
Abstract
Cesarean section (C-section) ectopic pregnancies (CSEPs) refer to the implantation of an embryo in the fibrous scar tissue from a previous cesarean section. C-section ectopic pregnancies pose a significant risk for uterine rupture and maternal morbidity, therefore early identification is imperative. Early detection and diagnosis of a CSEP can be difficult and follow-up imaging is often recommended. Recurrence in CSEPs may be observed, and this case study confirms the clinical importance of obtaining patient history in addition to a well-visualized pelvic sonogram.
An ectopic pregnancy occurs when implantation happens outside the endometrium. There are various types of ectopic pregnancies, including: tubal, ovarian, abdominal, cervical, and cesarean scar ectopic pregnancies. A cesarean section (C-section) ectopic pregnancy (CSEP) occurs when a gestational sac implants into the scar of a previous cesarean section incision, typically in the lower segment of the uterus. Sonography is the key component in detecting CSEPs. The incidence of CSEP has been found to be 1:1800 to 1:2500. 1 C-section ectopic pregnancies are becoming more common due to a higher incidence of births overall and C-section surgeries. Sonographers should have a detailed understanding of the appearance of CSEP and should always obtain a detailed history from the patient about any prior uterine surgeries and pregnancies. The following case provides a detailed description of a patient with recurrent CSEP.
Case Report
A 28-year-old G4P3 woman presented to the emergency department (ED) with vaginal bleeding, cramping, and a positive home pregnancy test. The beta-human chorionic gonadotropin (β-hCG) bloodwork drawn at this time was 1987. The patient had a history of two low transverse C-sections, the most recent surgery being 6 months prior. The patient also had a history of one vaginal delivery secondary to premature rupture of membranes, at 28 weeks gestation, resulting in a neonatal demise.
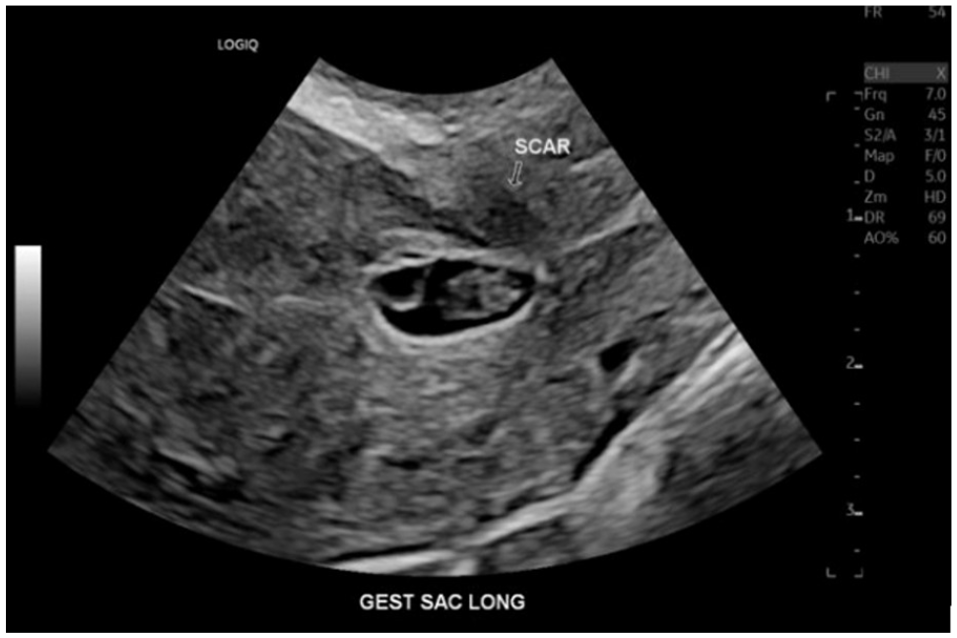
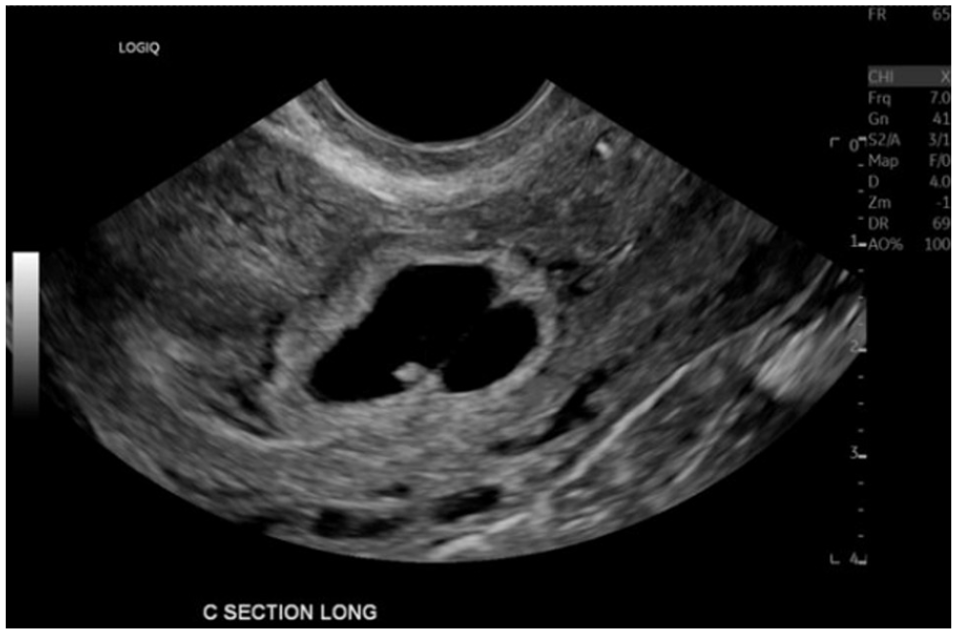
A transabdominal and transvaginal pelvic sonogram was performed utilizing a Logiq E10 ultrasound system (GE Medical Systems, Wauwatosa, Wisconsin) using a RIC 5-9-D MHz transducer. The protocol consisted of evaluating the uterus, ovaries, and both right and left adnexas thoroughly using grayscale, color, and spectral Doppler in transverse and sagittal planes. The examinations demonstrated concern for inevitable abortion versus CSEP. A follow-up repeat imaging examination was recommended. The patient returned to the ED 6 days later with worsening vaginal bleeding and cramping. Her β-hCG level drawn at this time was 3168. A pelvic sonogram was performed and a CSEP was noted in the cesarean scar, located in the lower uterine segment. The gestation and fetus measured 6 weeks and 2 days, based on the crown rump length (CRL) (See Figures 1 and 2). A normal first trimester sonogram would have been expected to demonstrate a gestational sac, within the endometrium. A dilation and curettage (D&C) surgery was performed the same day and pathology confirmed the diagnosis of CSEP.

An endovaginal sonogram demonstrating a sagittal view of the uterus containing a C-section scar ectopic pregnancy, in the lower uterine segment. (Note: This was the second visit to the emergency department.)
An endovaginal sonogram demonstrating a gestational sac implanted into the C-section scar. (Note: This was the second visit to the emergency department.)
The patient returned to the ED 5 months later with similar symptoms: spotting, cramping, and a positive home pregnancy test. The β-hCG level drawn at this time was 66, 357. A pelvic sonogram was performed using the same ultrasound equipment system with a RIC 5-9-D MHz transducer. The findings were consistent with a dichorionic-diamniotic twin CSEP (See Figures 3 and 4). Two gestational sacs were seen within the lower uterine segment, one gestational sac with a fetal pole and one without. A D&C was performed and a Nexplanon contraceptive implant was placed at this time. Pathology containing immature chorionic villi was consistent with another CSEP.
An endovaginal sonogram demonstrating a C-section ectopic with twin gestation visualized in the sagittal view. (Note: The third visit to the emergency department.)

An endovaginal sonogram that demonstrates a twin gestation C-section ectopic pregnancy, visualized in the transverse view. (Note: This was the third visit to the emergency department.)
Discussion
Ectopic pregnancies are to be taken seriously as they can result in serious consequences if not identified correctly. If there is a positive β-hcG and a gestational sac is not identified within the endometrium, the sonographer should be alerted that an ectopic pregnancy is possible. Both adnexas should be evaluated for a tubal ectopic as well as both ovaries for ovarian ectopic pregnancies. Heterotopic pregnancies are also a possibility so the entire pelvis should always be thoroughly evaluated. The cervix should be evaluated for a cervical ectopic as well as any C-section scars. C-section ectopic pregnancies are a rare type of pregnancy that pose a threat to maternal life and are one of the most concerning post-C-section complications. They may result in hemorrhage, hysterectomy, and maternal death. Sonography is the key method for early diagnostic detection. It is crucial for sonographers to provide quality images and obtain a detailed patient history for the radiologist to make a concise diagnosis. Questions such as “have you ever had a C-section” or “have you ever had an ectopic pregnancy?” will aid in making a diagnosis.
An early sonographic evaluation of a CSEP can often be difficult and may have a differential diagnosis of a spontaneous abortion due to its low-lying location in the lower uterine segment. This may appear like an active spontaneous abortion. One way to differentiate an early CSEP from a spontaneous abortion is the use of gentle transducer pressure to determine whether there is a “sliding organs sign,” also known as a “sliding sac sign.” A sliding organs sign is demonstrated when the gestational sac displaces with the use of gentle transducer pressure. Criteria for diagnosing a CSEP include a negative sliding organs sign, meaning the gestational sac will not displace from its position when transducer pressure is used. If the gestational sac displaces with the pressure, it likely indicates an active spontaneous abortion, rather than a CSEP. Using this maneuver may assist a radiologist in their diagnosis and lead to an earlier treatment plan for the patient. 2
C-section ectopic pregnancies have become a more common occurrence in the last decade, making recurrence also more common. The embryo implants into the C-section scar by going through a dehiscent tract made by a previous incision into the myometrium. 3 The implantation site can be identified as “exogenic,” meaning implanted within the scar or “endogenic,” meaning on the site of the scar in the uterine cavity. 4 Implantation on or within the scar has a high risk of uterine rupture due to the compromise and weakening of the myometrial tissue, especially in women with a history of multiple C-sections. Another risk factor for CSEP is a short interval between a C-section and the following conception. 5
Treatment for CSEP varies, but most often consists of an immediate D&C due to the high risk of uterine rupture and maternal morbidity. Additional treatment options consist of a wedge resection, intra-gestational methotrexate, or a combination of treatments. 4 A study conducted of 252 cases throughout six obstetric and gynecological departments between 2010 and 2019 reported that 34.3% of women with CSEPs have had at least one incidence of recurrence, and three of these women had more than one incidence of recurrence. This study did not confirm any association of the recurrence rate and the treatment method of the initial CSEP. This confirms the importance of taking the time to acquire a patient history prior to the examination in order to recognize the potential recurrence early in pregnancy. 6
Conclusion
The importance of diagnosing CSEPs early is crucial in minimizing maternal risk. A combination of sonography, clinical symptoms, and patient history are all criteria for confidently making this diagnosis. Sonographers should have an extensive understanding of the appearance of CSEPs and should take precaution on differentiating them from early spontaneous abortions using the “sliding organs sign” maneuver. Surgical history should always be reviewed prior to the examination in order to understand the presence and extent of scar tissue in the uterus. The increasing prevalence of recurrent CSEPs should be taken into consideration.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because only anonymous information was used in this report.
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.