
Abstract
This case study provides a report on a patient who had a segmental renal allograft infarction. The cause of this infarction within the segmental vessels was theorized to be due to prolonged warm ischemia within the organ donor. The area of infarction was visualized by the use of contrast-enhanced ultrasound (CEUS). This report raises the question as to whether routine sonographic imaging can demonstrated the sequence of infarction within a fresh renal allograft, as is routinely noted in native kidneys. This report highlights the importance of taking the segmental infarction into consideration when approaching the renal allograft recipient. CEUS could provide an important clinical application for the diagnosis of renal allograft infarctions and avoid more invasive procedures. Knowledge of the lack of sequence of sonographic changes in renal allograft infarction helps in assessing the function and outcomes of renal allograft recipients.
Introduction
Renal allografts has been established as the treatment of patients with end-stage renal disease and is performed in many transplant centers worldwide. However, a wide variety of surgical complications may occur, including renal infarction. Renal infarction results from a renal artery embolism (ischemic) or renal vein thrombosis (hemorrhagic) interruption of the normal blood supply to the kidney. It is an easily missed disease mainly due to its nonspecific presentations 1 and potential for misdiagnosis. 2 Renal infarction may involve the entire kidney or small areas of the cortex or medulla. In renal allografts, segmental infarction typically occurs in the early postoperative period, and a prompt diagnosis is difficult to obtain. 3 Because of its nonspecific presentations, it is difficult to define the incidence clinically. Unfortunately, the outcome of late or delayed diagnosis can have a negative outcome because it can result in complete loss of renal function in a native kidney, 4 and it also can compromise the long-term function of an allograft. 3 This case study illustrates this pathology in a patient who developed a segmental renal infarction and it may be attributed to prolonged warm ischemia within the donor patient. This report highlights the importance of taking the segmental infarction into consideration when approaching the renal allograft recipient and the efficacy of conservative management. In addition, this case demonstrates the lack of documenting a series of sonographic changes seen in the native kidney.
Case report
A 22-year-old female with end-stage renal disease secondary to immunoglobulin A (IgA) neuropathy, also known as Berger’s disease, underwent a live donor renal transplant from a matched living donor. The left kidney was removed by a hand-assisted laparoscopic technique. Warm ischemia time in the donor, from renal artery occlusion until flushing of the organ was 7 minutes. The whole operation time was 138 minutes. The patient received immunosuppression with tacrolimus, mycophenolate mofetil, and steroids. Her creatinine level did not decease immediately after transplantation, but fell slowly and achieved a nadir level of 1.8 mg/dl by day 4. As part of the patient’s diagnostic work-up, a color Doppler ultrasound (CDUS) using Superb Microvascular Image® (SMI) (Toshiba, Tokyo, Japan) was performed. It revealed a poorly marginated, mainly sonolucent, cortical area containing bright echoes in the corticomedullary transition and without perfusion (Figure 1). To better depict this area, a contrast-enhanced ultrasound (CEUS) was performed with 2.4 ml of Sonovue® (Bracco Int, Milan, Italy). It showed a clearly defined, nonenhanced wedge-shaped area in a pattern consistent with renal artery segmentation at the lower half of the graft (Figure 1). The recognition of a segmental infarct with this renal allograft prompted the present report. No additional diagnostic measures were taken. On postoperative day 14, lactate dehydrogenase (LDH) activity significantly increased from 302 (baseline) to 720 IU/L and decreased to 218 IU/L 2 weeks later (reference range, 135–225 IU/L). At discharge on day 23, graft function was stable with a serum creatinine of 1.4 mg/dl. The patient was readmitted with diarrhea, vomiting, and raised creatinine level (2.4 mg/dl) 1 week later. Since the tacrolimus blood level rose from 3.7 ng/ml (day 6) to 14.0 ng/ml (day 31), the tacrolimus dosage was reduced. As a diagnostic follow-up, 27 days later CDUS was repeated using SMI demonstrated that the infarction was almost anechoic in presentation (Figure 2). Thereafter, the patient’s situation improved with a decrease in serum creatinine level (1.3 mg/dl) associated with a reduction in the tacrolimus blood level (7.0 ng/ml). The patient was then discharged, and at follow-up at 104 days, the graft was still functioning with creatinine levels higher than expected (1.3 mg/dl) and unchanged infarction image (Figure 2).
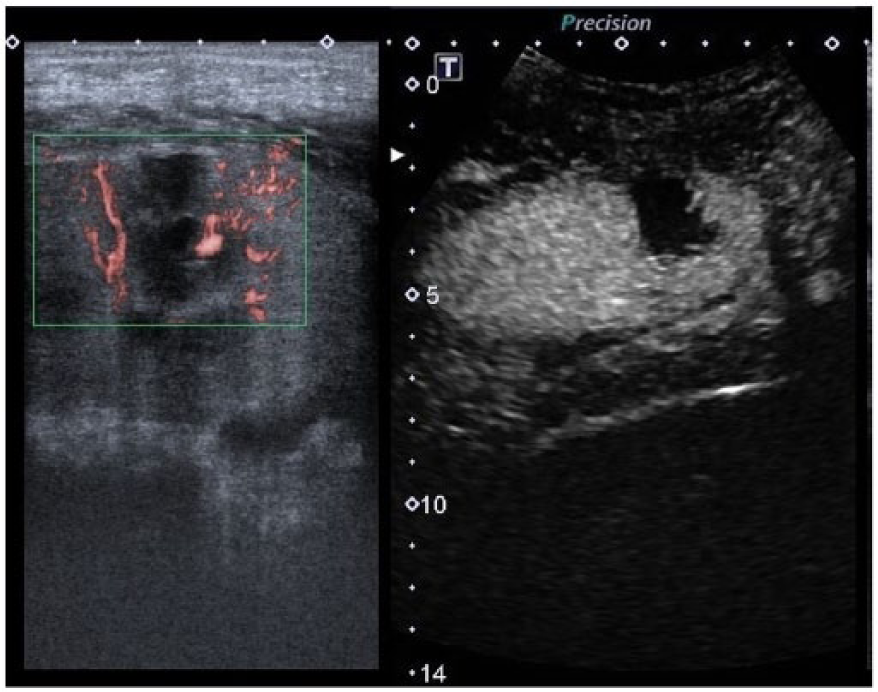
Segmental renal allograft infarction. Left: Doppler with Superb Microvascular Image (SMI) revealed a poorly marginated irregular sonolucent area with echoes within it without perfusion. Right: Contrast-enhanced ultrasound that demonstrates perfusion to the upper and lower renal pole with sharp wedge-shaped segmental loss of perfusion in the inferior midportion, a finding compatible with infarction.
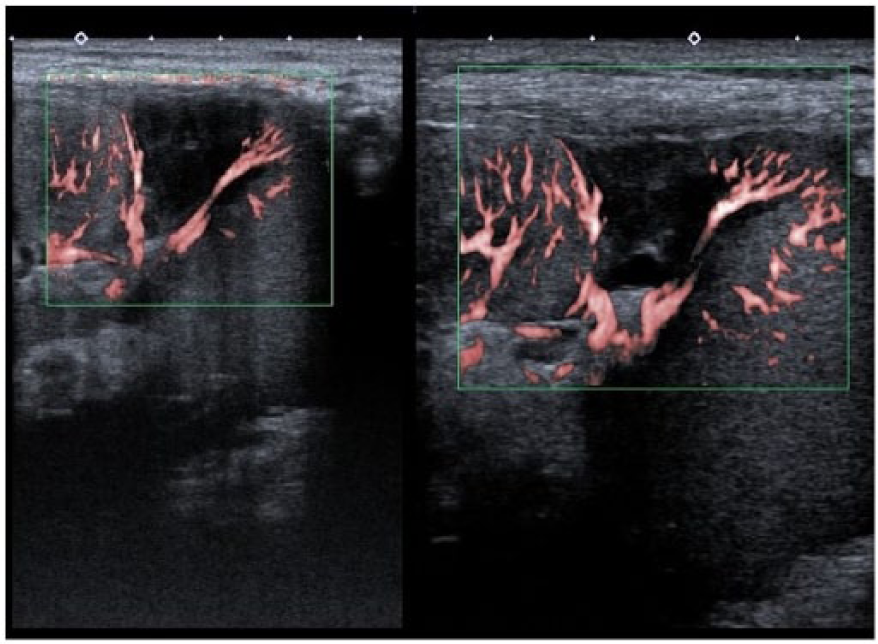
Segmental renal allograft infarction. Left: 27 days after transplantation, a repeated SMI showed a more smooth and marginated appearance and almost anechoic infarction in relation to the first examination, suggestive of necrosis. Right: 104 days after transplantation, the ultrasound with SMI did not show any changes.
Since CEUS was performed at our facility as off-label clinical research, the ethics committee approved the study according to local legal requirements, and informed consent was obtained from the patient.
