
Abstract
Background: Fetal ultrasound screening for congenital heart disease has high detection rates in efficacy studies but not in practice. We investigated sonographers’ perspectives on barriers to screening and their association with intermediate measures of cardiac imaging. Methods: Barriers to fetal heart screening were identified in focus groups with obstetric sonographers. A web-based survey measured reported barriers and sonographers’ ability to interpret fetal heart screening images. Generalized linear random effect models assessed associations between barriers and image interpretation. Results: Four themes were identified: intrinsic barriers (self-efficacy), external barriers (time), informational needs, and provider and patient expectations. Among 224 sonographers surveyed, an average of 77.6% of fetal heart images were interpreted correctly. Perceptions about self-efficacy (P = .03) and ease of performing imaging (P = .01) were associated with accuracy of image interpretation. Conclusions: Several sonographer-identified barriers associated with image interpretation may be novel targets for improving prenatal detection of congenital heart disease.
Prenatal detection of congenital heart disease (CHD) optimizes postnatal cardiac care.1–7 National guidelines recommend that prenatal screening for heart defects occur during the second-trimester fetal anomaly scan. 8 Current obstetric literature advocates imaging both the four-chamber view and the outflow tract for adequate screening of the fetal heart.9–12 In efficacy studies, the rate of detection of CHD with the four-chamber view alone is 55% to 65% and increases to ~85% with the addition of outflow tract imaging.12–14 Despite the fact that most women in the United States and other developed countries have an ultrasound during pregnancy,3,15,16 only 30% to 50% of CHD is detected during routine clinical care, and many defects requiring neonatal intervention are missed.7,15,17–20 Prenatal detection of CHD can be increased by improving the sensitivity of screening ultrasound in clinical practice.
The accuracy of prenatal CHD detection relies to a great degree on the sonographer who obtains the images. Sonographers are on the front line of the screening process. They must recognize whether the images that they obtain of the fetal heart adequately capture the important structures, and in some instances sonographers are responsible for differentiating between “normal” and “abnormal” images to demonstrate their findings for the interpreting physician. Previous work linking increased sonographer experience to improved rates of CHD detection underscores the importance of sonographers in this screening process.21,22 However, little has been done to directly engage sonographers in determining how prenatal detection of CHD might be improved.
Ultrasound technology and its use for cardiac screening have evolved significantly in the past two decades. 23 These technical gains are not useful without similar evolution in sonographer training and experience with this technology. Experience and training also likely interact with other factors that influence sonographers’ abilities to perform cardiac imaging. Research on sonographers’ understanding, acceptance, and performance of less familiar skills, such as cardiac screening, is scarce and could provide important strategies for improving the quality of prenatal screening ultrasounds in practice.24,25
This mixed methods study sought to determine sonographer self-reported barriers, facilitators, and behaviors with regard to the performance of cardiac screening, through qualitative methods. Factors identified in the qualitative study were then examined for associations with an objective assessment of sonographer accuracy in interpreting fetal heart images.
Methods
Design
We used a two-phase mixed methods approach employing focus groups to inform the creation of a quantitative regional survey. First, we conducted focus groups of sonographers to determine salient facilitators and barriers surrounding fetal cardiac screening. Focus groups were chosen as a data collection mode for two reasons: (1) they have been shown to be an efficient and effective means of collecting information about a topic in the target populations’ own words, and (2) they allow research participants to generate their own ideas and responses rather than choose from those preconceived by the investigator. 26 The focus group discussions identified sonographers’ ideas and thoughts regarding their attitude toward scanning fetal hearts, what they found made scanning fetal hearts easier or harder, their preparation for imaging, and suggestions for improving the screening process. Sonographer responses were used to develop an explanatory conceptual model for sonographer behaviors surrounding fetal cardiac screening that could be tested with quantitative investigation. 27 Our conceptual model incorporated cognitive and behavioral concepts from the technology acceptance model 28 and the “unified theory of acceptance and use of technology” model, 29 which explain the acceptance and use of new technology. Behavioral intention, a person’s perception of his or her own likelihood of engaging in a behavior—in this case, performing cardiac imaging—is central to both models and is one of the best predictors of behavior. 30
We then performed a quantitative cross-sectional regional survey to test the explanatory model of behaviors surrounding screening (Figure 1). The first section of the survey measured behavioral intentions and concepts that influence cardiac screening, as identified by the focus groups through validated measures. It also included questions regarding self-reported ability to obtain cardiac screening images and the estimated time to obtain such images. The second part of the survey presented 20 video clips of fetal heart screening views (10 four-chamber and 10 outflow tract views). Two fetal cardiologists, a fetal cardiac sonographer, and a maternal fetal medicine specialist all independently reviewed the images. Only images with 100% interrater agreement were used. Sonographers were asked to assess (1) whether the video clip image was adequate for screening the fetal heart and (2), when provided adequate images, whether the image was normal or abnormal. Volunteers from the previous focus groups critiqued the survey for content and clarity. The revised survey was pretested by 15 focus group participants.
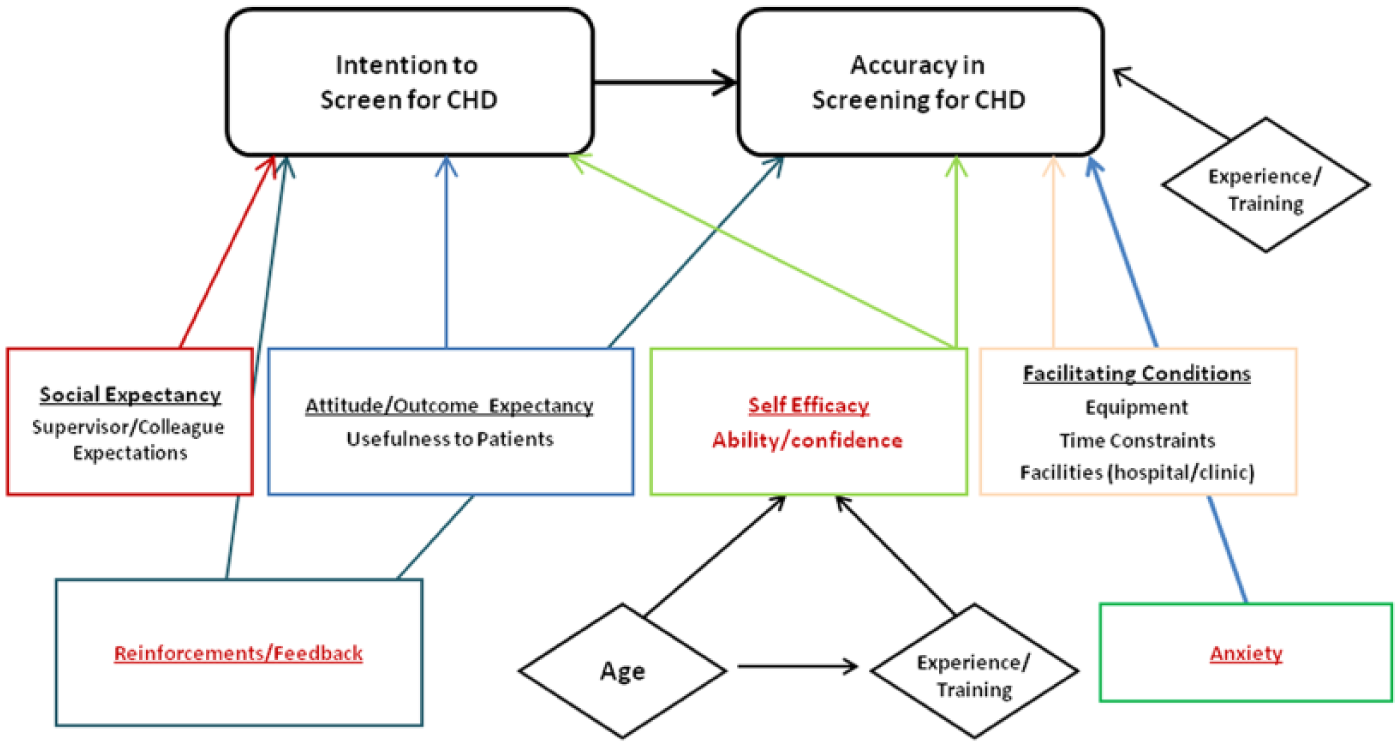
Final explanatory model of factors influencing screening behaviors and accuracy in image interpretation. CHD, congenital heart disease.
Participants and Procedures
Focus group participants were recruited locally from an annual meeting of Utah diagnostic sonographers via local flyers and email lists. A regional recruitment effort was undertaken through mailings to sonographers registered as specializing in obstetric ultrasound with the American Registry of Diagnostic Medical Sonography in Utah and Idaho. The target population included sonographers who practiced in hospital and clinic settings (both high-risk and general obstetrics) and who practiced in urban or rural settings. Focus group size was limited to 12 participants. 31 Written informed consent was obtained from all participants, who were given a $50 gift card as a token of appreciation for their time.
Evidence-based survey implementation procedures were employed. 32 First, invitations (with a $10 preincentive) were mailed to all sonographers registered with the American Registry for Diagnostic Medical Sonography in Idaho, Wyoming, and Utah who had designated obstetric ultrasound as their specialty. The initial recruitment letter was followed by email and additional postal mail invitations.
The study was approved by the University of Utah’s Institutional Review Board.
Data Analysis
Focus group discussions were recorded and transcribed. Data were analyzed through the framework of constant comparison. 33 Themes were identified by consensus and coded by two investigators using TAMS Analyzer software (version 4.14b1h). The primary outcome of the survey was accuracy of image interpretation. This was analyzed dichotomously as “correct” or “incorrect.” Reponses for all behavioral and cognitive concepts were measured with multi-item construct scales where each item (subscale) was measured with a 5-point Likert response, with 5 indicating the strongest agreement with a statement. Raw scores were summarized for each construct subscale and scale (average of subscales). Participant demographics were summarized. Factors associated with cardiac imaging behaviors and abilities were analyzed through linear regression models. The association of measured cognitive and behavioral concepts and the accuracy of image interpretation was examined through generalized linear random effects models. Exploratory subgroup analysis was also performed with groups based on the type of image (four chamber or outflow) and according to whether the image required interpretation of adequacy or abnormality. All quantitative analyses were conducted with SAS 9.4 (SAS Institute, Cary, NC).
Results
Focus Groups
Demographics
Two focus groups were conducted in Salt Lake City, Utah, and one in Boise, Idaho, between May 2010 and January 2011, with 11, 6, and 12 participants, respectively. Demographic information is presented in Table 1. The mean age of participants was 42 years (SD = 10.6, range = 28–56), and almost all were female. Of 29 participants, 24 answered the demographic survey questions; 12 (50%) practiced in clinic-based (vs. hospital) settings and 4 (17%) in rural settings.
Focus Group Participant Demographics. a
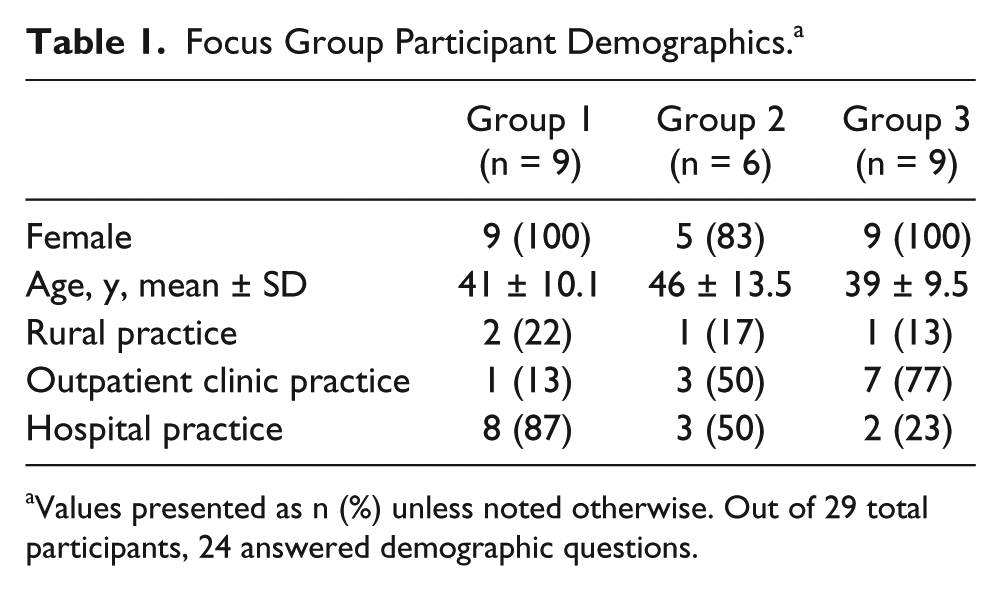
Values presented as n (%) unless noted otherwise. Out of 29 total participants, 24 answered demographic questions.
Analysis
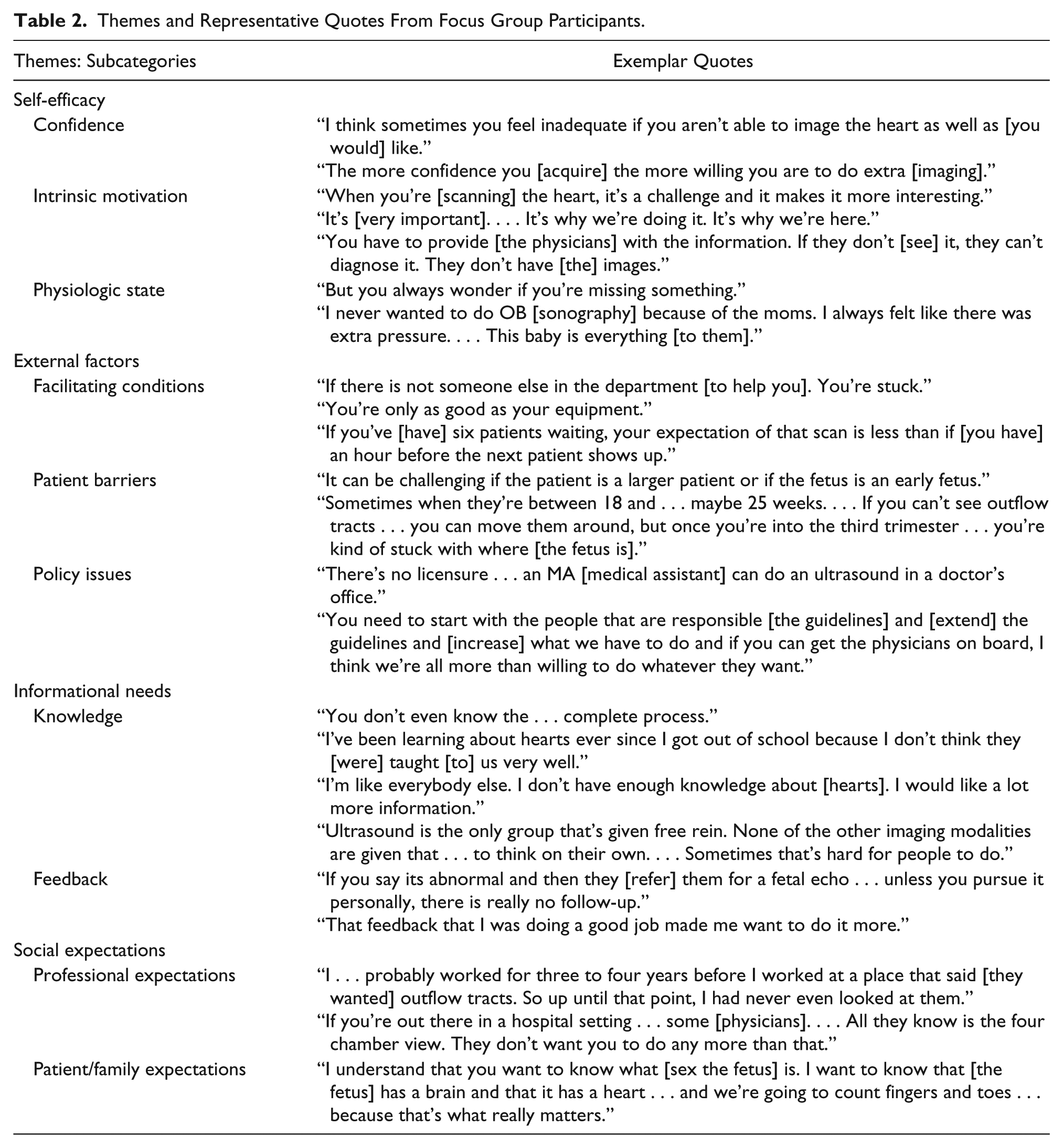
Four dominant themes emerged regarding factors influencing the performance of cardiac images during a second-trimester anomaly scan for prenatal screening for congenital heart defects (Table 2): intrinsic barriers, extrinsic barriers to performing imaging, informational needs for imaging, and external expectations regarding the performance of this imaging.
Themes and Representative Quotes From Focus Group Participants.
Intrinsic Barriers
Intrinsic barriers included the concepts of self-efficacy, outcome expectancy (perceived usefulness), and attitudes about screening. Self-efficacy—reflected by sonographers’ confidence in their ability to perform obstetric cardiac imaging—emerged as a key theme and was intimately related to intrinsic motivation to perform this imaging. Participants expressed varying levels of self-efficacy about their ability to perform screening images and about knowledge of the fetal heart. They believed strongly that confidence in their abilities had an impact on their performance, specifically that higher self-efficacy made a positive impact on both their skills and attitudes about scanning the fetal heart.
Some participants cited that they were motivated by the importance of their role in providing interpreting physicians with adequate images and ultimately helping their patients get appropriate care (outcome expectancy). However, participants reported that the cardiac portion of the anomaly scan could be anxiety provoking because of the fear of “missing something.” Several expressed that obstetric ultrasound was a more anxious setting than other imaging modalities because of the heightened emotions of expectant parents.
Extrinsic Barriers
Extrinsic barriers to performing adequate screening cardiac images fell into three main categories: facilitating conditions, patient factors, and policy issues. Participants in all three focus group discussions identified patient appointment time as a key barrier. The amount of time allotted for a fetal anomaly scan varied highly across practices. Most participants expressed that an adequate scan required 45 to 60 minutes, but some were allotted as little as 20 minutes. A few participants reported that they were also limited by suboptimal equipment.
There was strong agreement among sonographers that several key patient-related factors could influence their imaging. While participants specifically noted that patient body habitus and fetal position were important to obtaining adequate cardiac images, the most frequently mentioned barrier was the gestational age of the fetus. Sonographers found it particularly frustrating when physicians referred patients “too early” and this resulted in poor images. Most were comfortable with performing scans after 18 weeks, although several expressed that they would be more confident with their cardiac images if scans were repeated after 22 weeks of gestation. A few mentioned the scheduling systems in place in their offices to prevent expectant mothers from being scheduled too early.
Policy-level issues that affected the screening process were mentioned in two of the three focus groups. Participants raised concerns surrounding a lack of standardization or licensure for those performing fetal anomaly scans. A few sonographers also mentioned that the consensus guidelines at the time discouraged their performance of outflow tract imaging. 34 In fact, a few sonographers mentioned situations where they had been specifically asked not to do outflow tract or additional cardiac imaging.
Informational Needs
One area of strong agreement among all three focus groups was that their education and knowledge about the fetal heart and fetal heart imaging techniques were inadequate. Training regarding the anatomy and imaging of fetal hearts was highly variable, but participants universally agreed that their training did not prepare them to image the heart, especially the outflow tracts. Sonographers who had higher levels of self-efficacy about imaging the heart had independently sought out additional training/education after their schooling. However, support and funding for such activities by employers and institutions varied. Participants identified a need for a greater understanding of their role in the prenatal screening process. Most reported a lack of awareness of the current rate of prenatal detection of CHD, and many believed that this knowledge would motivate sonographers to take actions to improve their imaging.
Participants also expressed a desire to receive more feedback about the adequacy of their images and the diagnosis of referred patients. Receiving positive feedback was identified as a motivational factor, but they also expressed a desire for constructive criticism that would help them improve their imaging skills. Practice settings were identified as a factor that often influenced the amount and timeliness of feedback. For example, sonographers that scanned in a hospital that housed perinatologists or fetal cardiologists facilitated obtaining information on the subsequent imaging of referred patients.
External Expectations
External social expectations fell into two major categories: professional expectations and patient/family expectations. Some sonographers expressed pride in being held to high imaging standards by their physicians and coworkers. Others perceived that their imaging was negatively influenced by low external expectations. Regardless of the direction of their colleagues’ perceived expectations, there was strong agreement that their supervising physicians’ expectations affected their images and their imaging abilities.
Another prevalent belief identified by focus group participants was that families and patients’ expectations were often incongruent with what the sonographers perceived as the purpose of the imaging test. They expressed concern that many families believe that the primary purpose of the fetal anomaly scan is to determine the sex of the child. Sonographers felt that families’ desires to know the sex of the fetus as soon as possible influenced referrals for the anomaly scan too early to adequately image the fetal heart. Some participants highlighted the importance of educating families about the purpose of the second-trimester scan and the importance that scans be performed by registered sonographers at accredited facilities.
Study Model and Survey
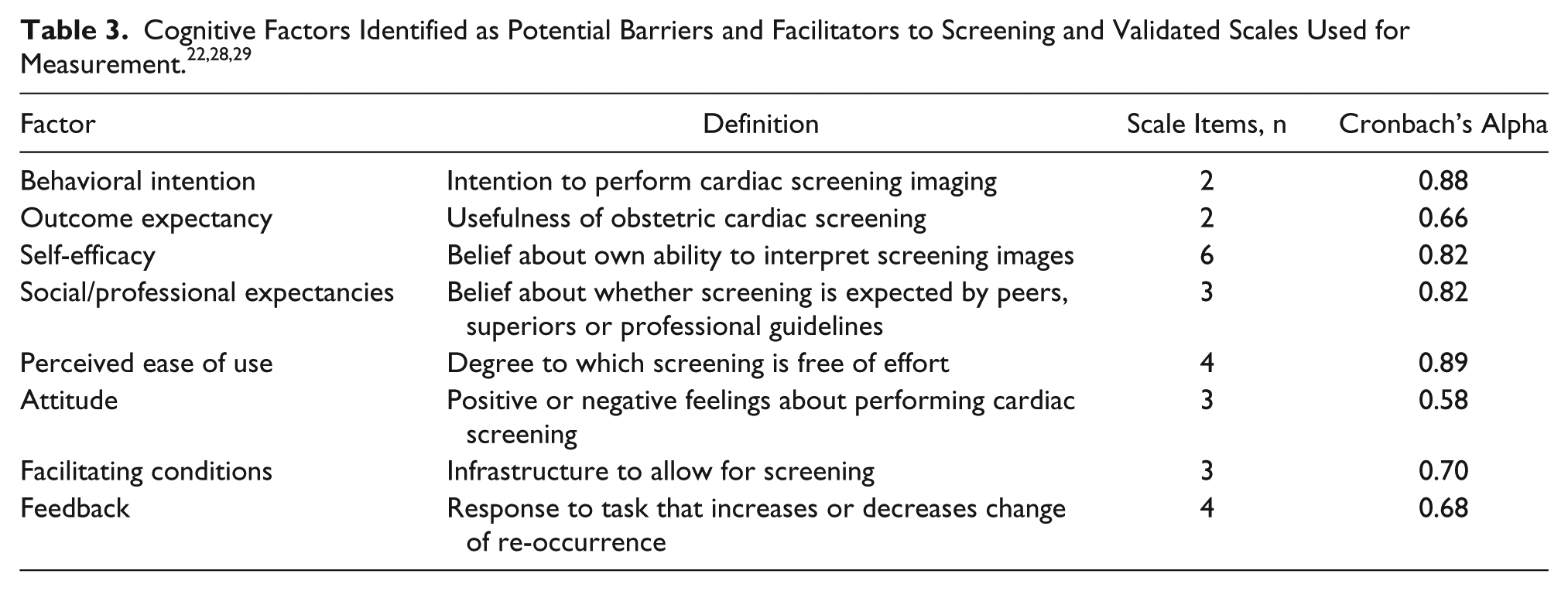
Based on focus group input, a study model was finalized that incorporated different concepts from several behavioral theories (Figure 1), including the theory of planned behavior and social cognitive theory in addition to those cited previously.35,36 Importantly, the concept of feedback was incorporated into the model, and sex was removed as a predictor of intention and ability. Survey questions were selected to reflect the behavioral and cognitive concepts from this model (Table 3).
Survey pretesting revealed excellent test-retest reliability, with 100% agreement in responses. The survey was attempted by 274 of 538 sonographers who received invitations (52% response rate) and completed by 224 participants.
Overall, behavioral intention to screen for CHD was high (87% “almost always”). The main factors associated with increased behavioral intention included facilitating conditions, higher professional expectations, outcome expectancy (higher perceived usefulness), higher self-efficacy, and positive attitude (Table 4). Self-assessment of ability was also high, with 76% of participants reporting that they were able to obtain both four-chamber and outflow views at least “most of the time.” Self-reported ability to obtain outflow views of the heart was lower than that for four-chamber views (16% able to obtain outflow views “all the time” vs. 42% for four-chamber views). Self-reported ability to obtain both four-chamber and outflow tract views was associated with self-efficacy, while attitude and experience were relevant to outflow tract views. Self-reported time to obtain images, an additional surrogate for ability, was associated with self-efficacy and perceived ease of use as well as professional expectations.
Stepwise Generalized Mixed Linear Regression Model: Factors Associated With Cardiac Imaging Behaviors and Abilities.
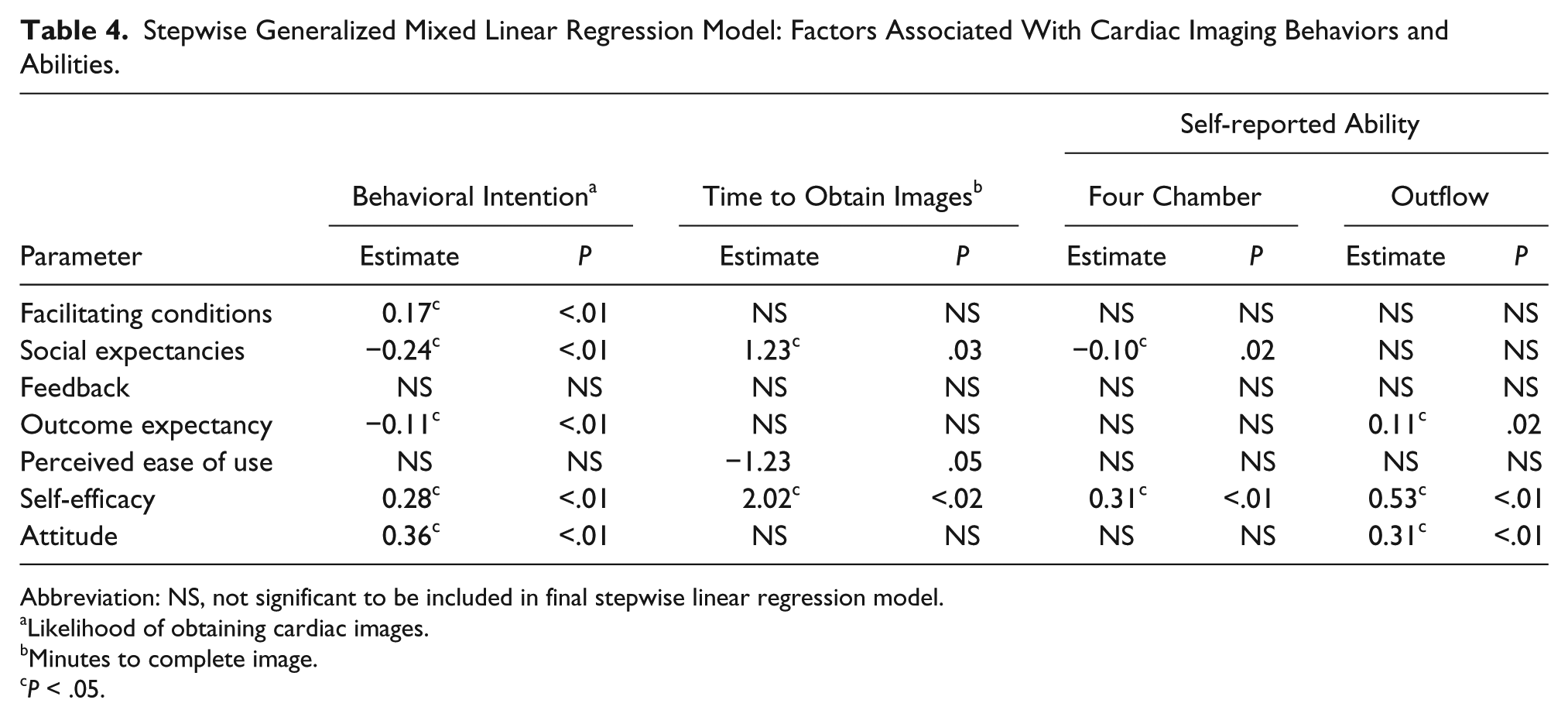
Abbreviation: NS, not significant to be included in final stepwise linear regression model.
Likelihood of obtaining cardiac images.
Minutes to complete image.
P < .05.
Sonographers performed well in interpreting the cardiac screening images presented on the survey, with a mean accuracy of 77.6% (Figure 2) for all images. Accuracy in image interpretation was associated with perceived ease of use and self-efficacy (Table 5). Accuracy in interpreting whether four-chamber views were adequate was associated with outcome expectancy (odds ratio [OR], 1.17; 95% confidence interval [95% CI], 1.03–1.33), while accuracy in interpreting adequacy of outflow images was associated with behavioral intention (OR, 1.22; 95% CI, 1.05–1.41). Correct interpretation of whether four-chamber images were normal or abnormal correlated with self-reported time to obtain images (OR, 0.96; 95% CI, 0.93–0.99) and years performing obstetric ultrasound (OR, 1.03; 95% CI, 1.01–1.05). Correctly interpreting whether outflow images were normal or abnormal was associated with perceived ease of use (OR, 1.52; 95% CI, 1.29–1.79). When separated by type of view, overall accuracy for four-chamber images (OR, 1.14; 95% CI, 1.03–1.26) and outflow images (OR, 1.23; 95% CI, 1.11–1.36) were associated with self-assessment of ability to obtain an outflow tract view.
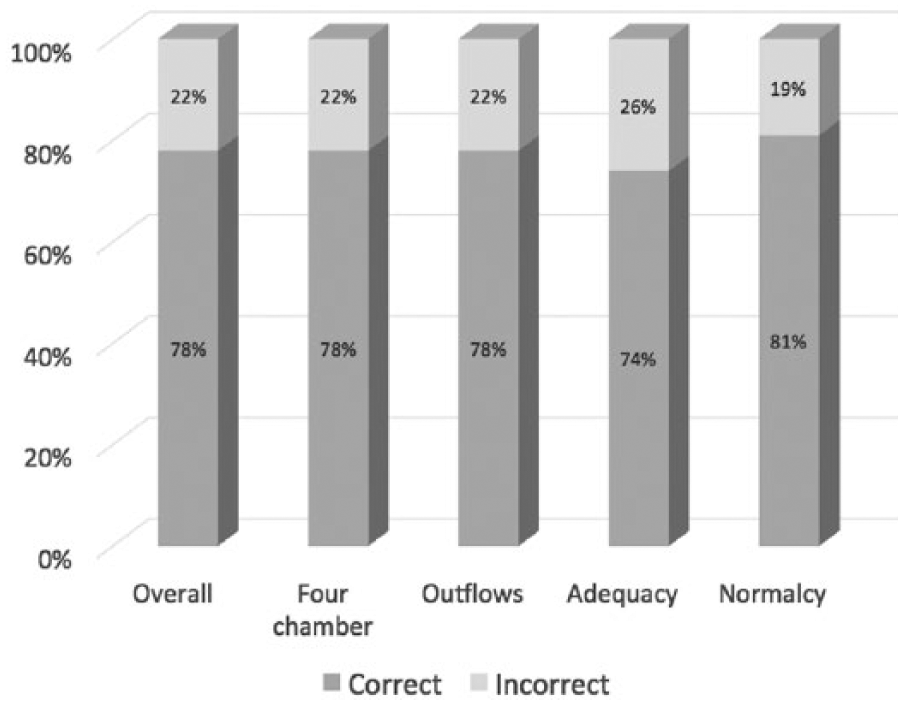
Accuracy of cardiac fetal screening image interpretation. Bars represent average percentage of images correctly interpreted.
Factors Associated With Accuracy of Fetal Cardiac Image Interpretation. a
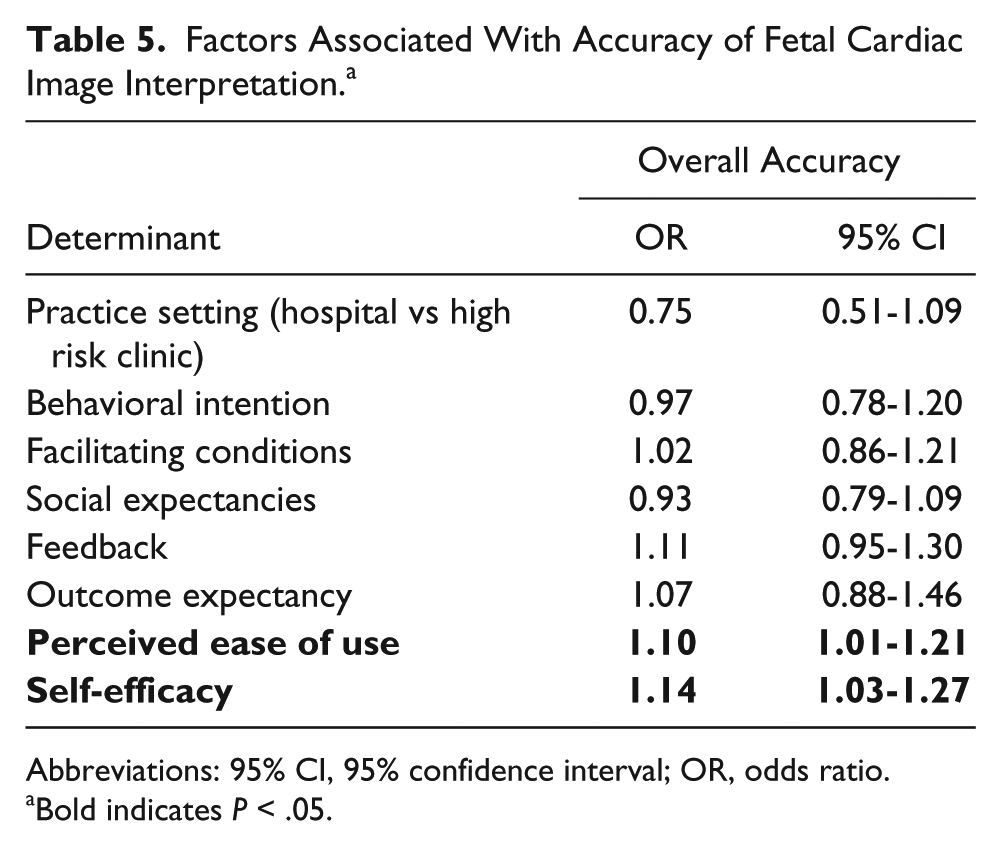
Abbreviations: 95% CI, 95% confidence interval; OR, odds ratio.
Bold indicates P < .05.
Discussion
To our knowledge, this is the first study that has directly engaged sonographers to strategize on improving prenatal detection of CHD. Sonographers identified informational needs as their most important barrier to screening the fetal heart. We found that cognitive factors affect sonographers’ intention to screen for CHD—self-efficacy, external expectations, and outcome expectancy. Furthermore, we found that behavioral intention, self-reported abilities, and outcome expectancy influenced sonographers’ abilities to interpret cardiac screening images. This information provides novel insights into multiple factors that may have an impact on fetal cardiac screening and may allow us to implement effective changes to improve CHD detection rates.
Sonographers are central to the cardiac screening process. Available data suggest that physicians infrequently rescan obstetric patients after sonographers,37,38 thereby relying on sonographers to provide them with the information they need to interpret studies. If sonographers are unable to recognize whether the four-chamber and outflow tract views are adequate for screening, heart defects can be missed in the prenatal period. Previous interventions to improve prenatal detection of heart defects in countries such as Great Britain, Sweden, and Canada have recognized their central role by providing didactic and hands-on training to sonographers. While these interventions have had regional success, they have not been widely disseminated.39–41 Engaging sonographers so that interventions aimed at improving their imaging quality are most useful and accessible to them has the potential to improve such interventions.
Sonographers identified lack of knowledge of the fetal heart and cardiac screening as a key barrier to screening, in line with previous studies.21,42,43 Sonographer training is highly variable and mostly unregulated in the United States. Teaching on cardiac imaging is almost nonexistent in obstetric sonographer training, even though it is one of the most difficult parts of the fetal ultrasound examination.44,45 Insufficient training likely has a direct impact on sonographers’ self-efficacy with regard to imaging the fetal heart. Our survey results show that self-efficacy was an important predictor of both intention to screen hearts and sonographer accuracy in interpreting images.
While a lack of training in the technical aspects of screening the fetal heart is an obvious barrier, we found that another important barrier included in our explanatory model that may be overlooked is the concept of outcome expectancy. If sonographers do not understand the usefulness to patients of performing cardiac screening of fetal hearts, they will have less intrinsic motivation to perform it. Perceived usefulness of cardiac screening was strongly associated with sonographers’ reported intention to perform screening and their actual performance in interpreting images. Yet, as identified in focus groups, sonographers have very little understanding in terms of the early detection of heart defects and its impact on the subsequent medical care of infants, or the current detection rates.
For sonographers, the extrinsic motivators of national screening guidelines and supervisor/physician expectation were identified as important factors in focus groups and were important to their fetal heart scanning behavioral intentions and abilities.34,46 The recently enacted 2013 national guideline that specifically includes outflow tracts is just the first step in enhancing extrinsic motivation. 8 Physicians need to ensure that sites are implementing these guidelines effectively and that professional expectations and clinical practice are achieving these higher standards.
External facilitating conditions identified by sonographers, such as timing of screening ultrasound, patient body habitus, and equipment, have been identified as potential barriers to adequate screening. 42 While equipment barriers and gestational age at scan are potentially modifiable factors, fetal position and maternal weight are not readily modifiable. Sonographers identified the gestational age of the fetus at the time of imaging as a potential barrier that was outside their control but potentially modifiable through system-level changes.
Another important area highlighted by sonographers and amenable to system-level change was feedback and reinforcements from supervisors and colleagues. Currently, feedback to sonographers is highly variable and often dependent on individual initiative. Implementation of quality improvement initiatives to standardize and improve imaging is a potentially effective approach that requires further study.47,48 Another approach is to develop strategies for improving communication and developing an increasingly collaborative environment between community practices and referral centers to provide regular feedback to sonographers and physicians. While we did not find these barriers to be associated with sonographer performance on imaging interpretation, it is possible that targeting these system-level barriers would improve sonographers’ feelings of self-efficacy and enhance performance.
Limitations
This study has several limitations. While we recruited widely for our focus groups, it is possible that sonographers who participated in the focus groups and survey were more interested in fetal cardiac imaging than sonographers in general. This bias would tend to overestimate the proportion of sonographers able to accurately read the images, although the associations with the behavioral constructs are likely generalizable to the overall population of sonographers. Similarly, the sonographer views expressed regarding the desire for more training may not be generalizable to obstetric sonographers outside this region or the United States. While certain themes may cut across geographic boundaries, similar methodologies may be employed to determine barriers in other regions or countries.
Conclusion
Documenting the perspective of sonographers provides a framework for understanding factors that contribute to performance of prenatal cardiac screening images. Focus group discussions enabled us to improve our understanding of factors that influence the effectiveness of prenatal screening for CHD, as well as their relative importance, and to identify novel targets for future intervention. Combining qualitative information with a quantitative survey allowed us to identify several important barriers associated with the cardiac screening behaviors and abilities of sonographers. Further research in a nationally representative sample will allow us to confirm these findings and examine the influence of practice setting (e.g., community vs. tertiary, urban vs. rural). Similar studies should be broadened to include physicians who interpret ultrasounds to develop interventions that can have an impact at multiple points in the screening process.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The study was approved by the University of Utah’s Institutional Review Board. Focus group participants gave signed, informed consent for participation in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Primary Children’s Medical Center Foundation Early Career Award as well as an National Institutes of Health Institutional Career Enhancement Award for Nelangi Pinto (1KM1CA156723-01). This investigation was supported by the University of Utah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through grant 5UL1TR001067-02 (formerly 8UL1TR000105 and UL1RR025764).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.