
Abstract
We examined the IAC-Echocardiography applications database to describe the board certification of physicians and registration of sonographers and explored how staff credentials affected initial laboratory accreditation decision. Deidentified IAC-Echocardiography applications from January 2012 to December 2013 were reviewed, including size and setting of echocardiography laboratories, National Board of Echocardiography (NBE) testamur status of physicians, and registered credential status of sonographers. Multivariate logistic regression models evaluated associations between echocardiography laboratory characteristics and accreditation and deficiencies in peer-reviewed domains (staff, imaging protocols, image quality, reporting, and quality assurance) of accreditation. During the study period, 1921 echocardiography laboratories representing 10 602 physicians and 6841 sonographers applied for IAC-Echocardiography accreditation; 26.9% of physicians were NBE testamurs and 79.5% of sonographers were registered. NBE status of medical directors did not reach statistical significance for accreditation success (AOR 1.15 [0.93-1.42]), but number of registered sonographers per applicant did (AOR 1.13 [1.04-1.23]). NBE testamur medical directors were associated with fewer deficiencies in image quality (AOR 0.61 [0.48-0.79]) and reports (AOR 0.72 [0.56-0.92]). Applicants whose technical director was a physician rather than a sonographer were more likely to have deficiencies in image quality (AOR 1.84 [1.06-3.21]). Registered sonographers were associated with fewer deficiencies in the domains of staff credentials (AOR 0.84 [0.78-0.92]), reporting (AOR 0.88 [0.81-0.96]), and quality assurance (AOR 0.91 [0.84-0.98]). Registration status of sonographers, but not NBE testamur status of physicians, was positively associated with accreditation decisions. The overall interaction between individual certification and laboratory accreditation suggests a complementary role for both.
Introduction
Accreditation of echocardiography laboratories and certification of professionals who perform and interpret echocardiography are advocated by many stakeholders as key components of quality imaging services.1,2 Medicare carriers and private payers are increasingly linking both specific physician certification and laboratory accreditation to reimbursement3-5 but data linking these credentials to quality care are few. 6 The National Board of Echocardiography (NBE) administers an examination of special competence in adult echocardiography for physicians as the first step in a two-step program of certification in echocardiography; physicians who successfully pass the examination are referred to as “NBE testamurs” who may then apply for “NBE certification” by submitting case logs and professional references. Both the American Registry for Diagnostic Medical Sonography (ARDMS) and Cardiovascular Credentialing International (CCI) offer registry examinations for sonographers. The Intersocietal Accreditation Commission for Echocardiography (IAC-Echocardiography), a nonprofit organization, is currently the only organization accrediting echocardiography laboratories. 5 IAC-Echocardiography accreditation is a peer-review process evaluating staff training and continuing education, application of guidelines from professional societies and the IAC Standards 7 in a lab’s protocols and sample echocardiograms, use of a structured report, and quality assurance policies. 8 The interaction of facility accreditation and individual personnel certification in echocardiography has not been studied.
We sought to examine the IAC-Echocardiography applications database to describe the training and credentials of physicians and sonographers practicing adult echocardiography and explore whether board certification of medical directors and registration of sonographers were positively associated with IAC-Echocardiography initial application success or peer-reviewed measures of echocardiography laboratory quality.
Methods
Study Type and Inclusion Criteria
This was a cross-sectional study using all IAC-Echocardiography applicants for adult echocardiography accreditation in the United States during the cycle spanning January 2012 to December 2013.
Data
Deidentified laboratory data were provided on each IAC-Echocardiography applicant directly from the Intersocietal Accreditation Commission. On the application, echocardiography laboratories self-report their setting (hospital or nonhospital) and annual volume of echocardiograms performed: adult transthoracic echocardiograms (ATTE) and transesophageal echocardiograms (TEE) and stress echocardiograms (SE) when applicable. Additional characteristics of the applicant collected included number of sites, the number of previous accreditation cycles, concurrent application for TEE or SE accreditation, the number of sonographers, number of registered sonographers, number of physicians, physician credentials and training pathway, physician NBE testamur status, and use of a consultant. Physicians were defined as NBE testamurs if they reported successful completion of the NBE examination, whether or not they had also completed the NBE certification process, following the definition used by the NBE; 1 NBE certification status, which is distinct from testamur status in that it requires case logs, training verification, and professional references in addition to a passing score on the examination, is not collected on the IAC-Echocardiography application. Table 1 lists the medical director, medical staff, technical director, technical staff certification/credentialing options and qualification pathways.
Staff Certification/Credentialing Options and Qualification Pathways.
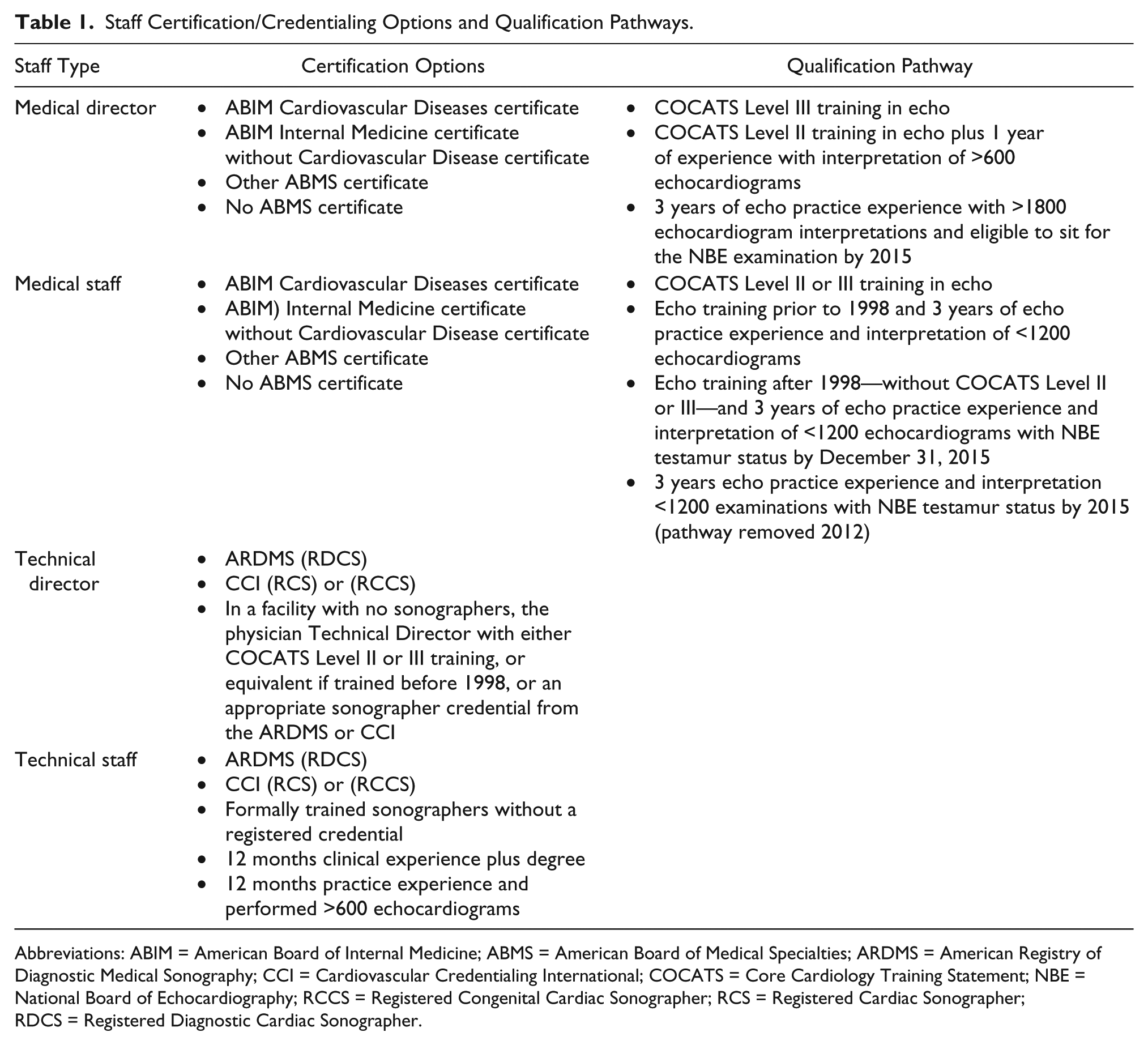
Abbreviations: ABIM = American Board of Internal Medicine; ABMS = American Board of Medical Specialties; ARDMS = American Registry of Diagnostic Medical Sonography; CCI = Cardiovascular Credentialing International; COCATS = Core Cardiology Training Statement; NBE = National Board of Echocardiography; RCCS = Registered Congenital Cardiac Sonographer; RCS = Registered Cardiac Sonographer; RDCS = Registered Diagnostic Cardiac Sonographer.
Five domains are evaluated as part of the IAC-Echocardiography peer review: (1) adequacy of staff credentials; (2) ATTE imaging protocols; (3) sample ATTE image quality; (4) ATTE report accuracy, completeness, and timeliness; and (5) quality assurance procedures (Table 2). Because ATTE was the primary modality of interest, we classified reasons for delay as ATTE-specific within the five peer-reviewed domains or organizational, such as policies for verification of staff credentials and addressing patient complaints.
Peer-Reviewed Domains of Accreditation.
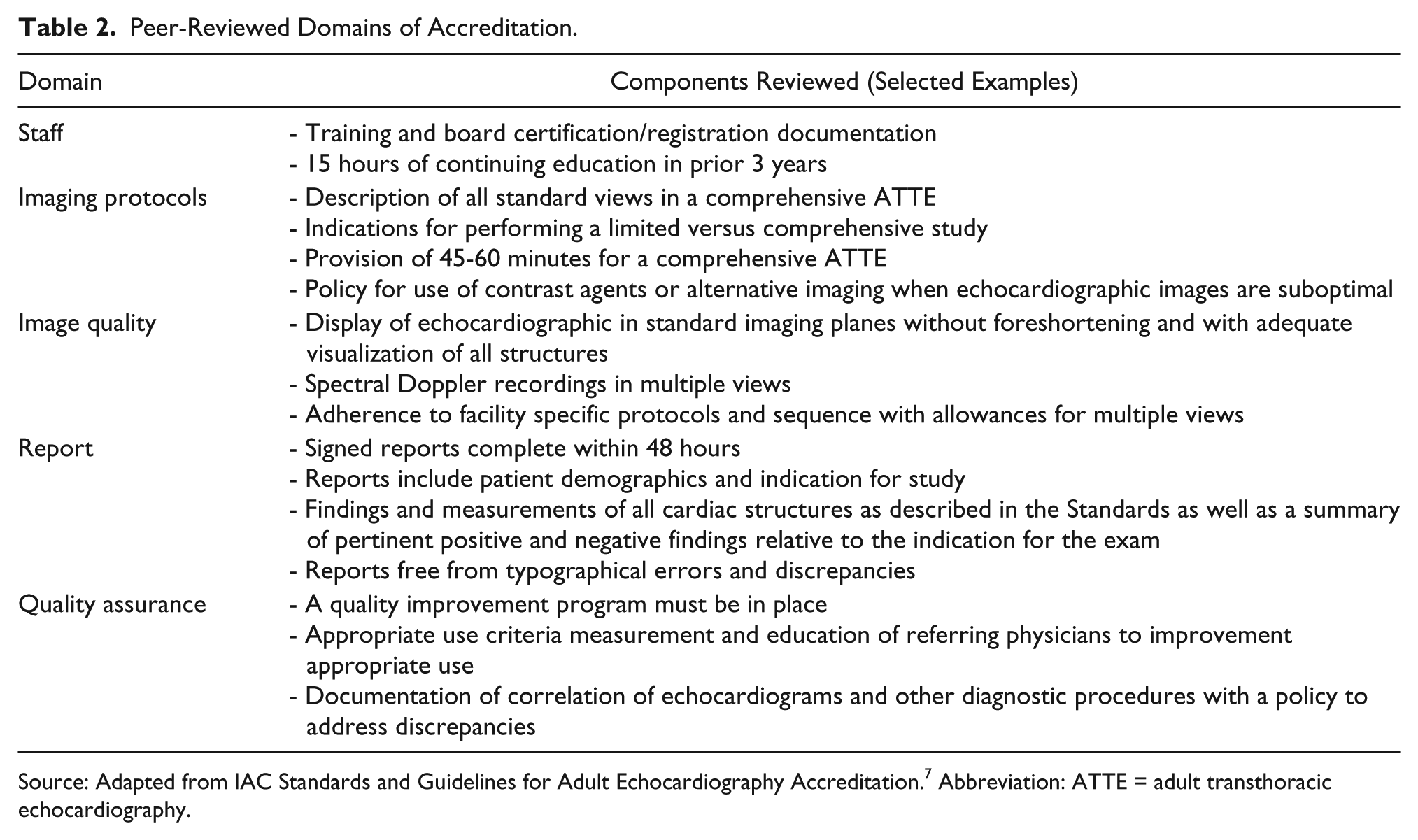
Source: Adapted from IAC Standards and Guidelines for Adult Echocardiography Accreditation. 7 Abbreviation: ATTE = adult transthoracic echocardiography.
Statistical Analysis
Echocardiography laboratories may apply for ATTE alone or in combination with TEE or SE; accreditation is granted for these secondary procedures only if and when an echocardiography laboratory is granted accreditation for ATTE. ATTE was therefore used as a surrogate for echocardiography laboratory accreditation and TEE and SE accreditation decisions subordinate to it in the analyses. Applicants were categorized into two groups based on initial ATTE accreditation decision, granted versus delayed. Characteristics of the applicants were summarized descriptively and compared using chi-square and t-tests or Mann-Whitney tests (based on distribution).
The dependent variable for the primary analysis was initial ATTE accreditation decision. We subsequently explored reasons for delay in each of the five peer-reviewed domains of ATTE accreditation as dependent variables. Laboratory characteristics provided on the IAC-Echocardiography applications described above were used to adjust each of these analyses through multivariate logistic regression. We also performed exploratory analyses of TEE and SE peer-review findings among those applicants also seeking TEE or SE accreditation. For all of these models, univariate analyses were first conducted using the above describe laboratory characteristics to identify independent variables with a P value less than .2, which were subsequently entered into the final multivariate models. Results of the multivariate models are presented as adjusted odds ratios (AOR) with accompanying 95% confidence intervals (CI). A p-value of <0.05 was considered statistically significant. Analyses were conducted using IBM SPSS Statistics for Windows, Version 22 (Armonk, NY, USA).
Results
Summary data for the 1921 granted and delayed IAC-Echocardiography applications during the observation period are presented in Table 3. Most (71.0%) echocardiography laboratories had one site and a median annual volume 1830 ATTE per applicant (interquartile range, 850-3992). Of the 1921, 280 also applied for TEE and 647 for SE, with 204 seeking both TEE and SE accreditation; median annual volume of TEE was 386 (interquartile range, 138-670) and median annual volume of SE was 559 (interquartile range, 220-1135). The majority (71.6%) were applications for reaccreditation. Only 13.9% used the services of a consultant to prepare their accreditation application. Nearly one-third of applicants were hospital-based.
Characteristics of Facilities With Initial Granted Compared to Delayed Accreditation for Adult Transthoracic Echocardiography.
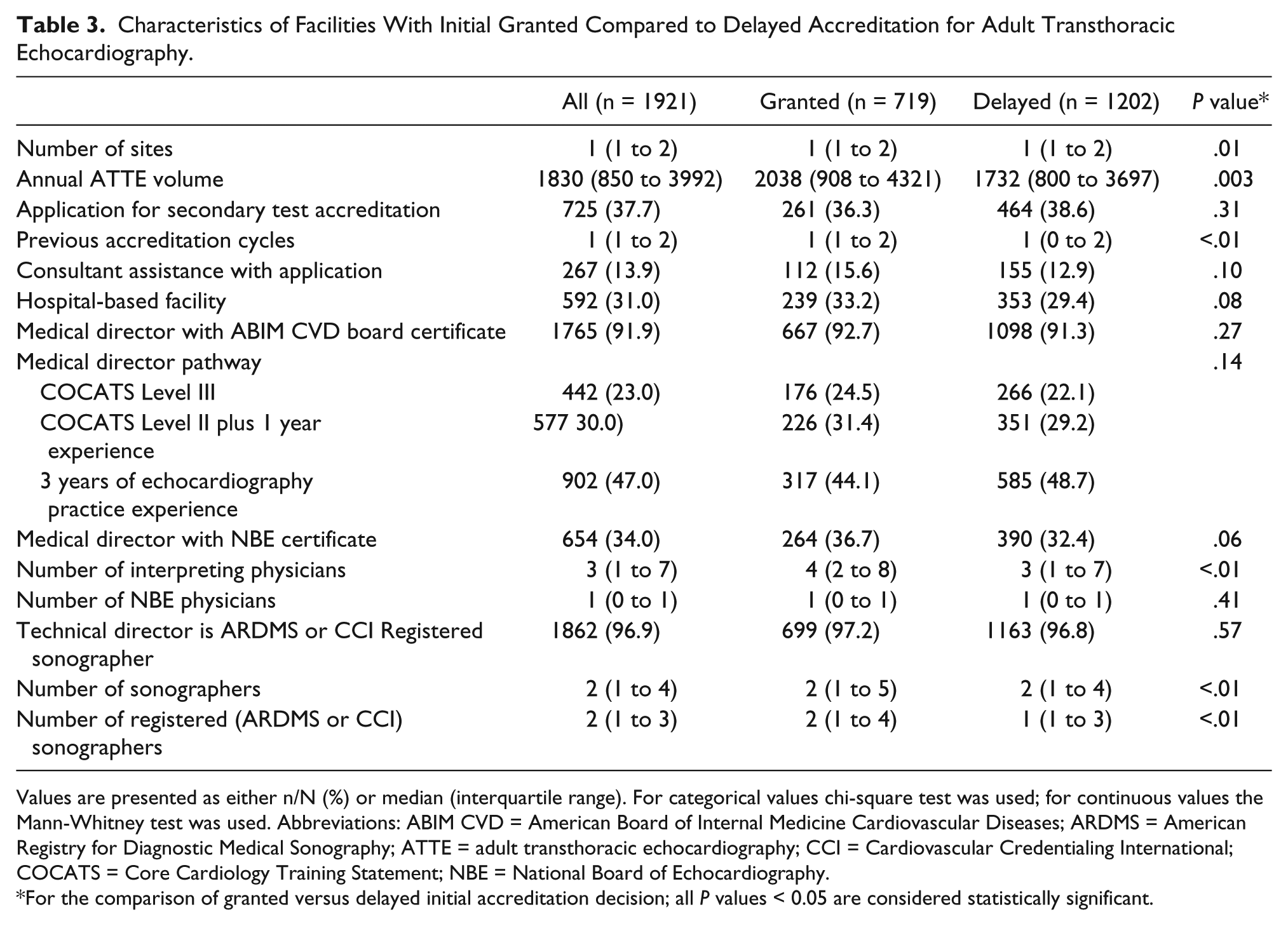
Values are presented as either n/N (%) or median (interquartile range). For categorical values chi-square test was used; for continuous values the Mann-Whitney test was used. Abbreviations: ABIM CVD = American Board of Internal Medicine Cardiovascular Diseases; ARDMS = American Registry for Diagnostic Medical Sonography; ATTE = adult transthoracic echocardiography; CCI = Cardiovascular Credentialing International; COCATS = Core Cardiology Training Statement; NBE = National Board of Echocardiography.
For the comparison of granted versus delayed initial accreditation decision; all P values < 0.05 are considered statistically significant.
Staff Credentials
Most (91.9%) echocardiography laboratory medical directors were board certified in cardiovascular diseases (CVD); 5.5% were certified in internal medicine but not CVD, 0.8% in another American Board of Medical Specialties (ABMS) specialty, and 1.8% had no ABMS certificate. The most commonly documented qualifying pathway among medical directors was experiential training (47.0%) with smaller numbers reporting Core Cardiology Training Statement (COCATS) Level III (23.0%) or COCATS Level II plus 1 year of experience (30.0%). Only 34.1% of medical directors were NBE testamurs and only 26.9% of interpreting physicians were NBE testamurs. Compared to nonhospital echocardiography laboratories, medical directors of hospital-based echocardiography laboratories were more likely to be COCATS Level III trained (30.8% versus 19.8%, P < .01) and be NBE testamurs (45.6% versus 28.9%, P < .01).
Over 96% of technical directors of echocardiography laboratories were registered sonographers and 79.5% of staff sonographers were registered with either ARDMS or CCI. A physician served as the technical director in 59 (3.6%) echocardiography laboratories; 14 of these physicians were NBE testamurs and 5 were registered with either ARDMS or CCI. Sonographers in hospital-based echocardiography laboratories were also more likely to be registered than in non-hospital-based echocardiography laboratories (82.2% versus 75.9%, P < .01).
Granted Versus Delayed ATTE Accreditation Decisions
During the study period, 719 (37.4%) applicants received “granted” accreditation decisions while the remaining 1202 received a “delay” decision (Figure 1). The majority of applicants’ accreditation was delayed due to a deficiency in both ATTE and organizational deficiencies. Deficiency in the staff domain was reported the most frequently (51%) although followed closely by the remaining four domains.
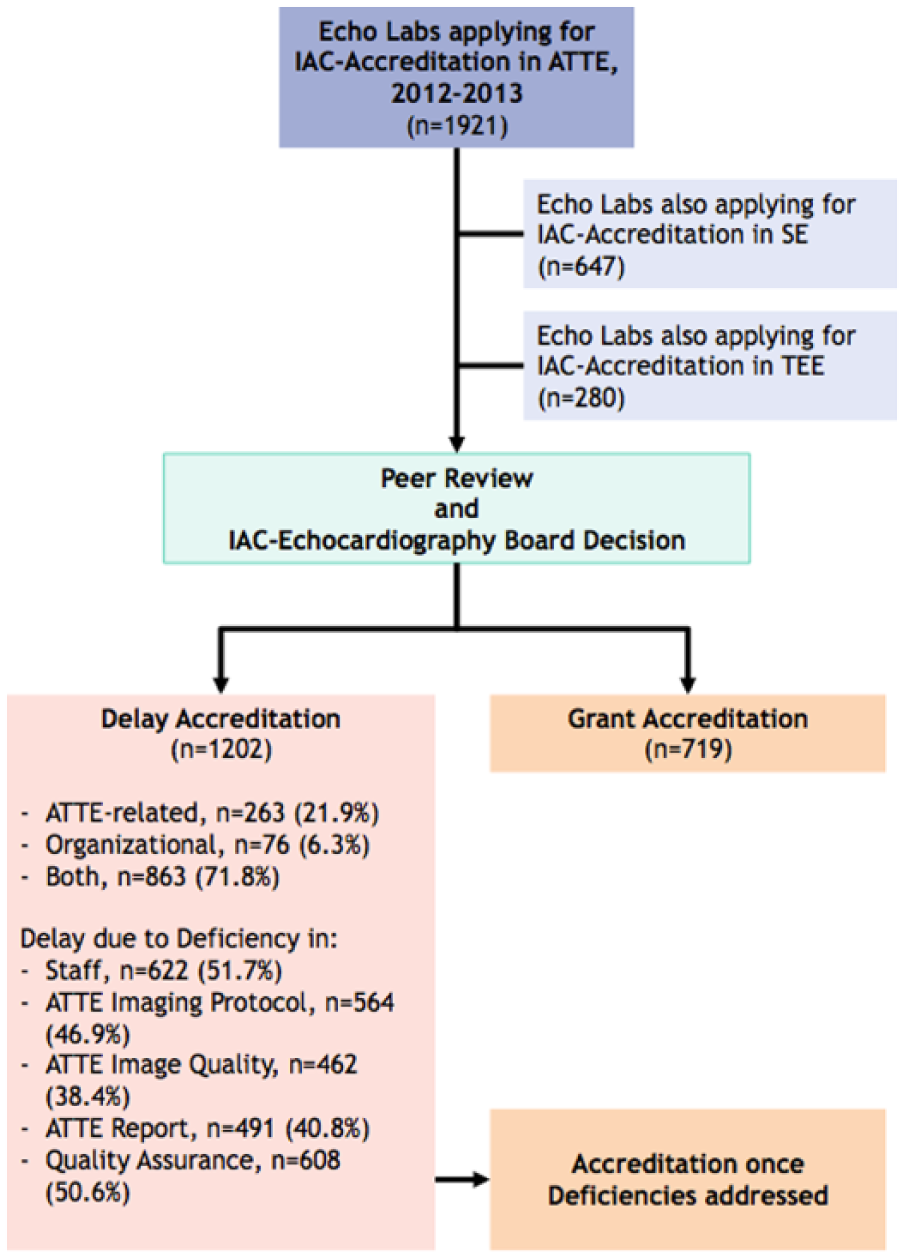
Schematic of the Intersocietal Accreditation Commission (IAC) -Echocardiography application process through Peer-Review and Accreditation for the applicants evaluated.
Upon univariate analysis, there was a trend toward granted versus delayed ATTE accreditation among echocardiography laboratories where the medical director was an NBE testamur (P = .06). Registered sonographers were significantly associated with granted versus delayed accreditation decisions (P < .01). Number of sites, annual volume, previous accreditation, number of physicians, number of sonographers, and number of registered sonographers were all associated with granted accreditation decision in univariate analyses (Table 3).
In the multivariate analysis, NBE testamur status of the echocardiography laboratory medical director did not reach statistical significance for accreditation application success (AOR 1.15 [0.93 to 1.42]) but number of registered sonographers per applicant did (AOR 1.13 [1.04 to 1.23]) (Table 4).
Characteristics of Applicants and the Impact on Adult Transthoracic Echocardiography Accreditation Decision After Multivariable Adjustment.
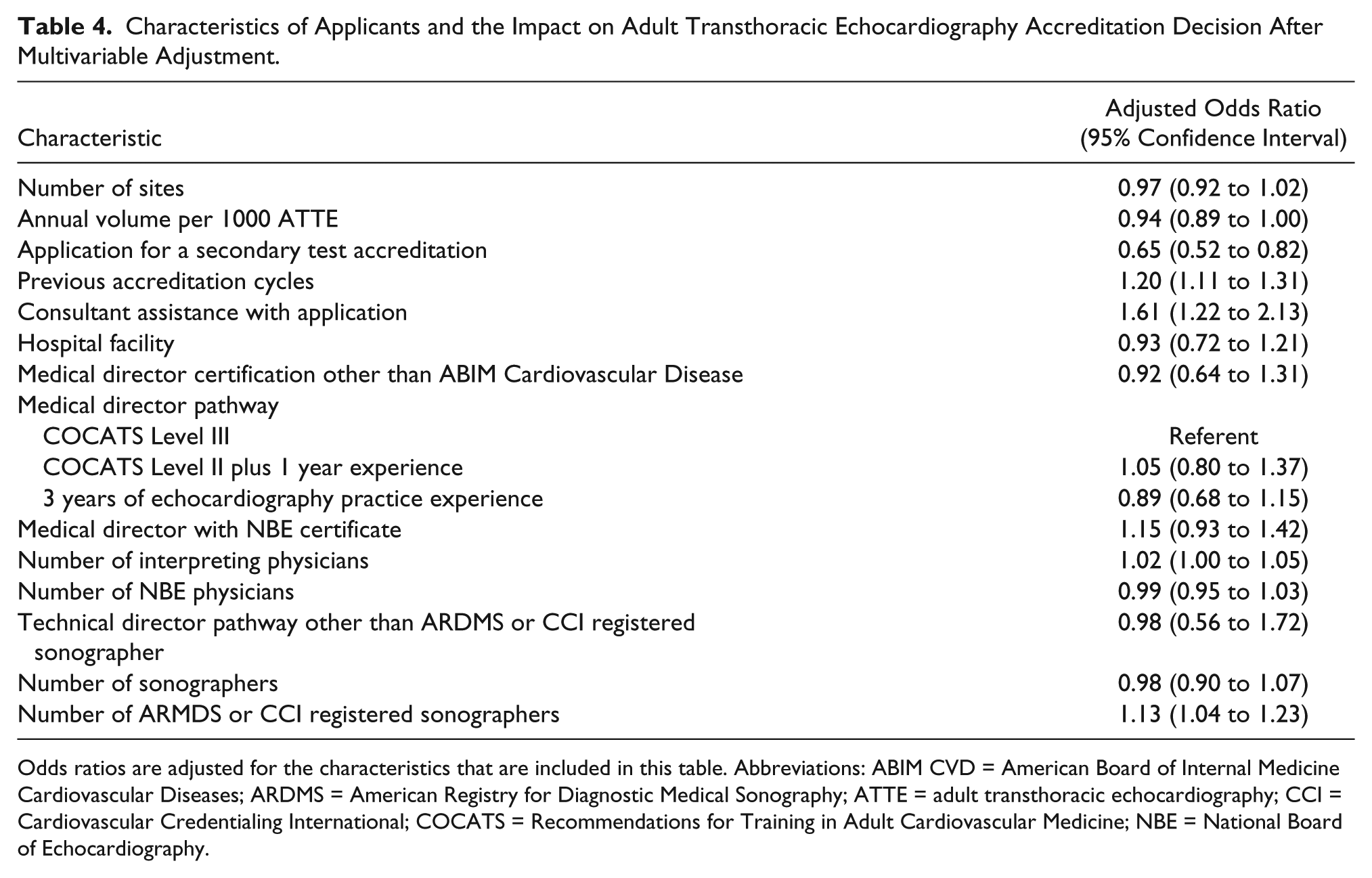
Odds ratios are adjusted for the characteristics that are included in this table. Abbreviations: ABIM CVD = American Board of Internal Medicine Cardiovascular Diseases; ARDMS = American Registry for Diagnostic Medical Sonography; ATTE = adult transthoracic echocardiography; CCI = Cardiovascular Credentialing International; COCATS = Recommendations for Training in Adult Cardiovascular Medicine; NBE = National Board of Echocardiography.
Individual Domain Deficiencies for ATTE Accreditation
Table 4 also reports the associations between applicant characteristics and deficiencies in each of the five peer-reviewed domains of accreditation for ATTE. Multiple markers of echocardiography laboratory size were associated with deficiencies in several domains: Echocardiography laboratories with more sites tended to have more deficiencies in ATTE reporting (AOR 1.07 [1.01 to 1.14]). Increasing annual ATTE volume was associated with deficiency in the staff credentials (AOR 1.07 [1.01 to 1.12]), ATTE report (AOR 1.08 [1.02 to 1.15]), and quality assurance (AOR 1.09 [1.03 to 1.16]) domains. Similar to the overall accreditation decision, applicants simultaneously seeking accreditation in TEE or SE were more likely to have deficiencies in ATTE image quality (AOR 1.31 [1.02 to 1.67]) and quality assurance (AOR 2.22 [1.77 to 2.80]) domains.
Familiarity with the IAC accreditation process was an important factor in several peer-reviewed areas. Each successive previous accreditation was associated with fewer deficiencies in four out of the five domains, as was assistance from a consultant in preparing the application.
Medical directors who were NBE testamurs were associated with fewer deficiencies in the image quality (AOR 0.61 [0.48 to 0.79]) and report (AOR 0.72 [0.56 to 0.92]) domains.
Applicants whose technical director was a physician rather than a sonographer were more likely to have deficiencies in the image quality (AOR 1.84 [1.06 to 3.21]) domain. Number of sonographers in an echocardiography laboratory increased the odds of deficiency in the staff domain (AOR 1.12 [1.02 to 1.21]), that is, documentation of adequate CME/CE and verification of credentials. Number of registered sonographers, however, reduced the odds of deficiency in the staff credentials domain (AOR 0.84 [0.78 to 0.92]) and also the report (AOR 0.88 [0.81 to 0.96]) and quality assurance (AOR 0.91 [0.84 to 0.98]) domains, with a trend toward fewer deficiencies in the image quality domain (AOR 0.91 [0.84 to 1.00]) (Table 5).
Characteristics Associated With Deficiency for Overall Accreditation Decision and the Five Domains of Accreditation for Adult Transthoracic Echocardiogram.
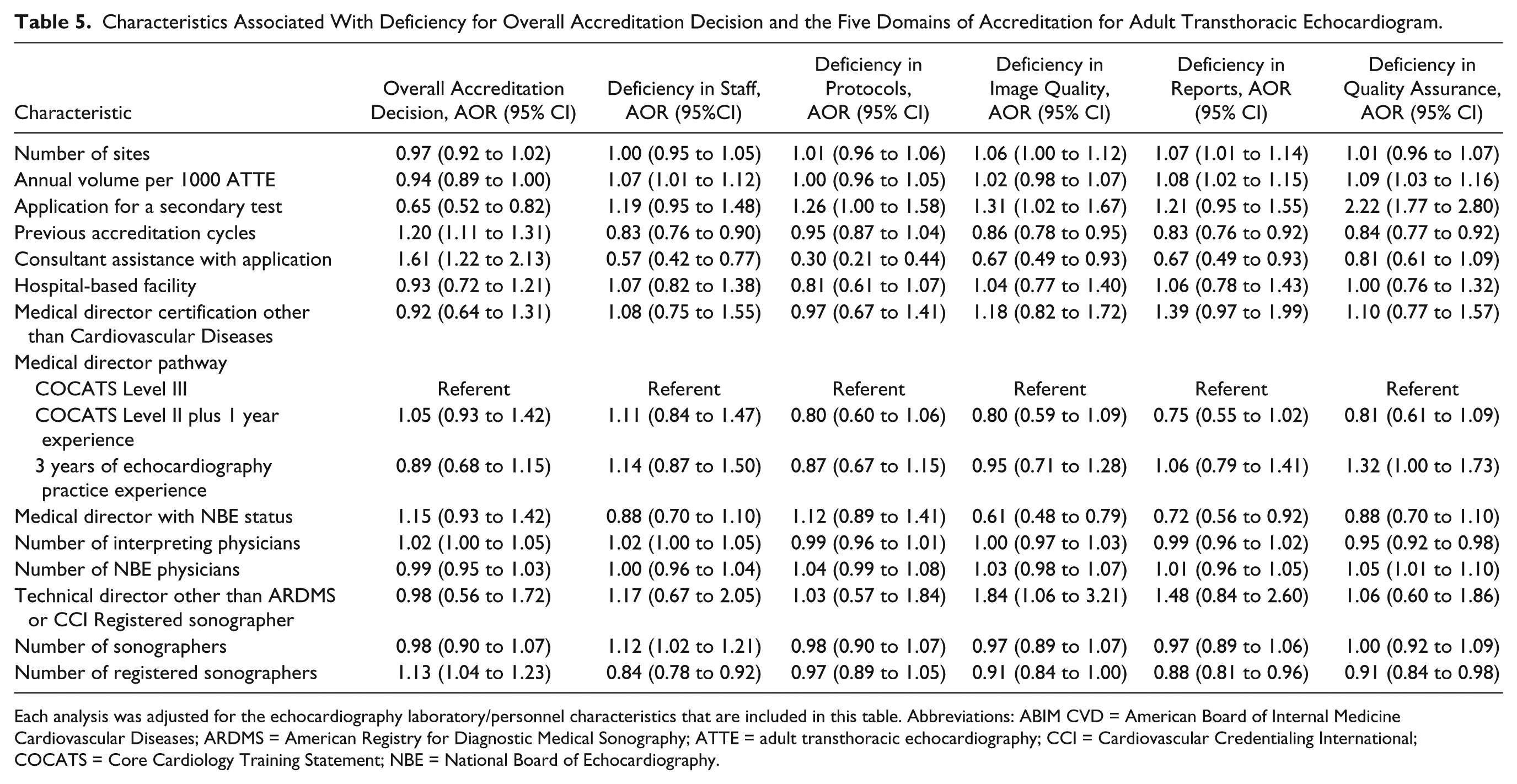
Each analysis was adjusted for the echocardiography laboratory/personnel characteristics that are included in this table. Abbreviations: ABIM CVD = American Board of Internal Medicine Cardiovascular Diseases; ARDMS = American Registry for Diagnostic Medical Sonography; ATTE = adult transthoracic echocardiography; CCI = Cardiovascular Credentialing International; COCATS = Core Cardiology Training Statement; NBE = National Board of Echocardiography.
TEE and SE
Of the 280 applications for TEE accreditation, 90 (32.1%) met peer-reviewed standards for accreditation. Of the 647 applications for SE accreditation, 275 (42.5%) met peer-reviewed standards for accreditation. After multivariate adjustment, NBE testamur status of the medical director was not significantly associated with TEE (AOR 1.18 [0.96-1.08]) or SE accreditation recommendation (AOR 1.24 [0.88-1.75]). Similarly, number of registered sonographers in the echocardiography laboratory did not reach statistical significance for association with TEE (AOR 1.15 [0.99 to 1.34]) or SE (AOR 1.10 [0.97 to 1.24]) accreditation recommendation. No other covariables significantly impacted TEE or SE peer-review findings (Supplemental Tables 1 and 2).
Discussion
Analysis of a large, voluntary sample of echocardiography laboratories seeking IAC-Echocardiography accreditation allows us to make the following conclusions: First, although a minority of physicians are NBE testamurs, the majority of sonographers performing echocardiography have registered credentials. Second, NBE testamur status of medical directors was not associated with positive overall accreditation decision after adjusting for other laboratory factors, but there was a positive association between number of registered sonographers in an echocardiography laboratory and initial IAC accreditation decision. We believe that these data suggest that the credentialing and registration of sonographers has a greater influence of adult echocardiography accreditation than the credentials of echocardiography physicians. Although these findings are not altogether surprising, we believe this is an important validation of training standards for front-line imaging professionals.
We speculate that this may reflect the greater responsibility of sonographers and technical directors in image quality and acquisition protocols. In support of this conclusion, we found that the group of echocardiography laboratories most likely to have deficiencies with image quality were those where physicians serve as technical directors. These were echocardiography laboratories with no sonographers at all. It is possible that physician-sonographers may perform limited or disease-driven exams rather than comprehensive, protocol-driven exams, which could explain the low peer-review scores in imaging protocols and quality. A recent analysis of echocardiographic case studies submitted to IAC-Echocardiography by credentialed and noncredentialed sonographers provided additional evidence that credentialing of sonographers ensures competency in protocol-driven imaging. 9
Our data extend the findings of Nagueh et al in their study of predictors of delayed accreditation, which also found that credentialed sonographers were associated with more positive accreditation decisions. 10 Our analysis specifically demonstrated that in addition to reducing deficiency in the staff domain of laboratory accreditation, credentialed sonographers are also associated with fewer delays due to report and quality assurance.
One goal of the accreditation process is to reduce variability in imaging services provided,5,8 and it is desirable that laboratories engaging in the accreditation process may improve their processes and quality independent from individual staff’s credentials as seen in our analysis.
During the study period more nonhospital echocardiography laboratories applied for accreditation than hospital-based labs, which may reflect payer coverage decisions. 11 Physicians in hospital-based echocardiography laboratories documented more advanced training (COCATS Level III) and NBE testamur status more often than non-hospital-based echocardiography laboratories; there was a parallel trend toward more frequent ARDMS/CCI registration among non-hospital-based sonographers. Whether these structural differences in hospital-based and non-hospital-based imaging laboratories are associated with differences in quality outcomes is worthy of further investigations.
Limitations
Detailed data on which physicians are “certified” by the NBE, a program that involves training and caseload verification, were not available. Certification of personnel and accreditation of laboratories are structural measures of quality, distinct from process measures such as appropriate use, or outcomes measures such as improved patient health or reduced cost.
The IAC-Echocardiography accreditation process has previously been critiqued because it is based on a single “snapshot” of cases and policy documentation provided by the applicant that may not fully reflect a laboratory’s day-to-day product. 4 The same limitation is true of our analysis.
As with all observational research, only variables which are included in the analysis are those adjusted for and reflected in the final odds ratios. We cannot discount other confounders that may be influencing the results, including duration of experience of physicians and sonographers and availability of advanced technology in the echocardiography laboratory.
The univariate trend toward an association with accreditation decisions in labs where the medical director was an NBE testamur may indicate that the sample was underpowered to detect a difference. This is especially relevant given the low frequency of NBE testamur status, but given the size of the sample, we would not expect a large difference to go undetected due to a type II, or “false negative,” error.
Conclusions
Among echocardiography laboratories seeking IAC-Echocardiography accreditation, a minority of echo physicians are testamurs of the NBE while the majority of sonographers are registered with a credentialing body. Registered sonographers, but not NBE testamur physicians, were positively associated with accreditation decisions; this appeared particularly important for the small number of echocardiography laboratories with physician-sonographers. The overall interaction of individual certification and laboratory accreditation suggests a complementary role for both.
Footnotes
Acknowledgements
The authors acknowledge Mary Beth Farrell, CNMT, for assistance with data management, and Warren J. Manning, MD, for review of the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Parker is a consultant for the Intersocietal Accreditation Commission. The remaining authors have no relevant disclosures.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an investigator-initiated research grant to the authors from the Intersocietal Accreditation Commission, Ellicott City, MD. The content is solely the responsibility of the authors and does not necessarily represent the official views of the IAC or the IAC Research Committee.