
Abstract
The authors report a case of a middle-age man presenting with a category IV pressure ulcer (PU) over the sacrum. Undermining of the PU was assessed with the aid of gray-scale sonography (US), color Doppler US, power Doppler US, and a microvascular imaging technique employing advanced clutter suppression. Clutter suppression post-processing the study allowed for the evaluation of low-velocity microvascular flow in the undermined PU and facilitated the choice of appropriate treatment.
Introduction
In general practice, the damage to the subcutaneous tissue caused by a pressure ulcer (PU) is initially evaluated by visual inspection and palpation, but these techniques do not allow the assessment of deep-tissue injury. 1 Previous studies have reported the advantages of gray-scale sonography (US) in diagnosing early-stage deep-tissue injury and in predicting the prognosis of PUs.2–4 Prognostic indicators of PUs can also be assessed by using color Doppler US (CDUS) and power Doppler sonography (PDUS) to evaluate the degree of inflammation by quantitative assessment of the blood flow in visualized vessels. Conventional CDUS and PDUS apply a wall filter to remove clutter noise and motion artifacts. Because of strong clutter signals overlapping with low-velocity blood flow components, low-velocity blood flow information could be suppressed.5–8
A novel sonogram post-processing technique was used to suppress received signal clutter (Superb Microvascular Imaging®; Toshiba Medical Systems, Tokyo, Japan). It has been reported that this technique allows the visualization of low-velocity microvascular blood flow with minimal color noise. 9 A case is provided in which blood flow in an undermined PU (a category III/IV PU with necrotic tissue inside the undermined region) was visualized. The wound’s severity was evaluated by using the DESIGN-R tool, which has a scale of 0 (healed) to 66 (greatest severity).10,11 This PU was also evaluated using CDUS, PDUS, and the clutter suppression technique, to determine the amount of perfusion in the ulcer.
Case Report
A middle-age man had spent most of his life confined to a wheelchair, due to a childhood spinal cord injury. He was admitted to the hospital with a suspected postoperative ileus, caused by perforation of a duodenal ulcer. He was also noted to have a category IV PU over the sacrum. The postoperative ileus was treated with a nasogastric tube. The hospital’s PU team assumed the management during the patient’s in-hospital stay of 14 weeks.
Diagnostic ultrasound equipment (Aplio® ultrasound system; Toshiba Medical, Ltd., Tokyo, Japan) was used to image with a linear-array (18 MHz) transducer. The sonographic interrogation was based on a focal range and image-depth thickness of 1 to 3 cm, to determine the correct display range. The echo gain was set at 80, the dynamic range at 60, and differential tissue harmonic imaging at 18.0. The patient was placed in the lateral position for imaging. Sagittal images, supplemented by transverse and oblique views of the ulcer and its underlying structures, were obtained in overlapping planes. After the gray-scale sonographic examination, the patient underwent CDUS, PDUS, and clutter suppression imaging in the sagittal plane, with the patient in the same position and equipment settings.
The PU (width, 74 mm; length, 59 mm; DESIGN-R score, 41 points) was category IV with undermining (larger area of the lesion than the degraded pore) PU. The patient was followed until discharge from the hospital. Sonographic images of the undermined PU portion demonstrated a distinct hypoechoic area (granulation tissue; proliferating new organization owing to improvement of the tissue-injured portion) with irregular borders and small cystic foci located within the subcutaneous fat layer of the sacral region (Figure 1). Color Doppler US and PDUS demonstrated prominent vessel signals with color blooming artifact (displays color outside of a vessel and makes vessels appear) and color noise. Of the two techniques, PDUS was better than CDUS at visualizing the color signal of the granulation tissue (Figures 2A and 2B). However, unlike CDUS and PDUS, clutter suppression imaging revealed the color signal of the microvasculature in the granulation tissue (Figure 2C).
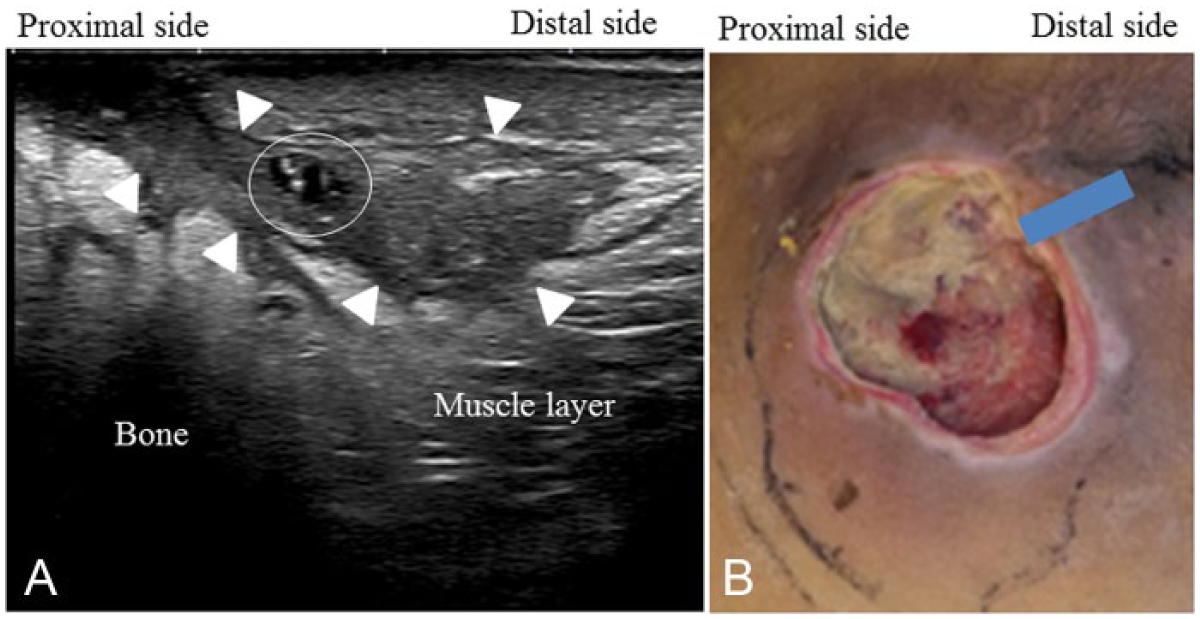
(A) Longitudinal scan obtained during sonography of the hypoechoic area (granulation tissue) and an internal spotty cystic area (representing fluid: circle) inside the undermining (arrowheads). (B) Photograph of the same category IV pressure ulcer in the sacral region after 7 weeks of follow up. Blue line, observation point of the sonogram.
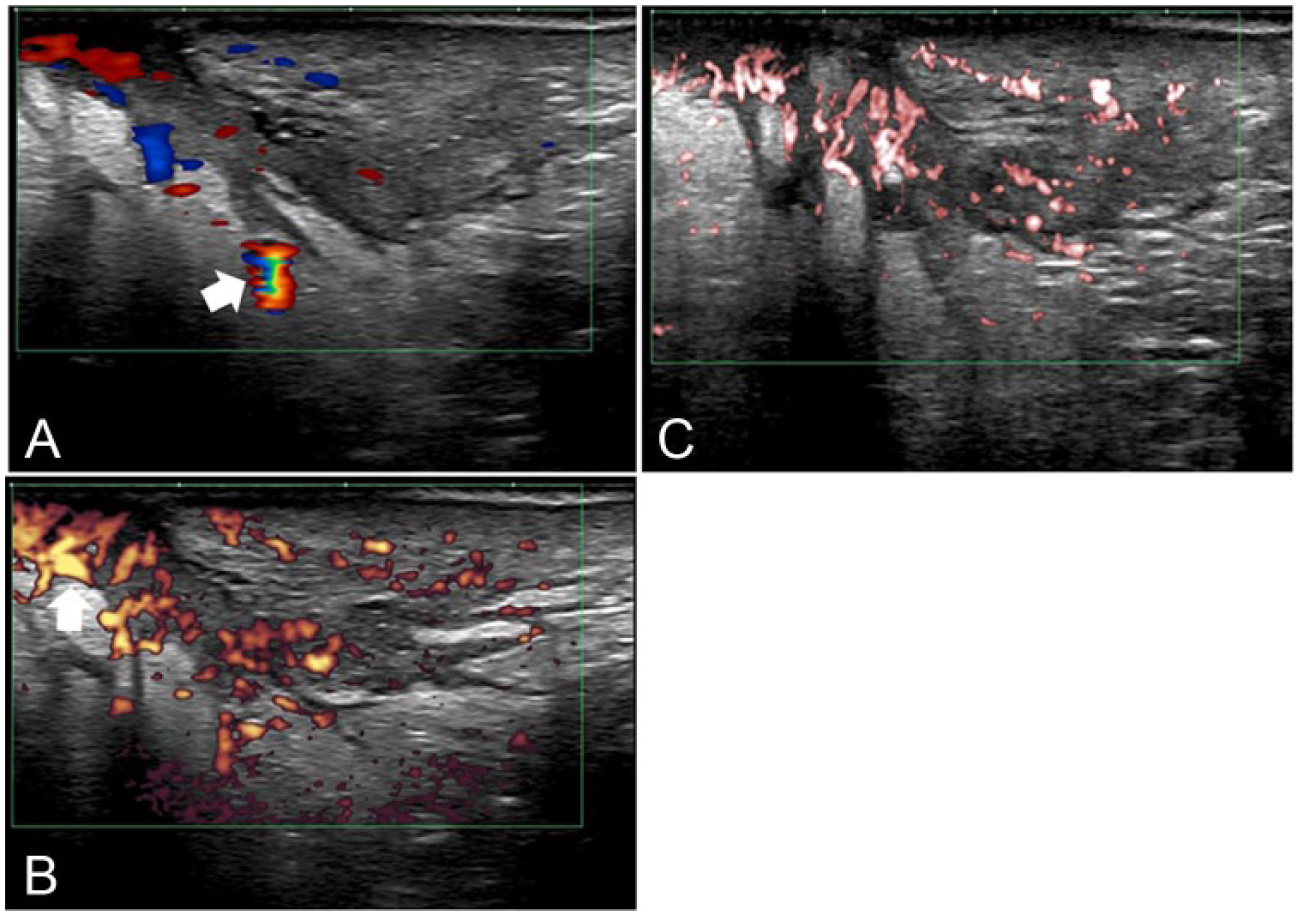
Color-signal sonograms inside the undermined pressure ulcer. The images were obtained with color Doppler sonography (CDUS), power Doppler sonography (PDUS), and microvascular imaging. (A) With CDUS, the color signal shows a prominent blooming effect and color noise (arrows); color gain, 45. (B) The color signal of the granulation tissue is stronger with PDUS than CDUS, but blooming effects and color noise remain; color gain, 52. (C) On clutter suppression imaging, the color signal of the microvasculature in the granulation tissue is subject to fewer blooming effects and less color noise; color gain, 43.
Discussion
This case study demonstrated the use of clutter suppression imaging to visualize the undermined tissue and ulcer itself. This technique provided new information especially regarding the amount of perfusion in the granulation tissue. Clinically, clutter suppression imaging has the advantage over CDUS and PDUS as it can reduce blooming artifacts, enabling the separation of blood flow from the surrounding tissues. As shown by these preliminary results, clutter suppression imaging may be suitable for assessing low-velocity microvascular flow in undermined PUs and may have greater sensitivity for small vessels than either CDUS or PDUS.
Color Doppler US is a useful tool for assessing active inflammatory disease, although PDUS is more sensitive in the detection of flow in small vessels.12–14 However, both CDUS and PDUS are subject to blooming effects from vessel signals as well as color noise and clutter artifacts resulting from the Doppler signals. Both blooming effects and color noise produce distortions in the sonographic appearance of the imaged structure, in particular artificially low blood-flow velocity measurements.5,6,8 Although PDUS can be used in the imaging of low-velocity blood flow, blooming artifacts are still problematic. 7
In this patient with an undermined PU, clutter suppression imaging clearly demonstrated the microvascularity of the granulation tissue, which appeared hypoechoic. Because the damage involved the subcutaneous fatty tissue and muscle, 20 to 30 mm below the skin surface, the undermined PU in the surrounding normal tissue was not recognized by clutter suppression imaging. 5 The precise localization of blood vessels by clutter suppression imaging enables the safe debridement of the undermined necrotic tissue region.
Conclusion
Clutter suppression image processing could allow for the visualization of smaller vessels with greater sensitivity and fewer motion artifacts than other Doppler imaging techniques. Based on this case, clutter suppression image processing may have potential for the assessment of blood-vessel signals in undermined tissue and could be studied further with a larger cohort of patients.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The ultrasound system was rented from Toshiba Medical Systems, Tokyo, Japan. The company did not have any role in this case study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.