
Abstract
A renal transplant recipient had a urinary fistula repaired and a double-pigtail ureteral stent left and later surgically removed. At this same time, an open biopsy was performed and closed with chromic 2-0 catgut sutures. A sonogram revealed an artifactual image that was interpreted as a fragmented piece of the stent that was left in the patient. An exploratory surgery performed, however, was unremarkable, and the renal incision was again closed with chromic 2-0 catgut sutures. A repeated sonogram demonstrated the previous artifact, which raised the suspicion that this appearance should be attributed to the chromic 2-0 catgut sutures. An experiment using a model of coupling gel and chromic 2-0 catgut sutures demonstrated artifacts that matched those seen during sonography of this particular renal allograft. This sonographic artifactual appearance may be seen in hypostenic patients with a high-frequency transducer centered over chromic 2-0 catgut sutures.
The American College of Radiology recommends diagnostic sonography as the first choice for imaging and determining dysfunction of a renal allograft. 1 Sonography of a transplanted kidney has the potential to demonstrate a more detailed image, compared with the native kidney, as the transplant is usually located more superficially. In addition, with patients who have a lean body mass, higher frequency transducers can be employed, 2 thereby increasing overall resolution. This case study discusses an unusual finding due to a sonogram of a renal allograft, initially interpreted as containing a fragmented piece of a double-pigtail ureteral stent. 3
Case Report
A 50-year-old man with a hypostenic body habitus and chronic renal failure, secondary to unknown kidney disease, received a cadaveric renal transplant. His clinical history included systemic hypertension but no history of diabetes mellitus, urinary tract infection, or analgesic abuse. There were two of six human leukocyte antigen matches (both in DR), and cold ischemia time was 14 hours and 30 minutes. Maintenance immunosuppression consisted of steroids, tacrolimus, and mycophenolate mofetil. Eleven days after transplantation, he was discharged with serum creatinine equal to 2.1 mg/dL. Five days later, the patient was admitted showing fever, urinary tract infection, and a significant rise in serum creatinine (2.8 mg/dL). A urinary fistula was seen by scintigraphy. Using an open surgical procedure, ureteral necrosis was repaired by ureteral reimplantation. A double-pigtail ureteral stent was left in place. In both surgical procedures (graft implantation and ureteral reimplantation), open biopsies were performed using the wedge excision technique, and the wounds were then closed with chrome 2-0 catgut stitches. Chrome 2-0 catgut sutures are an absorbable biological suture made by twisting together strands of purified collagen, made from bovine intestines. 4 This suture material is treated with chromic acid salts, and therefore this chromic treatment increases the holding time twofold compared with untreated catgut sutures. 4
Postsurgically, the patient’s condition improved, so the ureteral stent was removed. The patient was subsequently discharged 32 days after the second hospitalization. Unfortunately, this patient was readmitted with increased creatinine levels (11.1 mg/dL) and sepsis due to Escherichia coli 21 days later. He was treated with meropenem followed by cefepime. A sonogram was completed using a 3.5 curved linear array and 7.0-MHz linear array transducers (Siemens Sonoline G40; Siemens, Erlangen, Germany). The sonographic images revealed a set of parallel echogenic lines with an anechoic center (Figure 1), in renal parenchyma, resembling a tubular structure. The sonographic artifactual features on the image were interpreted as nonbiological material that could represent the migration and rupture of the double-pigtail stent. Furthermore, it was suggested that a fragmented piece left after surgical withdrawal could have contributed to the patient’s infection. On the basis of these hypotheses, the patient was taken back to the operating room for an exploratory surgery. The findings were unremarkable, and the renal incision was closed with chrome 2-0 catgut sutures. A repeated sonography with a linear transducer of 7.0 MHz demonstrated the same artifactual image as seen previously but much smaller in length than previously noted. The results of the surgery thus led to confusion about the causes of the artifactual image but did raise the suspicion that the artifact could have been produced by the chromic catgut suture itself.
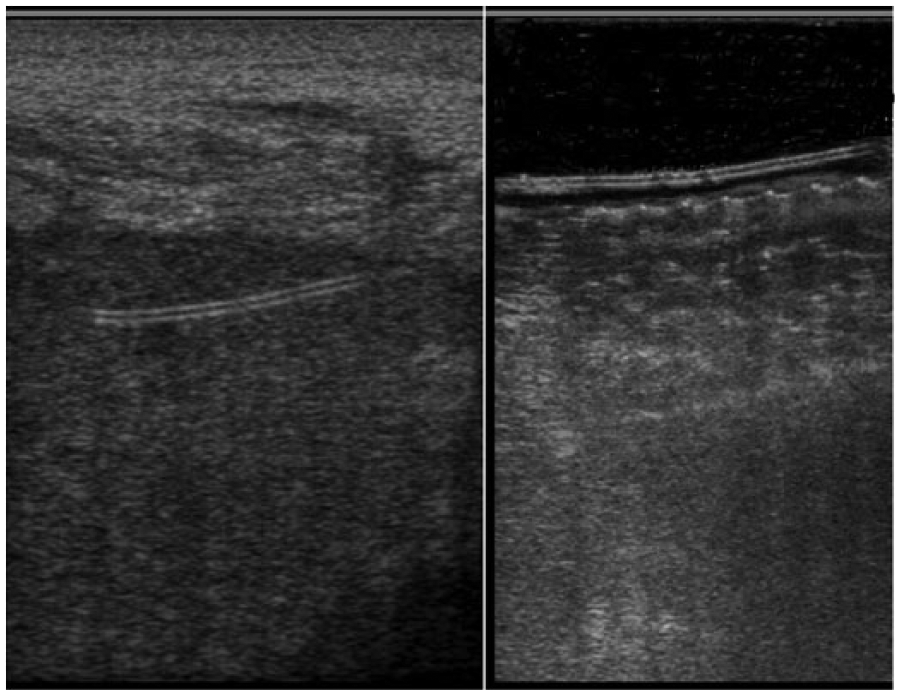
Sonographic chromic 2-0 catgut suture appearance. Sonography conducted with a 7.0-MHz linear transducer. Left: two parallel hyperechogenic lines border an anechoic center, resembling a tubular artifactual image, within the allograft parenchyma. Right: the phantom with chromic 2-0 catgut sutures immersed in coupling gel produced a similar artifactual image, as seen in the allograft parenchyma.
To verify this hypothesis, an in vitro experiment was undertaken, using chromic 2-0 catgut sutures, immersed in an open container filled with coupling gel. The perpendicular insonation of chromic 2-0 catgut suture, with a linear transducer of 7.0 MHz, demonstrated the same artifact, as had been seen within the renal allograft’s parenchyma (Figure 1). Thereafter, the patient’s condition improved, and therefore he was discharged 27 days after the second hospitalization, with a serum creatinine of 1.75 mg/dL.
Discussion
Diagnostic sonography associated with or without color Doppler is a relatively cheap, noninvasive, and nonnephrotoxic modality that may be used for diagnostic and surveillance purposes early on, in the posttransplant period, thus establishing a baseline for follow-up imaging. Occasionally, as in this case, unusual or unexpected findings can result due to sonographic artifacts. The patient had a ureteral stent inserted as part of the treatment for a urinary fistula, and later the stent was retrieved. Migration and fragmentation of stents are well-known complications associated with stent insertion.3,5 The tubular artifact image with two linear hyperechoic borders and an anechoic center was correctly interpreted as nonbiological material but was misdiagnosed as a fragmented piece of a double-pigtail stent that was left postsurgically. The persistence of the image and the appearance of other images containing the artifact, after surgery, aroused the suspicion that the chromic 2-0 catgut suture was the source of the artifact. The in vitro phantom experiment confirmed the hypothesis that the artifact represented the suture material. Although initially surprising that a solid structure, such as the chromic 2-0 catgut, was depicted as a tubular structure on the sonographic image, this kind of artifactual finding has been described as a pitfall that can occur during the sonographic image process. 6 This type of artifact can occur as follows. First, when the soundwave strikes an acoustic boundary, between media with different impedances, part of the energy is transmitted across the boundary, while some is reflected and yields an image. In this case different impedances between renal parenchyma and catgut yield the first echogenic line. Second, when the soundwave travels through the chromic 2-0 catgut suture and insonates the whole catgut homogeneous medium thickness, without different impedances, no reflection is produced, and therefore an anechoic region within the image is created. The second echogenic line is created in a similar way to the first one as the sound exits the catgut.
Sonography has been shown to accurately demonstrate radiolucent soft tissue foreign bodies, such as wood splinter, glass, metal, and plastic, using a high-frequency (7.5 MHz or higher) linear array transducer. 7 Moreover, the sonographic diagnosis of a gastric foreign body in a child has also been reported. 8 Reviewing this case study in conjunction with these other reported artifacts that were captured on a sonogram from foreign material, it would seem that the visualization of the catgut was plausible. Likely, this artifact could also be attributed to the combination of the body habitus of the patient and the use of a high-frequency transducer over the site. The result was an examination with a higher than usual degree of resolution that captured a sonographic representation of the chromic 2-0 catgut suture. A Medline and PubMed search was conducted to locate any previously published case reports of this type of artifact with sonography. Accordingly, the literature search did not provide any further evidence of an artifact associated with chromic 2-0 catgut suture seen in an allograft parenchyma.
This case study highlights an unusual example of a misleading sonographic artifact that contributed to unnecessary treatments for this particular patient. Since the surgical wedge biopsy can be closed using 2-0 chrome catgut sutures, it may be important to be aware of the sonographic artifact presentation. Likely, this artifact may only be seen in combination with chromic 2-0 catgut sutures imaged with a 7.0-MHz linear transducer in a patient with a hypostenic body habitus.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This case report is made possible through the support from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ).