
Abstract
Solid pseudopapillary epithelial neoplasms are a rare form of exocrine pancreatic tumors. While most of these neoplasms are benign, small percentages are malignant. Complete resection is associated with long-term survival, even in the presence of metastatic disease. This case study presents a solid pseudopapillary epithelial neoplasm arising from the pancreatic tail. The pancreatic neoplasm was initially detected as an incidental finding sonographically and then further investigated by magnetic resonance imaging. This case highlights the importance of documenting incidental findings during sonography and how the combination of multiple imaging modalities provided an accurate diagnosis that led to proper treatment.
A solid pseudopapillary epithelial neoplasm (SPEN) is a fairly rare pancreatic tumor that is usually seen in young women. 1 Until 1995, only 300 reported cases of this neoplasm were documented. 2 However, with increased awareness by health care professionals, the number has increased to approximately 600 reported cases each year. 2 SPEN accounts for 1% to 2% of all exocrine pancreatic tumors. 1 The prognosis for patients with SPEN is good, with complete resection being the primary treatment option. 1 In most reported cases, SPEN was an incidental finding on a routine sonogram. 1 Because of the nature of this pathology and the reported clinical symptoms of vague abdominal discomfort, sonography is an important imaging tool to aid in the detection of this rare pathology. This case report illustrates the importance of documenting incidental findings, and it discusses the sonographic appearance of SPEN, the risk factors and characteristics associated with SPEN, and the importance of comparing multiple imaging modalities to reach a comprehensive diagnosis.
Case Report
A 34-year-old woman with a history of uncontrolled hypertension presented to the sonography department for a renal duplex sonogram. A curvilinear-array transducer with a frequency of 4.7 MHz was used on GE LogiqE9 (Waukesha, Wisconsin) ultrasound equipment.
The renal duplex sonogram demonstrated no evidence of renal artery stenosis. The sonographic appearance of the kidneys and renal artery velocities were all within normal limits. While the left kidney was being evaluated, a large round well-defined isoechoic-to-hyperechoic heterogeneous mass was detected superior to the left kidney, near the hilum of the spleen (Figures 1 and 2). The greatest dimension of the mass was visualized at the hilum of the spleen, measuring 6.4 × 6.3 × 6.2 cm (Figures 3 and 4). Color Doppler evaluation demonstrated no flow within the mass but did demonstrate the presence of flow surrounding its periphery (Figure 5). No other masses were visualized, and the origin of this mass could not be definitively identified sonographically. Based on the incidental sonographic findings, a magnetic resonance imaging (MRI) study was recommended for further evaluation.

Sonogram demonstrating a heterogeneous mass superior to left kidney (LK) and medial to the spleen (SPL) in the transverse plane.
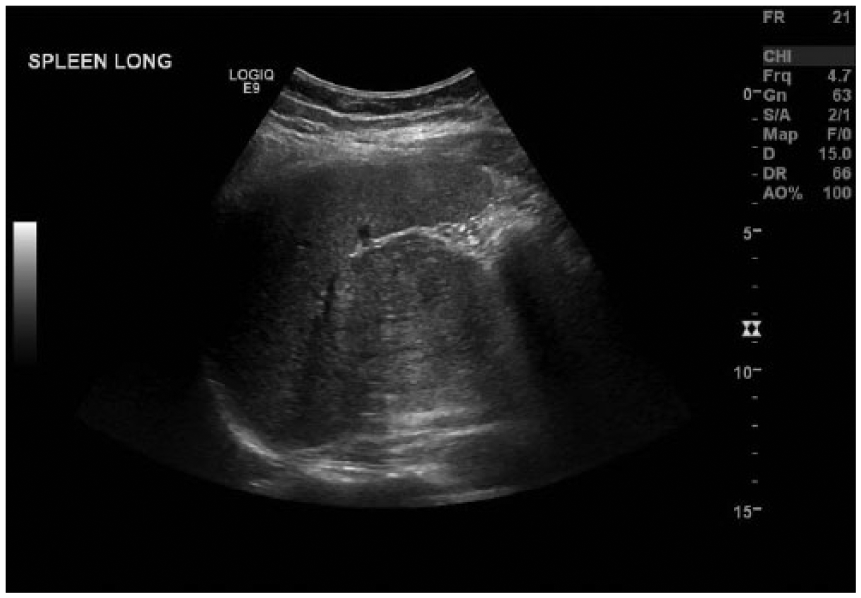
Sonogram demonstrating a well-defined heterogeneous solid mass near the splenic hilum in the longitudinal plane.
