
Abstract
Page kidney phenomenon occurs due to external compression of a kidney by either subcapsular or perinephric hematoma, tumor, lymphocele, or urinoma. This article describes a case of reversed diastolic arterial flow on Doppler insonation in a Page kidney due to external compression as a consequence of native kidney biopsy-induced perinephric hematoma. Reversed diastolic arterial flow has already been reported in Page kidney in renal allografts; however, we are not aware of any report of such a finding in a native kidney. This report highlights the importance of being aware of the possible occurrence of the reversion of the diastolic flow in Doppler sonography in Page kidney, even though it is rare. Moreover, this case illustrates the short but severe impact of Page kidney on renal function and suggests that a conservative approach is an effective treatment option even in a moderate to severe perinephric hematoma.
Page kidney phenomenon occurs due to external compression of a kidney by either subcapsular or perinephric hematoma, tumor, lymphocele, or urinoma. 1 The condition is usually associated with the development of renin-dependent hypertension. This phenomenon was first described in 1939 by Dr. Irwin Page in an experiment whereby he compressed canine kidneys by wrapping them in cellophane and induced hypertension. 2 Numerous case reports of Page kidney have previously appeared in otherwise healthy young athletic men with a history of sports-related trauma who presented a few years after the injury with new-onset hypertension. 3 In the more recent reports, the etiology has been attributed to complications of iatrogenic procedures, particularly subcapsular hematoma following renal transplant biopsies. 1 This case study describes the case of a Page kidney as a consequence of native kidney biopsy-induced perinephric hematoma. This report highlights the importance of being aware of the possible occurrence of the reversion of the diastolic flow in Doppler sonography in a Page kidney, even though it is rare.
Case Report
A 23-year-old man with no particular medical history presented to the hospital with a two-week history of lower extremity edema and weight gain of more than 10 kg. His physical examination was normal except for the edema of the lower extremities and a blood pressure of 140/90 mm Hg.
The laboratory investigation yielded some relevant abnormal findings: serum creatinine 1.40 mg/dL (reference range [RR], 0.5–1.1 mg/dL), serum albumin 1.8 g/dL (RR, 3.4–5.4 g/dL), and total cholesterol 447 mg/dL (RR, <200 mg/dL). Urinary protein excretion was 2.5 g/g creatinine (RR, <0.20), and microhematuria was present. The coagulation profile was normal.
Workup for secondary or systemic causes of the patient’s renal disease was performed, revealing no antinuclear antibodies and antineutrophilic cytoplasmic antibodies, normal complement and rheumatoid factor levels, and negative serology for hepatitis B and C and human immunodeficiency virus.
On the sonogram, the right kidney measured 12.1 cm, and the left kidney measured 12.3 cm. Both showed normal echogenicity and no evidence of renal vein thrombosis (RVT), hydronephrosis, or perinephric fluid collection.
The patient’s blood pressure was controlled with hydralazine. He was also started on spironolactone and furosemide to help minimize edema. A left renal biopsy was performed under sonography guidance with an automatic biopsy gun. The patient was discharged one day later.
The patient was readmitted with back pain, hypertension (180 × 100 mm Hg), and increased creatinine levels (2.4 mg/dL) 10 days later. The biopsy results were consistent with minimal change in disease. The patient was initially treated with intravenous methylprednisone and then switched to oral prednisone.
