
Abstract
Abdominal pain in women of reproductive age is a frequently encountered chief complaint in the emergency department. Adnexal torsion is a time-sensitive diagnosis that is essential for emergency physicians to consider in the initial differential diagnosis. Bedside sonography can be used to assist the clinician in the detection of adnexal masses placing the patient at risk for torsion. Lipoleiomyomas are uncommon, benign neoplasms consisting of variable portions of mature lipocytes, smooth muscle, or fibrous tissue. Very few cases have been reported, with no cases previously reported by emergency physicians using bedside ultrasound. A case is presented of a middle-aged woman who presented to the emergency department with acute lower abdominal pain. At the time of the initial history and physical examination, bedside screening sonogram was performed, which allowed rapid diagnosis of a large, heterogeneous, relatively avascular adnexal mass that was later identified as a lipoleiomyoma, a rare adnexal neoplasm, that resulted in adnexal torsion.
Abdominal pain is a frequently seen chief complaint in the emergency department (ED). Adnexal torsion is a time-sensitive diagnosis that is essential to consider in reproductive-age females to avoid the potential morbidity of ovarian necrosis and possible diminished future fertility. Bedside screening sonograms can be used to rapidly evaluate undifferentiated abdominal pain and potentially identify adnexal masses that may place patients at higher risk of adnexal torsion. In addition, bedside screening sonogram is a valuable tool to rapidly evaluate other diagnostic considerations, assisting in shortening and revising a broad differential diagnosis, potentially limiting downstream evaluation, and improving patient care through earlier diagnosis. A case of acute abdominal pain in a female patient is presented that makes the use of sonography, at the point of care, that revealed a large adnexal mass, eventually identified as a lipoleiomyoma. Lipoleiomyomas are very rare, benign neoplasms consisting of variable portions of mature lipocytes, smooth muscle, and/or fibrous tissue. Most often, these tumors are found within the uterine body, although they have also been documented in other locations such as the cervix, ovary, or retroperitoneal space. 1
Case Report
A 46-year-old woman presented to the ED with acute-onset left lower quadrant abdominal pain that began approximately one hour prior to arrival with radiation to the back and left lower extremity. Her medical history was notable for ovarian cysts that had resolved in the past without intervention as well as chronic back pain secondary to degenerative disc disease. The patient stated that her current pain was different from the chronic back pain she had experienced in the past. The patient denied vaginal bleeding, dysuria, hematuria, bowel or bladder incontinence, or neurologic symptoms. She reported that her last menstrual period was approximately three weeks prior to evaluation.
On physical examination, the patient appeared uncomfortable and was in moderate distress secondary to pain. Her initial vital signs revealed a blood pressure of 158/90 mm Hg and a pulse of 91 without evidence of fever. Her abdomen was soft but markedly tender to palpation in both the right and left lower quadrant with voluntary guarding and rebound present on the left. The remainder of the physical examination was within normal limits. Laboratory findings were largely unremarkable and included a negative serum pregnancy test. The emergency physician performed a bedside screening sonogram during the initial history and physical examination. During the screening sonogram, a large, solid, heterogeneous mass was identified in the right lower quadrant area (Figures 1 –3) measuring roughly 10 cm in all dimensions, and no blood flow could be identified by color Doppler analysis. It should be noted that when evaluating low blood flow states, such as torsion, the color and Doppler scale settings should be placed as low as possible to differentiate low flow and absent flow states. In Figure 2, the color scale is at a rather wide setting from −18 to +18 cm/s. Typical settings to more completely evaluate torsion should be as low as possible, possibly down to ±1 to 2 cm/s depending on the capabilities of the ultrasound machine. In this case, the screening sonogram was followed by a consultative sonographer study where the lowest possible settings were used.
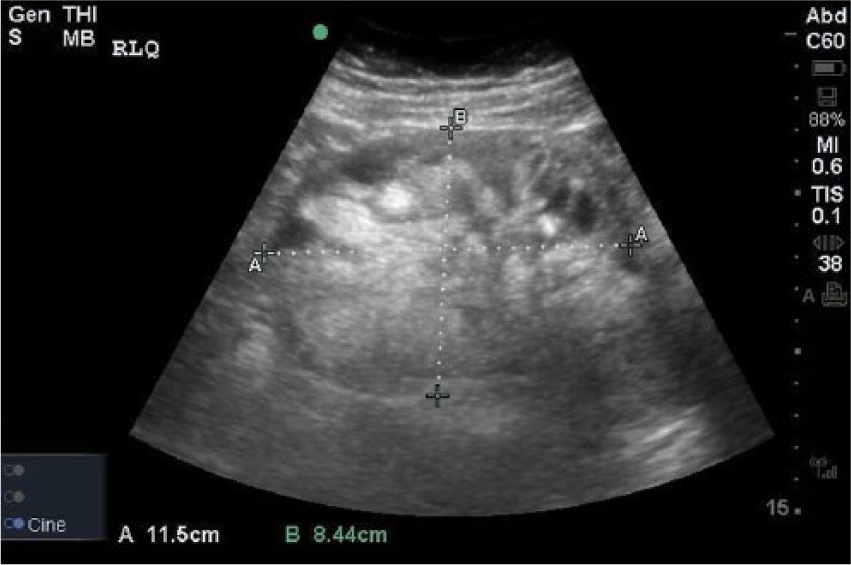
Sagittal image from the bedside ultrasound demonstrating the right lower quadrant mass.
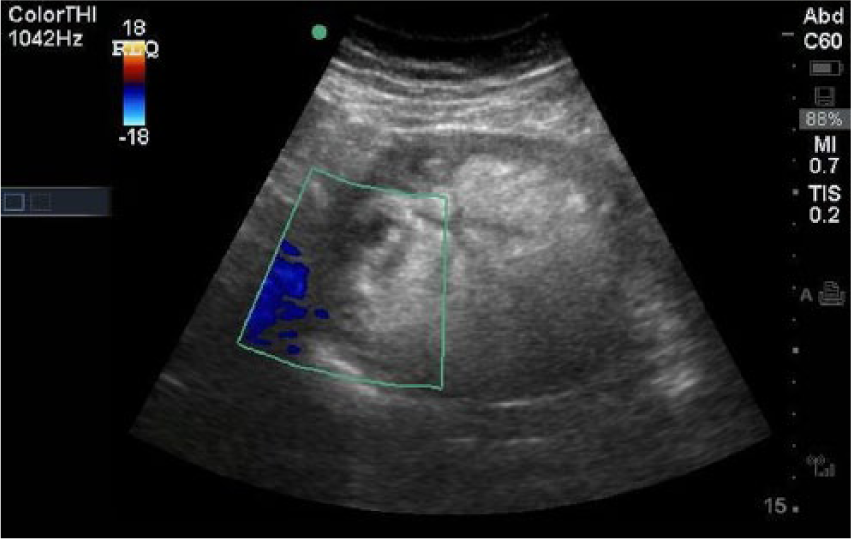
Mass located in the right lower quadrant on emergency bedside ultrasound.
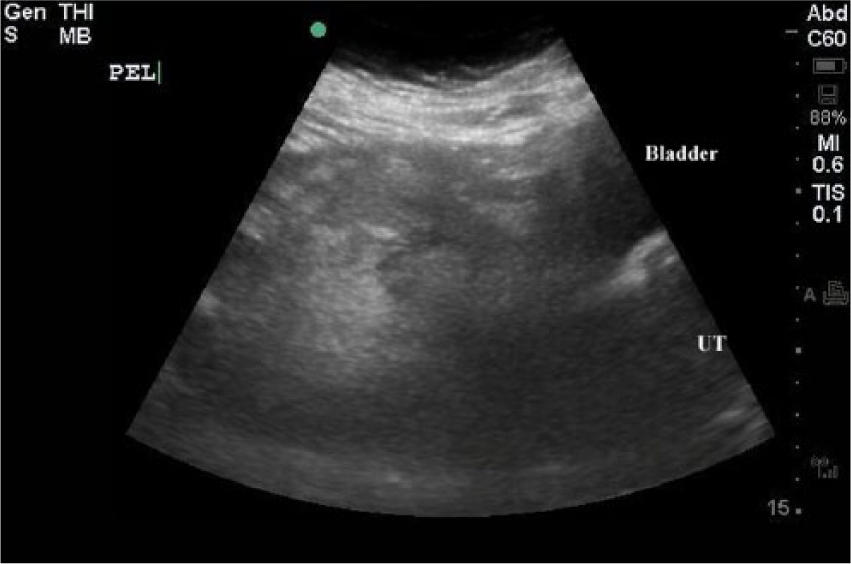
Sagittal image of the pelvis noting location of the right lower quadrant mass.
The sonographer study was performed in the radiology department confirming the presence of a large heterogeneous mass intimately associated with the right ovary and findings concerning for torsion of the right ovary. The obstetrics and gynecology service was subsequently consulted, and upon discussing the diagnosis and potential treatment options, the patient expressed a desire to undergo hysterectomy as she no longer desired fertility and had suffered with chronic pelvic pain in the past. The patient was subsequently taken to the operating room for exploratory laparotomy and total abdominal hysterectomy and bilateral salpingo-oophorectomy. A large, solid mass approximately 13 cm in diameter originating from the right adnexa was excised and sent to pathology. The final pathologic report identified the mass arising from near the right ovary as a lipoleiomyoma with findings consistent with adnexal torsion. The patient did well and had an uneventful postoperative course.
Discussion
On every shift, emergency physicians evaluate patients with abdominal pain. Although the differential diagnosis is broad, the clinician must include adnexal torsion in the list of diagnostic possibilities when evaluating a female patient presenting with lower quadrant abdominal pain. Adnexal torsion is a gynecologic emergency that occurs when the ovary or fallopian tube twists upon its vascular pedicle, leading to occlusion of the adnexal blood supply. Failure to recognize adnexal torsion or a delay in surgical intervention can lead to loss of the ovary secondary to ischemic injury and necrosis. The presence of an ovarian cyst or mass lesion increases the weight of the adnexal structures and is a major risk factor for the development of torsion.2,3
Sonography is the primary imaging modality to make the diagnosis of adnexal torsion and when deployed appropriately and early in the evaluation of a patient with abdominopelvic pain, it can also help the physician rapidly narrow the differential diagnosis. To effectively use bedside sonography, emergency physicians should be familiar with sonographic findings suggestive of torsion. The primary findings in ovarian torsion include ovarian enlargement and abnormalities of ovarian blood flow by spectral Doppler analysis. Ovarian enlargement and adnexal masses are common, but these findings alone have poor sensitivity for the diagnosis. Similarly, blood flow by color and spectral Doppler may be decreased, be absent, or exhibit high-resistance flow patterns, but the presence of blood flow does not exclude the diagnosis.2–4
When evaluating the adnexa with sonography, the clinician should also evaluate for the presence of the “whirlpool” sign, which has been described as the visualization of hypoechoic vessels of the ovarian artery and vein wrapping around the central axis while moving the probe to and fro along the twisted pedicle. 5 Vijayaraghavan 5 reported that in a prospective study of women with suspected adnexal torsion, all 20 patients with the presence of a whirlpool sign had surgically proven ovarian torsion. Unfortunately, it is important to remember that no single sonographic finding can reliably exclude adnexal torsion, and the emergency physician must be vigilant to aggressively pursue this diagnosis even with a nondiagnostic sonogram when there is high clinical suspicion.2,3
While most masses leading to torsion are benign cystic lesions, more complex tumors have also been associated with torsion. 6 The patient described in this case presented with a lipoleiomyoma, an exceedingly rare benign encapsulated pelvic tumor composed of adipose and smooth muscle with a reported incidence of only 0.03% to 0.2%. 7 This type of tumor has not been previously described in the medical literature as leading to adnexal torsion. Most previously described lipoleiomyomas have been in the uterus; however, there have been case reports of lipoleiomyomas diagnosed in the broad ligament, peritoneum, and ovary.1,8 Due to its rarity, the typical presentation of this tumor type is not well described, but in symptomatic patients, it has been associated with pelvic pain, increasing abdominal girth mimicking ovarian cancer, or dysfunctional uterine bleeding. 6 Lipoleiomyomas frequently grow to sizes greater than 10 cm, 5 which would place an adnexal lipoleiomyoma, such as the one in this case, at high risk for adnexal torsion.
Sonographically, lipoleiomyomas have been described as heterogeneous, largely echogenic masses with a thin, hypoechoic rim, exhibiting posterior acoustic enhancement and poor vascularity. The sonographic findings of a large, heterogeneous mass with areas of echogenic fatty infiltration should raise the suspicion of this diagnosis, but the differential includes many other gynecologic tumors, specifically teratoma with or without malignant degeneration, but also including lipoma, liposarcoma, angiomyolipoma, fibromyolipoma, and myelolipoma. 9
In summary, this case study of an ovarian lipoleiomyoma, an exceedingly rare neoplasm of the female pelvis, was quickly identified at the bedside by an emergency physician. The lipoleiomyoma in this case led to ovarian torsion. Identifying this mass immediately at the bedside was useful in narrowing the differential diagnosis and likely improved the patient’s outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.