Discussion
Warm ischemia time in the donor is defined as the time between artery occlusion and perfusion of the donor kidney. Longer warm ischemia time in donors could be a unique risk factor and may have influenced the segmental infarction in this patient. In native kidney, renal infarction often presents with nonspecific symptoms like flank pain and/or abdominal pain, nausea, vomiting, fever, and hematuria and the onset of symptoms may be insidious or rapid. 1 On the other hand, diagnosis of segmental renal infarction in a renal allograft relies mainly on high clinical suspicion, raised lactate dehydrogenase level, and imaging studies. 3 Segmental allograft necrosis is one of a wide variety of surgical complications that can occur after renal transplantation.5,6
Indeed, segmental infarction was identified in 13 of 277 consecutive renal allograft recipients (4.7%). 3
In cadaveric allografts, the risk of segmental infarction is associated with suboptimal graft quality, 3 whereas a longer warm ischemia time represents a higher risk in living-related donor transplants. 7 In addition, an association with allografts with multiples arteries has also been reported. 3
Although laparoscopic nephrectomy results in greater donor satisfaction, segmental infarction has been associated with this procedure, 8 which is likely due to a longer warm ischemia time. 7
In this case, it may be worthwhile to investigate any causal relationship between segmental infarction and prolonged warm ischemia, although the total operative time was acceptable. Indeed, in comparison to the range of 90–300 seconds reported by others, 7 420 seconds of warm ischemia time in the donor of our case was longer than satisfactory. In this case, the LDH level did not increase in parallel with the onset of infarction, suggesting that such an increase is not highly sensitive for the early detection of infarction.
Segmental renal infarction is usually associated with allograft dysfunction. 3 However, sometimes this impairment is negligible due to the small area of the infarct. The patient showed a normal postoperative urine output, but serum creatinine decreased slowly, and did not return to normal after 1 week. However, dialysis was not required. The segmental infarction was the only risk factor that may explain this reduced allograft’s function. Given segmental infarctions may hinder allograft function, earlier diagnosis of this condition may avoid further inappropriately harmful procedures. Moreover, this may help explain, at least in part, the “stuck creatinine” as proposed by McArthur and Baxter. 9 It is well known that most segmental infarctions are asymptomatic. 3 In disagreement with some case reports, the infarction was associated with urine leakage and required polar nefrectomy.5,6 Since this patient presented with no signs of graft rupture, such as urine extravasation or hematuria, no intervention was undertaken.
The rise in creatinine level that led to readmission of this patient could be multifactorial, including (1) tacrolimus-induced nephrotoxicity based on the increased whole blood levels of tacrolimus (from 3.7 to 14.0 ng/l) and subsequent decrease in the creatinine level associated with tacrolimus dosage reduction; and (2) pathophysiologic effects of tumor necrosis factor alpha released from the necrotic area related to the infarction, which could have acted as endogenous tubular toxins. 10
In relation to the sonographic appearance of renal infarction, it has been reported in experiments with canines that, following acute segmental renal artery occlusion, the echogenicity of the affected renal parenchyma changes from hypoechoic at 24 hours to a well-defined and uniformly echogenic focus at 17 days associated with marked foam cell, macrophage, lymphocyte, and plasma infiltration. 11 In accordance with this, one report of renal infarction in which the patient presented with an acute onset of flank pain, the gray-scale sonography of the kidneys was normal, 12 while in two cases of subacute or chronic presentation, renal sonography demonstrated an echogenic wedge-shaped renal mass, without posterior shadowing. 13 In this case study, the infarct area changed from being poorly marginated and slightly hypoechoic at day 4 to having a clearly defined marginated appearance and being hypoechoic at day 11; the latter appearance did not change up to the last examination at day 104. We hypothesize that the histological changes seen in the experimental study were inhibited in this patient by immunosuppression putting an end to echogenicity changes. Therefore, we theorize that acute segmental renal allograft infarction, in patients under immunosuppression, may not demonstrate a sequence of changes that may aid in dating the infarct, until at least 104 days.
Although CDUS using SMI yielded a strong suspicion of segmental infarction, CEUS clearly provided an excellent visualization of the infarct. Evidence is growing that ultrasound contrast agents are a necessary adjunctive tool to sonography studies, they present a pure intravascular distribution. 14
Because of the advantages CEUS plays an important role in the diagnosis of renal transplant infarctions, 9 more studies are needed to confirm its utility for transplant recipients with unexplained raised creatinine. It is worth noting, that the equipment sensitivity was critical for showing the borders of the infarcted area in the follow-up of the evolutionary changes of the infarct.
Conclusion
The development of a segmental infarction within a renal allograft is not uncommon and can be complicated by decreased organ function. CEUS played an important role in this diagnosis of a renal allograft infarctions. It yielded a timely and exact diagnosis that negated the need for further invasive procedures. The knowledge for sonographers and nephrologists on the limited documentation of gray-scale sonographic changes in acute segmental renal allograft infarction will be useful in approaching transplant recipients.
Footnotes
Acknowledgements
Bracco (Milan, Italy) provided the contrast agent (Sonovue®) free of charge.
Toshiba (Tokyo, Japan) provided Superb Microvascular Image® free of charge.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This case report is made possible through the support from Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ).