indicators. Within the other two categories, more nonphysicians reported improvement for only those statements related to patient satisfaction and improved laboratory efficiency.
Percentage of Physicians Versus Nonphysicians Who Agree With Improvement Effect of Accreditation.
Facility type
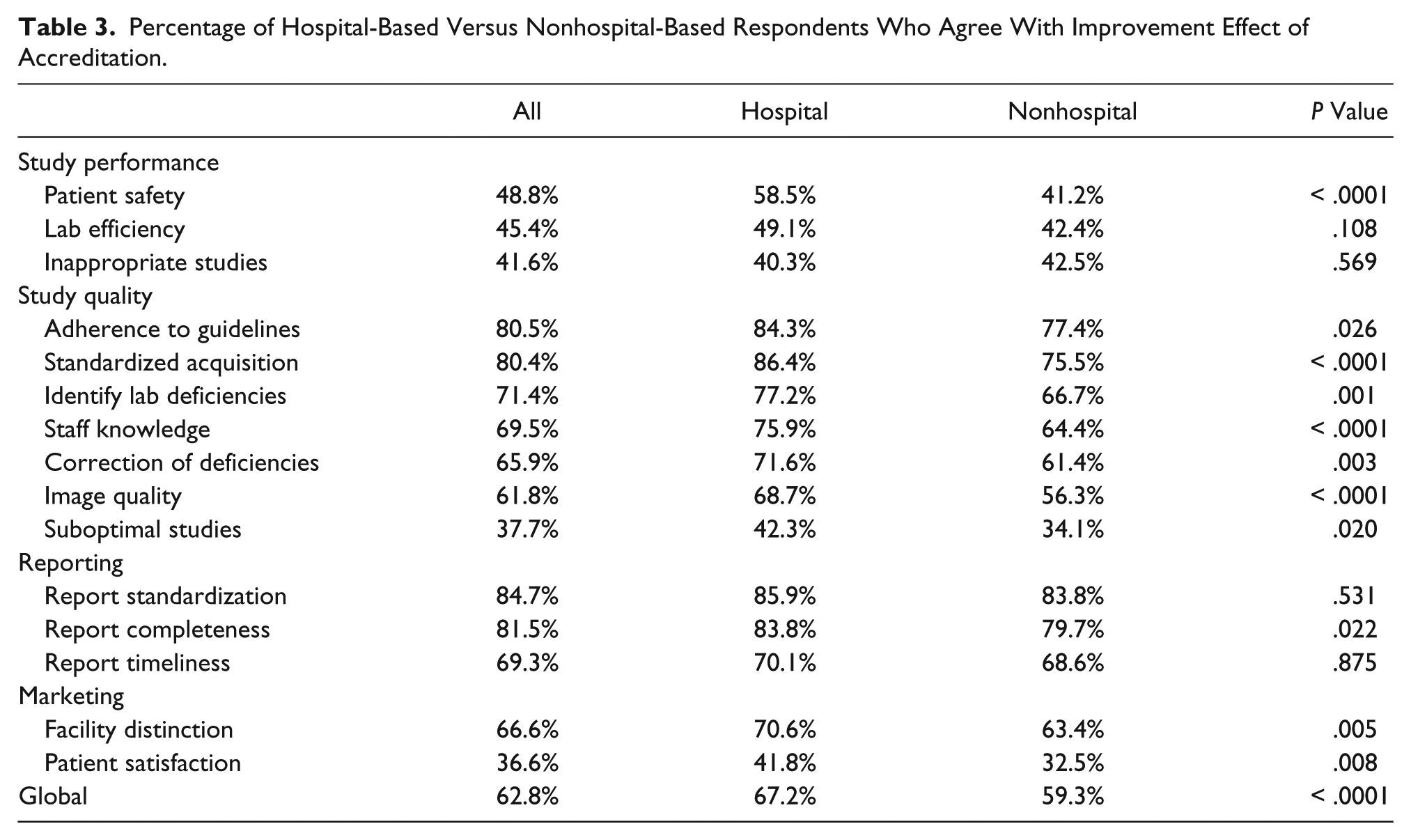
Comparison of the responses from hospital-based laboratories and those in nonhospital settings revealed more favorable perception by respondents from hospital-based settings (67% vs. 59%, P < .001) (Table 3). Significant differences were seen for all the statements in the study quality and marketing categories as well as the statement in the study performance category related to patient safety.
Percentage of Hospital-Based Versus Nonhospital-Based Respondents Who Agree With Improvement Effect of Accreditation.
Years of accreditation
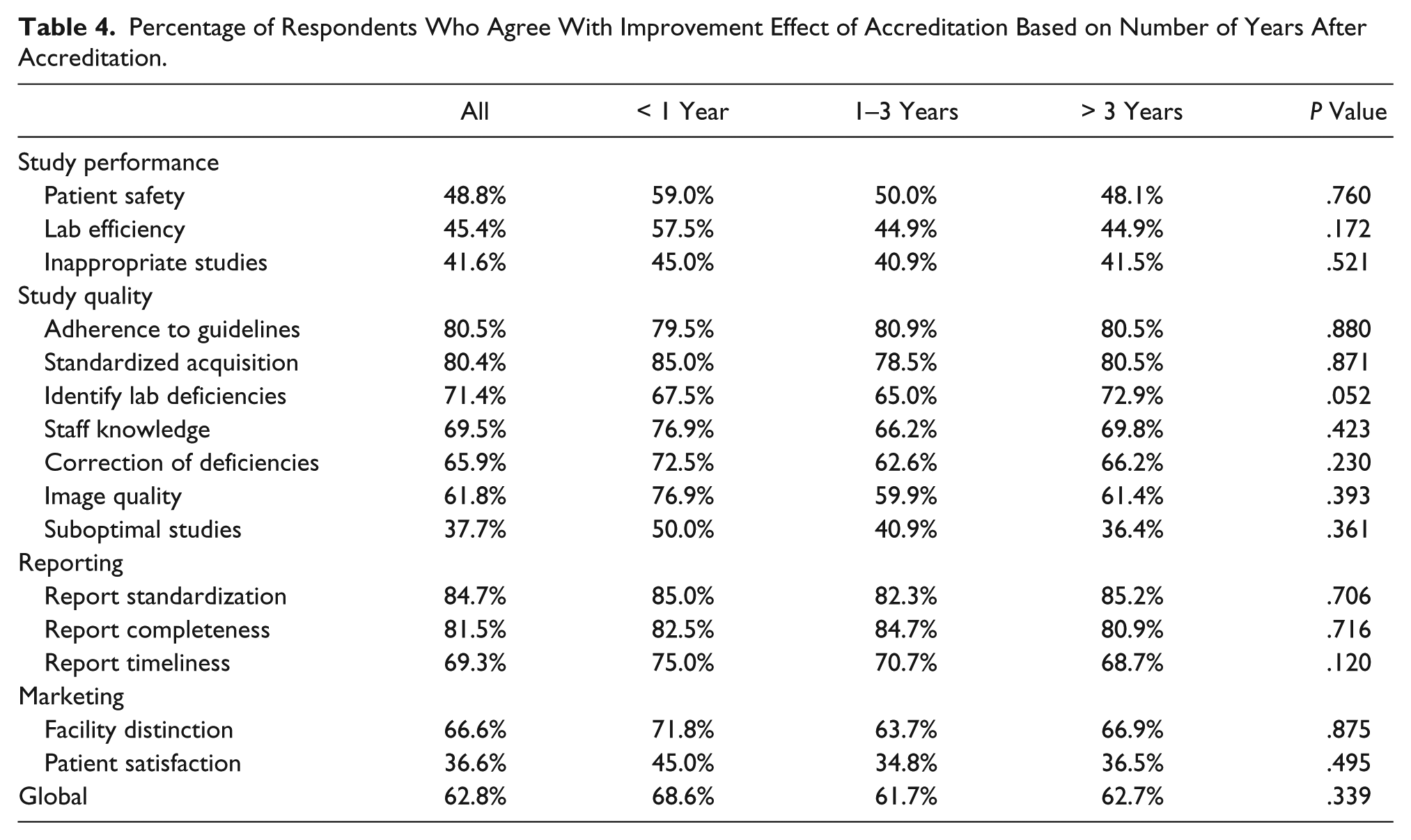
There were no significant differences in the responses of facilities based on the number of years of accreditation for all of the quality indicator statements (Table 4).
Percentage of Respondents Who Agree With Improvement Effect of Accreditation Based on Number of Years After Accreditation.
Geographic location
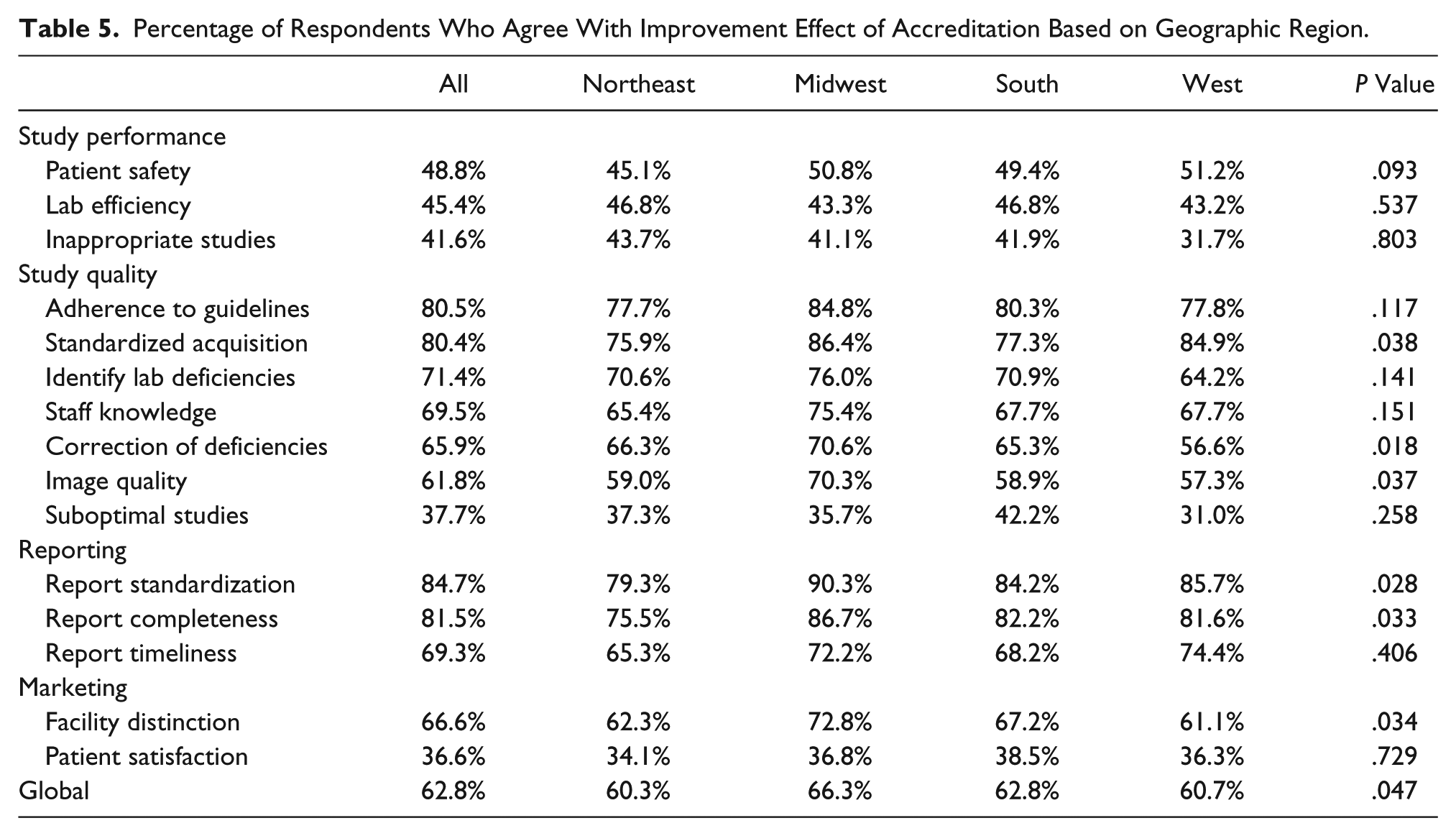
When comparing the responses to each statement based on geographic location, there was agreement that accreditation resulted in similar improvement for all responses, ranging from 60% to 66% (Table 5). For most of the statements, there were no significant differences among the facility geographic locations.
Percentage of Respondents Who Agree With Improvement Effect of Accreditation Based on Geographic Region.
Importance of Accreditation
Ninety-three percent of the respondents reported that maintaining accreditation was important to the facility, with 80% reporting that this activity was very important and 13% reporting that it was somewhat important. Only 3% of the respondents reported that accreditation was not important to the facility. Among the reasons for the importance of accreditation were quality (38%), reimbursement (36%), and marketing (14%).
Discussion
This study represents the first effort to evaluate the perceived value of accreditation in echocardiography laboratories. The process of accreditation evolved out of the growing emphasis on quality in the provision of health care services, and several documents have been published with specific guidelines related to the establishment and maintenance of quality operations in echocardiography.7,8 These documents have focused on the three broad domains where quality initiatives have their primary effect: structure, process, and outcomes. 9
The IAC was established to improve the quality of diagnostic procedures by defining standards and guidelines addressing clinical indicators in each of these quality domains. For example, organizational and structural indicators for echocardiography laboratories involve the physical space, equipment, and staffing. Process indicators involve patient selection, image acquisition and interpretation, and reporting. Outcome indicators involve diagnostic errors, associated morbidity and mortality, and patient satisfaction.
The relationship between accreditation and these quality indicators or metrics is difficult to evaluate and has not been systematically studied. However, several studies have evaluated the perceived effect of accreditation among health care providers using interviews and surveys.3,5,6,10,11 Similar studies have specifically evaluated the perceptions of nuclear cardiology and vascular ultrasound facilities. However, no studies have focused specifically on echocardiography.
The IAC survey provides some insight into the attitude of sonographers, physicians, and administrators toward accreditation of echocardiography laboratories by quantifying its perceived effect on several quality indicators. Although most of the survey questions evaluated process quality indicators such as patient selection, image acquisition, and reporting, several questions address structure indicators related to staff knowledge and facility efficiency and deficiencies as well as outcome indicators related to patient safety and patient satisfaction (Table 6).
Categorization of Quality Indicators Based on Quality Domains.

The majority of respondents perceived improvement after accreditation for the structure quality indicators involving staff knowledge as well as identification and correction of facility deficiencies, but most did not see a consequent improvement in laboratory efficiency. The latter is not surprising given the added work associated with applying for and maintaining accreditation. The majority of the respondents did see improvement for most of the process quality indicators, including image quality, adherence to guidelines and standards for image acquisition, and reporting. In fact, the quality indicators related to standardized, comprehensive, and timely reports were consistently identified as a valuable result of accreditation for echocardiography laboratories. However, most respondents did not see a reduction in the number of suboptimal studies or inappropriate studies after accreditation. The survey was conducted before the institution of the IAC requirement for quality improvement activities related to published appropriate use criteria for echocardiography,12–14 so the lack of improvement in this area is likely related to the prior IAC policy. Last, most respondents did not perceive improvement for outcome quality indicators related to patient safety and satisfaction as a result of accreditation. It is important to continue to address the elusive domain of outcomes. It is certain that it will take more than survey questions to gauge the effect of accreditation on patient outcomes. More studies are needed that could generate empirical evidence that would provide higher levels of evidence that may link accreditation to positive patient outcomes.
In this study, sonographers were more favorable than physicians with regard to most of the structure and process quality indicators, possibly because sonographers as frontline providers of the service are more directly reliant on quality indicators related to structure and process, such as standardized protocols, laboratory efficiency, and complete, accurate, and timely interpretation. Also, although most respondents did not perceive an improvement in patient satisfaction as a result of accreditation, sonographers were more likely to perceive improvement than physicians for this quality indicator.
It is interesting that hospital-based laboratories perceived greater value of accreditation than nonhospital facilities, particularly regarding study performance and quality as well as marketing of the facility. This may be related to the greater flexibility and availability of staff for processing the accreditation application in hospitals relative to smaller practices with fewer administrative support mechanisms. Hospital-based laboratories may also have had more resources to take advantage of marketing opportunities.
More than 90% of the respondents recognized the importance of maintaining accreditation, with a relatively equal number of respondents associating accreditation with improved quality and better reimbursement. This attitude is more positive than those reported previously.3,10,11 It should be noted that accreditation of echocardiography facilities as a condition for reimbursement is not mandated under the Medicare Improvements for Patients and Providers Act of 2008 as it is for computed tomography, magnetic resonance, and nuclear medicine. 15 However, echocardiography facility accreditation is required by some private insurers such as UnitedHealthcare. This may explain why echocardiography facilities view accreditation more positively.
Limitations
A major limitation of this survey research is the pre-experimental design, which has internal and external threats to validity. In addition, this study had a response rate of only 9.6% of those invited from the participant list; however, this rate is similar to other surveys that did not provide a financial incentive for participation. 16 Also, there may be an inherent bias in the type of individual who responds to an invitation to participate in a survey, although one could argue that people with positive or negative perceptions of accreditation are equally likely to respond. It should also be noted that respondents were primarily sonographers, as opposed to physicians, and most of the laboratories had been accredited for more than 3 years. This may also represent selection bias of individuals invested in the accreditation process. The study is also limited in that actual outcomes were not measured with respondent perceptions and attitudes evaluated as a surrogate outcomes measure.
Conclusion
Intersocietal Accreditation Commission echocardiography facility accreditation is perceived, by those survey participants, to improve operations for most quality indicators, particularly regarding study quality and reporting. In addition, these respondents recognized the importance of maintaining accreditation from the standpoint of quality, reimbursement, and marketing.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Mary B. Farrell, MS, and Gary V. Heller, MD, are employees of the IAC. Leo Lopez, MD, John Y. Choi, MD, Kevin M. Cockroft, MD, Heather L. Gornik, MD, Scott D. Jerome, MD, and Warren J. Manning, MD, are IAC board members and members of the IAC Research Committee.