An additional renal sonogram and color Doppler (CDUS) study revealed a large perinephric hematoma of 197.9 cm3 (Figure 1), reversed diastolic flow in all branches of the intrarenal and extrarenal arteries vasculature, and no flow in intrarenal veins (Figure 2). In addition, flow within the main renal vein was not shown in a convincing way (Figure 3). This spectral tracing suggested the diagnosis of an intrarenal vein thrombosis, which prompted an immediate initiation of anticoagulant therapy with intravenous administration of low-molecular-weight heparin (enoxaparin sodium). A marked worsening in the patient’s condition was evident within one day, with a decrease in hematocrit from 34.8% to 27.1% requiring a blood transfusion. Anticoagulation was discontinued. A repeated CDUS showed enlargement of the hematoma (293.1 cm3) (Figure 1) and continued reversed diastolic flow in the arteries (Figure 4). Five days later, another CDUS examination revealed persistent hematoma and normalization of spectral tracing of arterial blood flow (Figure 4). Once the patient’s clinical condition stabilized, no further measure was taken. Based on the patient’s recovery of renal perfusion, despite the withdrawal of anticoagulation, the diagnosis was amended from RVT to Page kidney. After that, since the patient’s condition had improved, he was discharged nine days after the second hospitalization. Two months after biopsy, a repeated CDUS revealed a reduction in hematoma size (145.0 cm3) and normal diastolic flow. The patient has continued with routine follow-up medical visits for over one year. In the meantime, prednisone was shifted to cyclosporine because of steroid dependence. The level of serum creatinine remains at 1.2 mg/dL, and urinalysis reveals no abnormality. The patient did not return for CDUS examination.
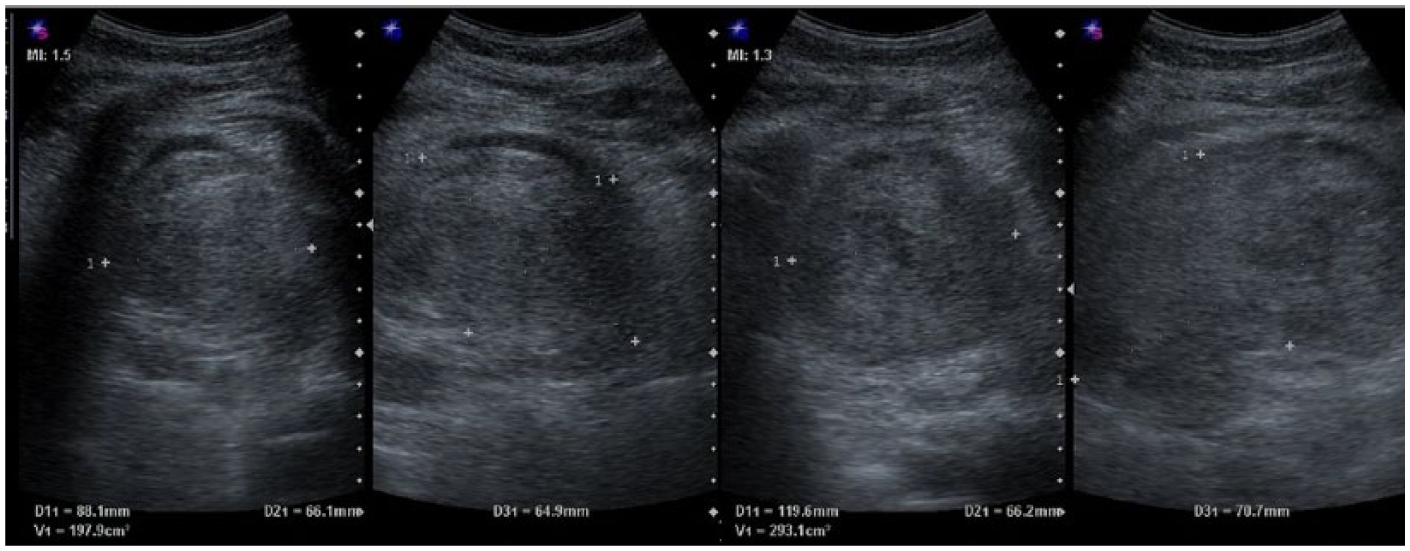
Left: a hematoma of 197.9 cm3 surrounding the posterior aspect of the left kidney 10 days after biopsy when reversed diastolic flow was first seen. Right: the repeated ultrasound, two days later after starting anticoagulation showed enlargement of the hematoma to 293.1 cm3.
