
Abstract
Sonographers are acquainted with the signs, symptoms, and findings of ectopic pregnancies as well as their recurrence; however, a recurrent ipsilateral ectopic pregnancy after a salpingectomy is also possible. While recurrent ipsilateral ectopic pregnancies are rare, they are a significant diagnostic discovery. It is important to highlight this rare manifestation and be aware of the potential for recurrent ipsilateral findings to avoid a misdiagnosis or prolonged treatment. The goal of this case study is to review a patient’s presentation and raise awareness of recurrent ipsilateral tubal ectopic pregnancy.
Although ectopic pregnancies account for about only 2% of all gestations, the rate of ectopic pregnancy has increased substantially over the last several decades. 1 It is thought that the increase is due to a higher rate of tubal infections and greater use of in vitro fertilization. 2 Fallopian tubes are the most common location for this to occur and account for 93% to 97% of all ectopic pregnancies. 3 Recurrent ectopic pregnancies are rare and range anywhere from 6% to 28%. 2 Ipsilateral (or same side) ectopic pregnancies following a salpingectomy are rarer still, with fewer than a dozen cases documented in the English literature over the last 10 years. 4
The risk factors for a recurrent ipsilateral ectopic pregnancy are similar to that of an initial ectopic pregnancy. A previous ectopic pregnancy significantly increases the risk of a recurrent ectopic pregnancy with each incidence. If a patient has had one ectopic pregnancy and salpingectomy, she has a 15% to 20% chance of reoccurrence. If she has had two ectopic pregnancies, the risk of reoccurrence increases to 32%. 5 A history of tubal surgery, pelvic surgery, or pelvic inflammatory disease significantly increases the risk of a recurrent ectopic pregnancy. A recent study found that a patient with at least one live birth has more of an increased risk of ectopic pregnancy than a nulliparous patient. 6
A recurrent ipsilateral tubal ectopic pregnancy can have a similar sonographic appearance as initial tubal ectopic pregnancy. What can be unexpected is that the ectopic pregnancy can appear on the same side as the previous occurrence after a laparoscopic salpingectomy. A reoccurrence can have the same appearance as an initial tubal ectopic pregnancy, and there is usually no evidence of intrauterine pregnancy (IUP). However, about 10% to 20% of the time, a pseudogestational sac or decidual cast may be visualized in place of an IUP.7,8 Beyond the routine sonographic findings that can be used, spectral Doppler can be used as a last resort to distinguish a normal sac from a pseudogestational sac. An IUP will typically demonstrate peritrophoblastic flow, which has a low-resistance pattern with peak velocities of 20 cm/s. A pseudogestational sac can demonstrate a high-resistance pattern with low peak velocities. 9
There is typically a simple or complex extra-adnexal cyst or mass separate from the ovary, and about 95% of the time with tubal ectopic pregnancies, the mass is complex.7,10 One way to differentiate between a tubal mass and a corpus luteal cyst is to carefully palpate the area of the mass while scanning. If gentle massage causes the suspected mass to move independently, this may be consistent with an ectopic pregnancy. If the mass moves with the ovary, this raises the likelihood that it is a corpus luteal cyst. About 95% of the time, the adnexal mass will be a tubal ring sign.7,8 A sonographic ring-of-fire sign can be demonstrated with color Doppler as peripheral vascularity. Since this sign can also be seen with a corpus luteal cyst, using spectral Doppler will help differentiate between a corpus luteal cyst and an ectopic pregnancy. A resistive index <0.40 suggests an ectopic pregnancy.9,11 Be sure to carefully examine both adnexa because a recurrent tubal ectopic pregnancy can be on the same side even with a past salpingectomy. 1
Case Study
A 32-year-old woman (G4, P2, AB1) presented for an obstetric sonogram. Her serum levels for β subunit of human chorionic gonadotropin (β-hCG) were 2891 mIU/mL. Her last menstrual period suggested a gestational age of 7 weeks 5 days. She had been experiencing pelvic pain for 2 days, which had escalated to pelvic and rectal pain with severe vaginal bleeding. An obstetric sonogram was performed with Mindray ultrasound equipment (Mindray, Oxnard, California) with a 4- to 6-MHz curvilinear array and a 6- to 8-MHz endocavity transducer. Sonographic findings included a thickened endometrium without an IUP (Figure 1), a sonographic tubal ring sign, a ring-of-fire sign, and free fluid in the cul-de-sac (Figure 2). No fluid was seen in Morison’s pouch. A left extra-adnexal mass (2 × 2.4 × 1.7 cm) containing a gestational sac (0.90 × 0.60 × 0.80 cm) was imaged (Figure 3). Fetal heart tones of 83 beats per minute were noted (Figure 4). The average ultrasound gestational age was calculated at 5 weeks 5 days.

A gray-scale transabdominal image that demonstrates the uterus in the sagittal plane.

A gray-scale transvaginal sagittal view of the uterus, with a thickened endometrium, free fluid, and extrauterine mass with a tubal ring sign.

A magnified sagittal view of an adnexal mass that contains a gestational sac.
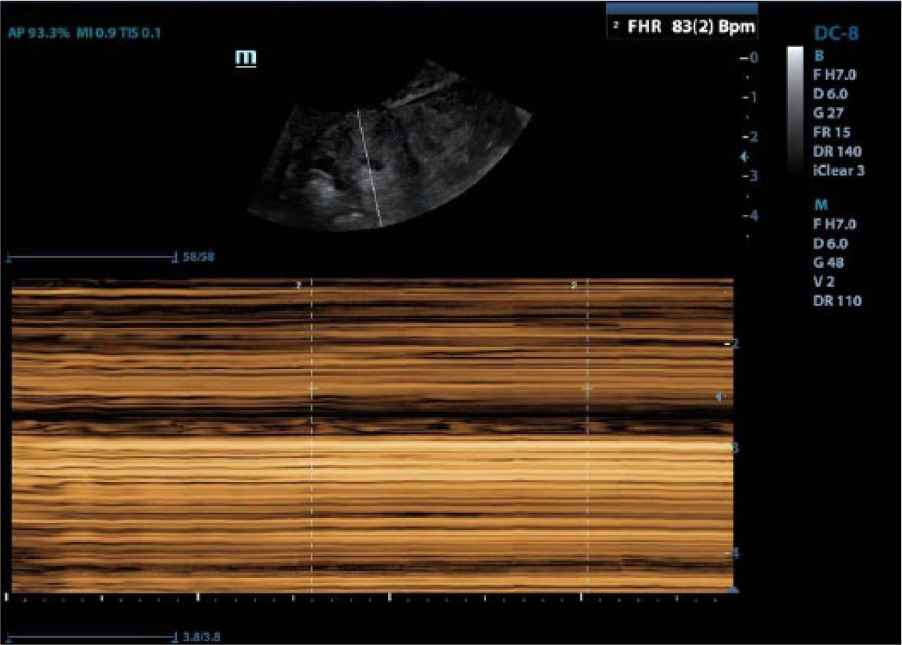
An M-mode tracing of the fetal heart rate within the ectopic pregnancy.
These findings were suggestive of a left tubal ectopic pregnancy, and the patient was taken to surgery, where the ectopic pregnancy was confirmed and a left laparoscopic salpingectomy was performed. Her serum β-hCG levels were monitored as decreasing to zero. Because the patient indicated that she planned to attempt another pregnancy, she was advised to come back immediately when she had a positive pregnancy test.
The patient returned in 1 month for a follow-up after an emergency department visit due to right lower quadrant pain. Her serum β-hCG level was 192 mIU/mL and increased to 1325 mIU/mL 4 days later. The sonogram showed a thickened endometrium (Figure 5), a corpus luteal cyst on the right ovary (Figure 6), a left ovary within normal limits (Figure 7), and a left extra-adnexal mass with a gestational sac inside with fetal heart tones noted (Figure 8). The average ultrasound gestational age was calculated at 6 weeks 0 days (Figure 9). Since the extra-adnexal mass and gestational sac were seen on the left side after the patient had a left salpingectomy, it was thought that it might be a cornual or abdominal ectopic pregnancy.

A gray-scale transvaginal sagittal view of the nongravid uterus.
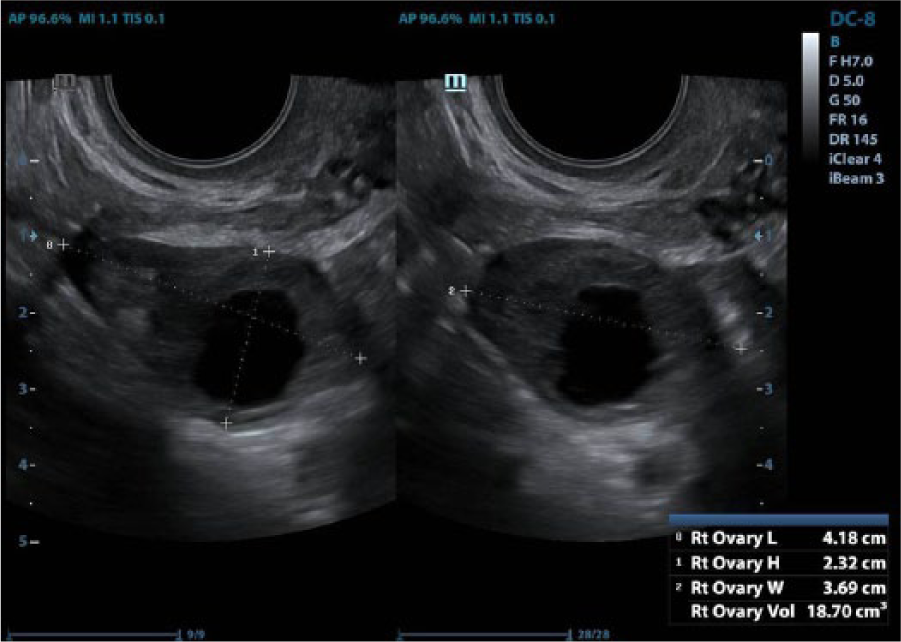
A transvaginal image of the right ovary with a corpus luteal cyst.
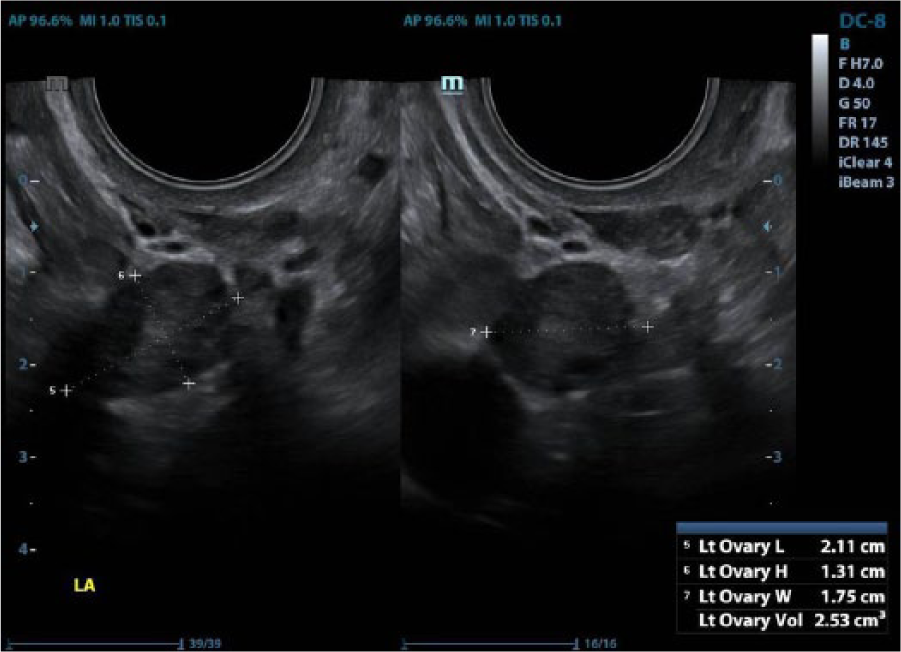
A dual sagittal and transverse set of images of a normal left ovary.
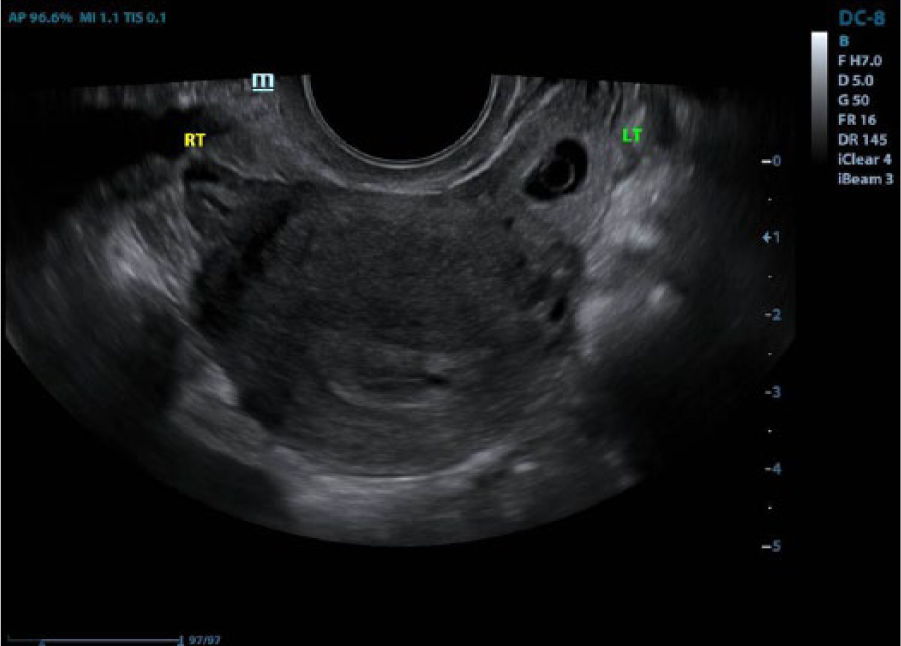
A coronal image of a uterus with a left adnexal mass.
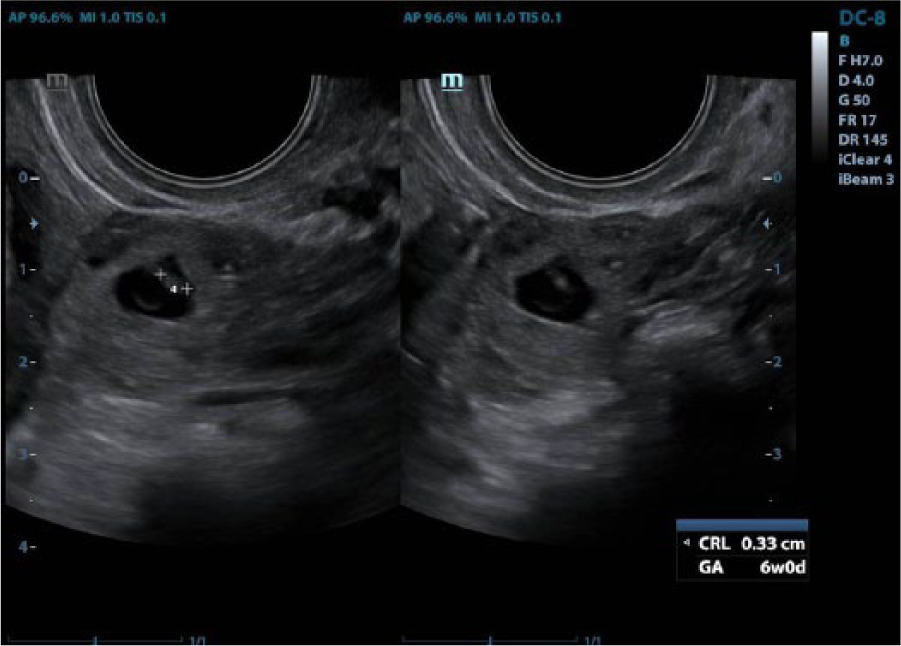
A magnified set of images of a left adnexal mass and measurement of the fetal pole.
The patient was promptly taken to surgery, and it was determined that the recurrent ectopic pregnancy was ipsilateral within the remaining fallopian tubal stump (Figure 10). The patient needed a second left laparoscopic salpingectomy. Best practices advise monitoring a patient’s serum β-hCG levels to zero following an ectopic pregnancy and a laparoscopic salpingectomy. In cases where the serum β-hCG levels have not properly decreased as anticipated, then further treatment may be necessary (e.g., methotrexate). 12 Although no record was available indicating when this patient’s serum β-hCG levels fell to zero after her second salpingectomy, her postoperative visit showed no complications from the procedure. The patient went on to have a successful term pregnancy the following year.
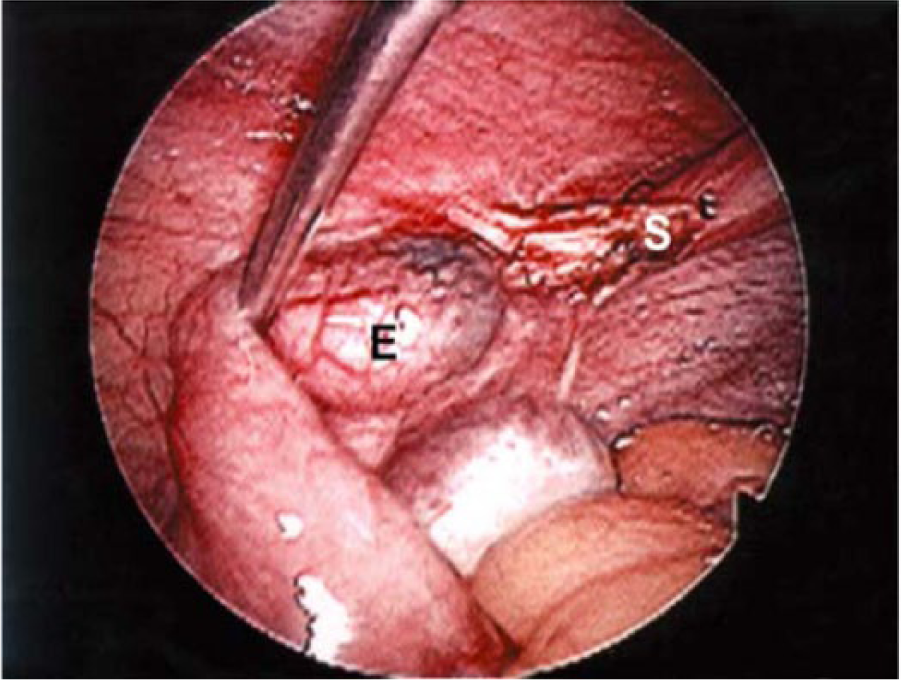
A similar case demonstrating a laparoscopy of an ipsilateral recurrent pregnancy. The letter S indicates the site of the first partial proximal left salpingectomy. The letter E indicates the ectopic pregnancy in the distal remnant of the left fallopian tube. Reproduced from Zuzarte and Khong, Recurrent ectopic pregnancy following ipsilateral partial salpingectomy, Singapore Med J 2005;46(9):476-8.
Discussion
A fallopian tubal ectopic pregnancy usually occurs when the fertilized embryo becomes implanted in the tube, on its way to the uterus. There are numerous reasons for this, including a damaged fallopian tube, hormonal imbalances, or a fertilized embryo that has developed abnormally. Currently, the exact pathogenesis regarding an ipsilateral ectopic pregnancy is unknown. However, there are several theories. One is that the ovum can still be fertilized within the fallopian tubal stump by spermatozoa traveling through the patent tube, into the cul-de-sac, and through the damaged tube. Another possibility is the intrauterine migration of the ovum throughout the reproductive track. The oocyte is fertilized from the contralateral ovary in the patent tube only to travel via the uterus and implant in the remaining fallopian tubal stump. Last, the remaining fallopian tubal stump may still have some patency after ligation. Usually, the tubal stump is ligated after the salpingectomy, but it can still hold some patency or even recanalize. If this is the case, then there is a possibility for a fertilized ovum to implant in the isthmic portion of the tubal stump4,13,14 (Figure 11).
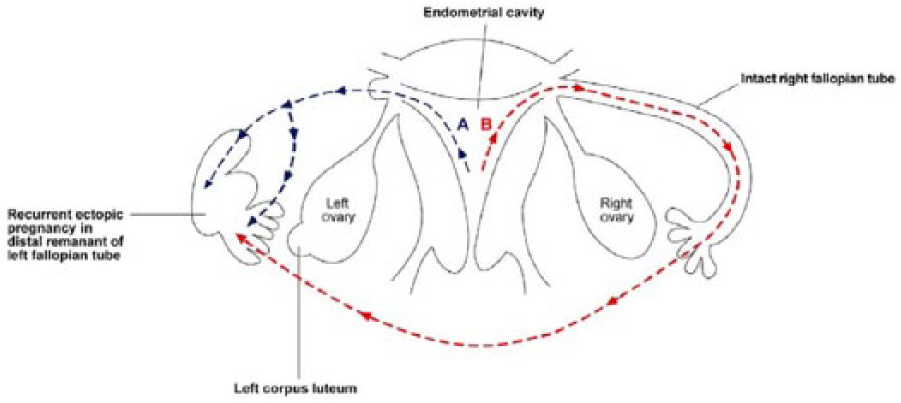
Two possible pathways that the fertilized ovum may travel, in a similar case. Pathway A represents spermatozoa or the fertilized egg traveling from the uterus to the distal remnant of the left fallopian tube after partial salpingectomy. Pathway B represents the spermatozoa traveling through the intact right fallopian tube and the pouch of Douglas into the left tubal stump. Reproduced from Zuzarte and Khong, Recurrent ectopic pregnancy following ipsilateral partial salpingectomy, Singapore Med J 2005;46(9):476-8.
A laparoscopic salpingectomy, where the fetus and tube are removed, has been the most common way to treat the patient. Due to the increasingly early diagnosis of ectopic pregnancy as well as the preservation of fertility, salpingotomy has been used as a more conservative treatment.1,15 Methotrexate, a folic acid antagonist, is used in cases where a patient has had previous surgery or extensive pelvic adhesions. It has a success rate of 70% to 97% and works best when there is no fetal cardiac activity, no tubal rupture, and a low serum β-hCG level. It affects the trophoblast, which is a highly proliferative tissue, by impeding DNA synthesis and cell production.1,16 Expectant management is recommended when patients are closely monitored and there are no complications due to the self-absorption of ectopic pregnancies. Also, in cases where there is still a question of an early IUP versus spontaneous abortion versus an ectopic pregnancy, monitoring is the best option so that the patient is not needlessly treated. 16
Overall, ectopic pregnancies account for 73% to 75% of first-trimester maternal deaths4,17 and approximately 9% to 15% of all pregnancy mortalities.1,5,17 Still, fallopian tubal ectopic pregnancy has a better prognosis since it has a lower risk of rupture, 10 about 10% to 15% of the time. 9 However, the mortality rate with recurrent ipsilateral tubal ectopic pregnancies is about 10 to 15 times higher than other ectopic pregnancies. 4
Nearly 95% of tubal ectopic pregnancies are located in the ampullary segment and have a lower risk of rupture. Following a salpingectomy for an ampullary tubal ectopic pregnancy, a portion of the fallopian tube called the tubal stump may remain. A recurrent ipsilateral tubal ectopic pregnancy is most likely to occur in the interstitial or isthmic portions of the tubal remnant. Due to the elasticity of the myometrial layer that surrounds the interstitial segment of the fallopian tube, the embryo can survive up to 7 to 16 weeks of gestation before possibly rupturing. By the time that the rupture occurs, there will be severe hemorrhaging because of the size of the gestation, as well as the amount of blood supply going to that area from the uterine and ovarian vessels. If the ipsilateral tubal ectopic pregnancy reoccurs in the isthmic segment, the risk of rupture is higher because of the inability of this portion of the fallopian tube to properly expand along with the growing gestation. This results in an increased probability of rupture and massive hemorrhaging at an early gestational age. Statistically, interstitial and isthmic ectopic pregnancies account for 2.0% to 2.5% of mortalities, whereas other types of ectopic pregnancies make up about only 0.14% of mortalities. It is good practice to evaluate a patient at risk for a recurrent ectopic pregnancy, specifically the ipsilateral side.1,4,18
There are a few ways to help prevent recurrent ipsilateral tubal ectopic pregnancies. When a salpingectomy is being performed, it would be best to leave a short tube instead of a long tube. Usually, a long tube is left to minimize risk of bleeding from the isthmic portion of the tube; however, this could increase the risk of a recurrent ipsilateral tubal ectopic pregnancy. Once the salpingectomy and ligation have been completed, a hysterosalpingography (HSG) is a good way to assess if patency is left in the fallopian tubes. One way to ensure that fallopian tube patency has been permanently occluded is to place flexible microinserts (e.g., Essure) within the remaining stump of the fallopian tube. This could help to decrease the risk of future implantation. After the procedure, it is important to determine whether the microinserts were placed correctly and that the fallopian tube has been permanently occluded. 19 An HSG or a sonosalpingography (SSG) can be performed to assess patency. When it comes to tubal patency evaluation, research has shown that an HSG has a sensitivity of 91.67% and a specificity of 100%, while the SSG has a little higher sensitivity of 95.83% and a specificity of 100%. The SSG has been suggested as the first choice in evaluating patency, mainly because it is a safe, noninvasive outpatient procedure that is very tolerable and does not use ionizing radiation like the HSG.20-22 Still, in some cases, it may be even more prudent for the patient to consider implementing more permanent contraceptive measures.4,19
Conclusion
As the risk and occurrence of ectopic pregnancies increase, so does the need for understanding and prompt diagnosis due to the mortality rate associated with a recurrent ipsilateral ectopic pregnancy. Sonography is the gold standard in diagnosing an ectopic pregnancy, with a sensitivity of 100% and a specificity of 100%. 23 Sonography is extremely useful in finding the location of the ectopic pregnancy, identifying other signs to diagnosis an ectopic pregnancy, and detecting if a rupture has occurred.
Given that the risk of a recurrent ipsilateral ectopic pregnancy after a salpingectomy is possible, then it is worth reviewing the patient’s history, as well as current signs and symptoms to increase detection rates. It is important to look in multiple anatomic areas, such as bilateral adnexa, the cul-de-sac, and retroperitoneum spaces for fluid. Sonography is also helpful in determining the best possible treatments, such as monitoring a small ectopic pregnancy, prescribing methotrexate, and conducting surgery and follow-up. As sonographic resolution advances, even earlier diagnoses can be made, which will allow for expedient treatment and possible preservation of the patient’s fertility.
Footnotes
Acknowledgements
I dedicate this article to friends and family, in particular my parents, Daisy Harris and Willie Boykin, for supporting me in everything, especially during the El Centro College diagnostic medical sonography program. I could not have done it without all of you. I also thank Caring for Women in Denton, Texas, and the Singapore Medical Journal for their contribution of images and case reports. A special thanks to Eden Chavira, RDMS (OB/GYN, NT), and Lynn Schluns, BS, RDMS, RVT, for their assistance, encouragement, and guidance in writing and submitting this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.