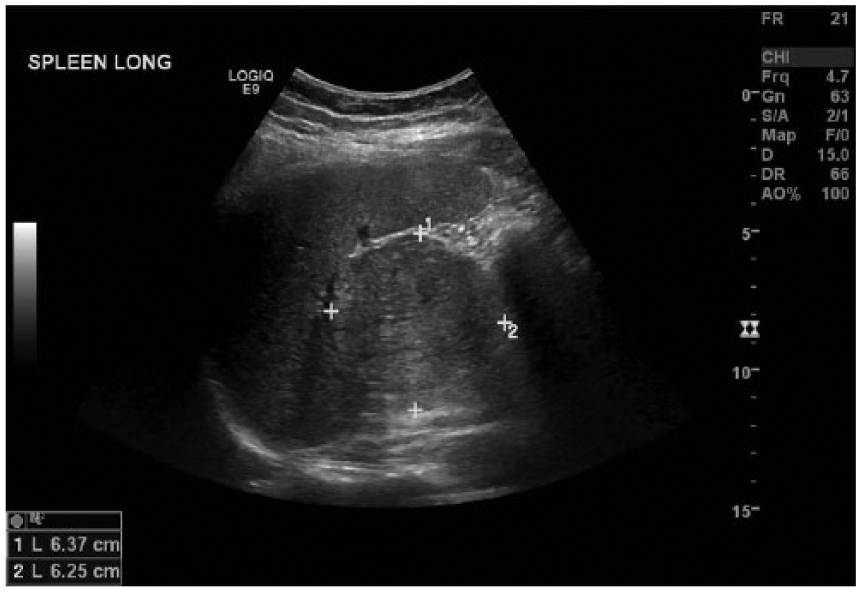
Sonogram demonstrating the approximate measurements of the mass in the longitudinal plane.
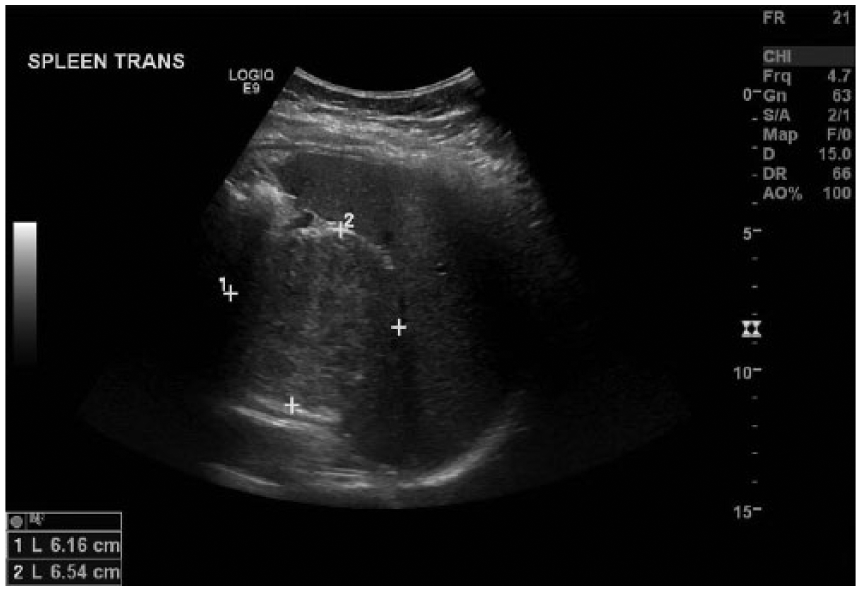
Sonogram demonstrating the approximate measurements of the mass in the transverse plane.
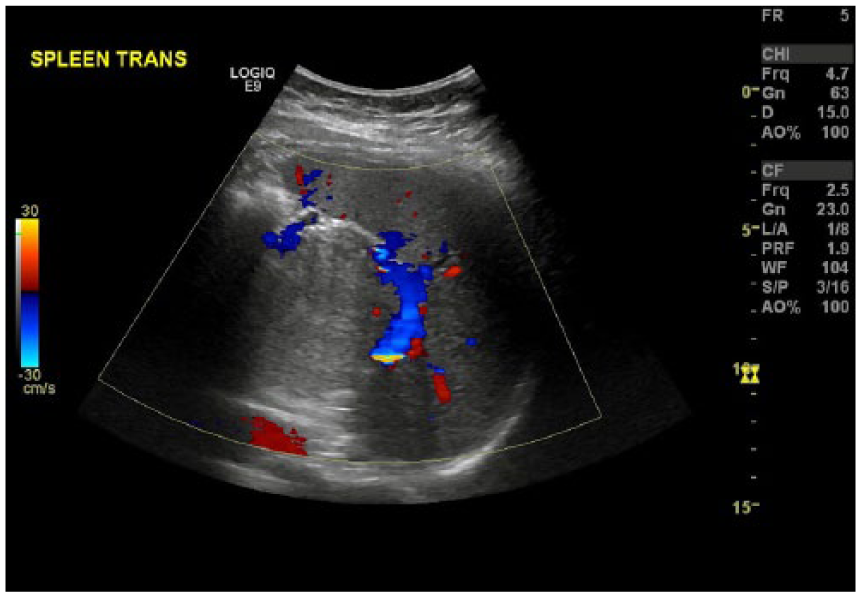
Sonogram with color Doppler of the mass near the splenic hilum demonstrating no internal flow but surrounding flow around the periphery of the mass.
Abdominal MRI with and without contrast was performed the following day. The results were comparable to the sonographic findings in that the mass was classified as well defined, measuring 6.8 × 5.6 × 6.1 cm. It was reported as having a heterogeneous low signal intensity of T1-weighted images, which indicated high water density in the tissue suggestive of a tumor. The report also stated that the mass had a heterogeneous high T2 signal intensity, which also indicated increased water density suggestive of a tumor (Figures 6 and 7). The mass was seen extending from the pancreatic tail, and it seemed to compress the splenic vein, which appeared patent. The pancreatic tail mass was suggested as being consistent with SPEN, while other considerations included pancreatic adenocarcinoma and gastrointestinal stromal tumor.

Magnetic resonance image demonstrating the well-circumscribed heterogeneous low signal intensity of a T1-weighted image of a mass extending from the pancreatic tail.
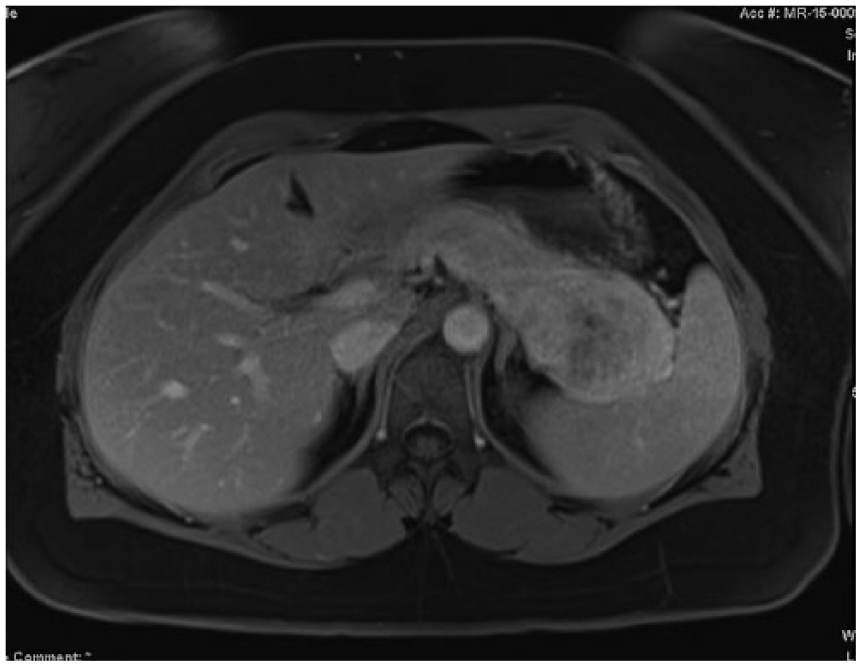
Magnetic resonance image demonstrating a well-circumscribed heterogeneous slowly progressive enhancement of postcontrast T1 images of a mass extending from the pancreatic tail.
Based on the sonography and MRI findings, surgery was performed within the next 2 weeks, and the mass was completely resected, along with the tail of the pancreas and the entire spleen. When the mass was removed, it measured 8.0 cm. The patient had no complications following the surgery. Further workup with the oncology department was performed 2 weeks after surgery to determine if radiation or chemotherapy would be necessary. The foreign tissue was deemed completely gone, and no radiation or chemotherapy was needed.
Discussion
SPEN of the pancreas is a rare neoplasm composed of monomorphic cells forming solid and pseudopapillary structures. 1 The tumor is characterized by a well-encapsulated mass with varying amounts of necrosis, hemorrhage, and cystic change. 3 The tumor can have an atypical appearance, such as metastasis, ductal obstruction, parenchymal and extracapsular invasion, simulation of islet cell tumor, and intratumoral calcification. 3 Lesions can become very large at diagnosis, with a median size of 8.0 cm. 4
This type of exocrine pancreatic tumor occurs predominantly in women in their second and third decades of life, but some tumors have been seen in males as well. 3 Most patients are asymptomatic at diagnosis. Patients may occasionally present with a gradually enlarging abdominal mass or vague abdominal pain. 4 Usually, the neoplasms are found incidentally on routine physical examinations, occasionally after abdominal trauma.
The majority of SPENs are benign; however, 15% have been found to be malignant. 1 Common metastatic sites include regional lymph nodes and the liver, peritoneum, and greater omentum. Prognosis for SPEN is rather good, if complete removal is performed. After complete removal, >95% of patients remain disease free.4,5 When the tumor is larger, more extensive resection is required, which can lead to pancreaticoduodenectomies, distal pancreatectomies, and distal pancreatomy with omentectomy or transverse colectomy. 6 Even in cases such as these with extensive resections, most patients were living disease free at their follow-up. 6 Even if metastasis is present, long periods of remission have been recorded after resection.4,5 Only a few patients have been reported to succumb to a metastasizing SPEN.7,8 In reported cases of death related to SPEN, patients have been >40 years old, and their mortality was suspected to be due to widespread abdominal metastases.7,8
The best method for detecting and diagnosing SPEN include a combination of sonography, MRI, and computed tomography. 9 In the case presented, sonography was a key noninvasive study used to initially detect the presence of the mass, while MRI verified the sonographic findings and aided in pinpointing the origin of the mass.
This case study highlights the importance of incidental findings and the importance that sonography plays in routine screening. The American College of Radiology’s appropriateness criteria strongly support the use of multi- or triphasic computed tomography imaging for an accurate diagnosis of pancreatic tumors. 10 This case demonstrates the important diagnostic information that is contributed with a sonogram of the pancreas. This case also provides a classic demonstration of a SPEN tumor and could be a helpful reference for future suspected cases of a SPEN tumor of the pancreas.
Conclusion
This case showcases how diagnostic imaging, especially sonography, has the ability to contribute significant imaging information in the detection, characterization, and classification of SPEN. The origin of this mass was unable to be definitively determined sonographically; therefore, further studies were ordered to evaluate the mass. The MRI confirmed the sonographic findings and distinguished that the mass in question was arising from the pancreatic tail and had all the characteristics of SPEN. This case study demonstrates low-level evidence that sonography can provide incidental imaging information that can lead to the detection of SPEN.
Footnotes
Acknowledgements
I thank Anne Trent, RDMS, RVT, Michelle Klenklen, RDMS, RVT, and Mark Tinsley, RDMS, RVT, for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.