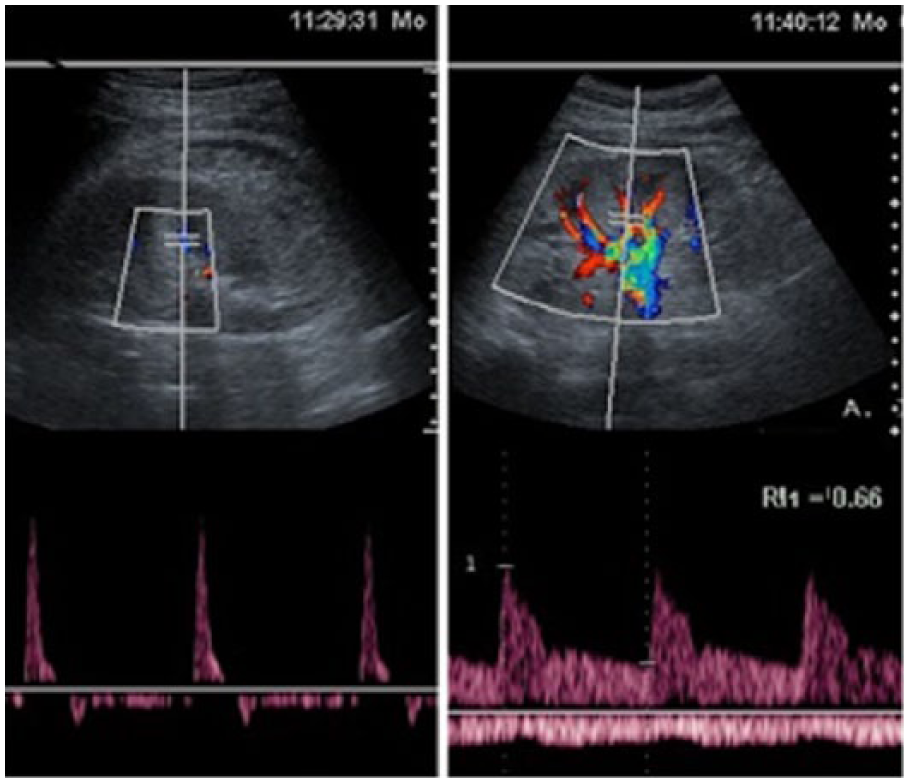
Left: Doppler of the left kidney, 10 days after biopsy, revealed paucity of vessels and spectral tracing with diastolic flow reversion. Right: the insonation of the right kidney shows normal arterial waveform and resistance index.
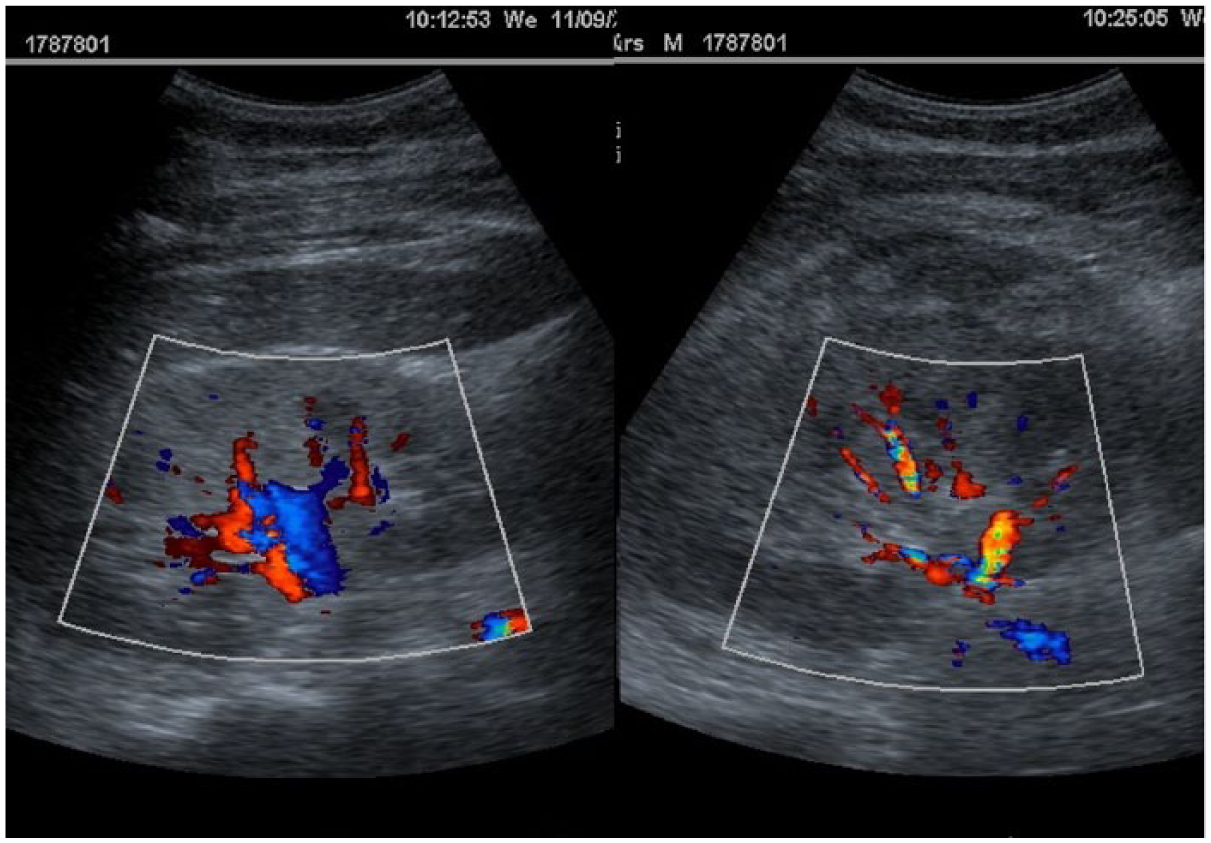
Left: color Doppler shows clearly the renal artery and vein of the right kidney. Right: color Doppler shows unequivocally the renal artery but not the vein of left kidney.
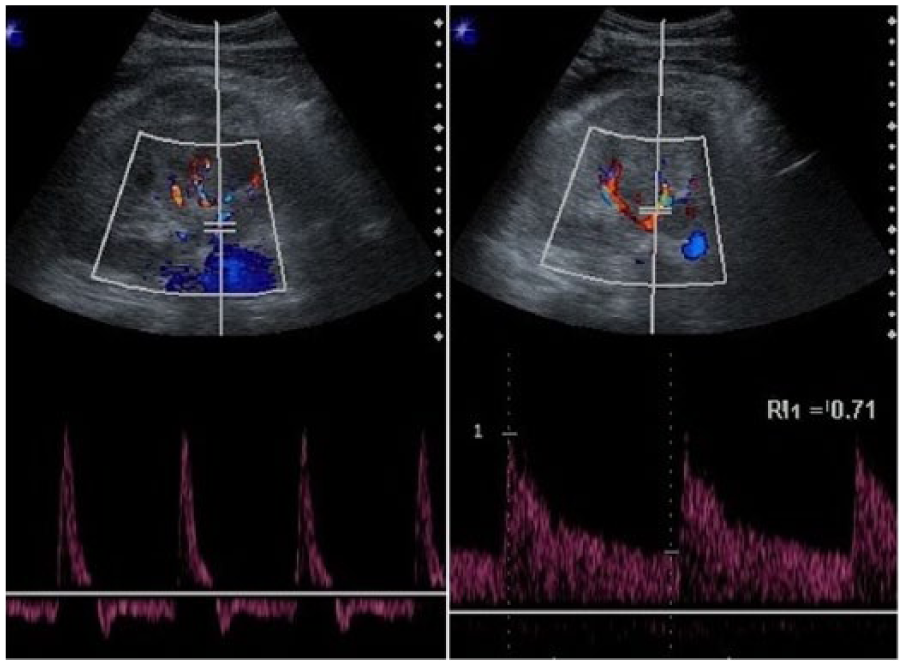
Doppler findings in left kidney after biopsy: 12 days later (left) revealed no change in relation to findings obtained two days before. On the other hand, 17 days later (right), abnormal spectral waveform and reversed diastolic flow were no longer present.
The sonogram was performed using a Sonoline 40 (Siemens, Erlangen, Germany) instrument with a 3.5-MHz transducer. The biopsy was performed using a 16-gauge automated, spring-loaded core biopsy device (Tru-cut; Baxter, CA, USA) under real-time sonographic guidance.
Discussion
In addition to trauma, etiologies for perinephric hematomas are numerous and include a percutaneous renal biopsy. Percutaneous core biopsy remains the gold standard for the assessment of adults’ nephrotic syndrome, but it carries the limitations of bleeding complications that can result in a perirenal or subcapsular hematoma. In this patient, the nephrotic syndrome was diagnosed based on laboratory (hypoalbuminemia, hypercholesterolemia, and proteinuria) and clinical findings (edema). Page kidney generally refers to the development of hypertension due to the effects of external compression of the kidney, among other causes, by either acute or chronic hematoma. The resulting hypertension of Page kidney is due to activation of the renin-angiotensin-aldosterone system. In the case of a single kidney or renal allograft, acute renal failure may also develop in Page kidney. 4
The kidney is a primary retroperitoneal organ that is surrounded by two envelopes. The first is the fat-filled perirenal space, confined anteriorly by the anterior renal fascia (Gerota fascia or fascia of Toldt) and posteriorly by the posterior renal fascia (Zuckerkandl fascia) that encloses the kidney on all sides except inferiorly, so that perirenal fluid collections can spread downward. The perirenal space is a large space, and only a large hematoma would yield enough pressure to compress the kidney. The second envelope is the renal capsule, a thin layer of fibrous connective tissue. The potential space between the renal capsule and underlying parenchyma allows only a small amount of blood to accumulate before yielding enough pressure to compress the kidney.
This patient presented a large perinephric hematoma, developed hypertension, and acute renal failure even though he has both kidneys. His acute renal failure was presumably due to a decreased perfusion of the kidney as a result of pressure exerted by the perinephric hematoma without compensation from the contralateral kidney, probably due to the underlying disease. Moreover, in some cases, the nephrotic syndrome can be accompanied by acute renal failure. 5 It is noteworthy that, based on the reversed diastolic artery flow, the patient’s condition was initially misdiagnosed as a vein thrombosis, which prompted the initiation of anticoagulation.
The worsening of the patient’s hematocrit and enlargement of the hematoma led to a cessation of the anticoagulation. Curiously, five days later, although the hematoma remained, pressure was likely relieved because of the restoration of blood flow, recovery of renal function, and normalization of spectral tracing of the renal arteries. There are two reasons why the clinical condition improved. First, perinephric hematoma exerts less pressure on the kidney than a subcapsular hematoma. Second, it is also possible that some amount of the hematoma spread downward through the inferior opening of the perirenal space, which would help relieve the pressure.
Although reversed diastolic arterial flow is a well-known indication of venous thrombosis in a transplanted kidney,6,7 this sign is unreliable in RVT of native kidneys. 8 One reason is that native kidneys, unlike renal allografts, are able to form capsular venous anastomoses in as little as 24 hours and often within the first two weeks after RVT. 9 This case was misdiagnosed as RVT 10 days after the renal biopsy when the collateralization should have taken place and obviated the diagnosis; however, the uncertainty about the final reason for the observed pathologic flow pattern and the concern of the devastating outcome of the RVT led to initiating anticoagulation.
Reversed diastolic arterial flow has already been reported in Page kidney following biopsy 6 and percutaneous nephrostomy 7 in renal allografts; however, this is likely a unique report of such a finding in the same condition in a native kidney.
Treatment goals should be a reversal of systemic hypertension and preservation of renal function. This was achieved in this patient using conservative medical therapy, awaiting spontaneous resolution of the hematoma, which resulted in significant clinical improvement that was in line with other reports.10,11 This may be a demonstration of a temporary Page kidney with rapid reversal of the hypertensive effect.
Based on this case, it would be advised that the finding of reversed arterial diastolic flow in a native kidney could suggest the likelihood of internal or external compression of the kidney more than RVT, particularly if a causal factor for compression is identified. Therefore, it is important to know that the finding of reversed diastolic flow in a native kidney may not determine the same strength of association with RVT as in a renal allograft, as highlighted by Platt et al. 8
Moreover, this case illustrates the short but severe impact of Page kidney on renal function and suggests that a conservative approach could be an effective treatment option even in a moderate to severe perinephric hematoma.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This case report is made possible through the support from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ).