
Abstract
Sonography is the imaging modality of choice to evaluate suspected intrauterine and extrauterine pregnancies. Determining the anatomic location of an ectopic pregnancy can be challenging, particularly when the ectopic is located external to the fallopian tube. Ovarian ectopic pregnancy is one of the rarest forms of nontubal ectopics. This report documents one such uncommon case of ovarian pregnancy in a woman presenting with light vaginal bleeding in early pregnancy, with subsequent rupture and laparotomy. Histopathologic analysis confirmed the diagnosis of ovarian ectopic pregnancy.
Introduction
Ectopic pregnancy (EP) is the most common cause of pregnancy-related death in the first trimester, and sonography is the imaging method of choice when it comes to evaluating a woman with a suspected ectopic pregnancy. 1 The vast majority of ectopic pregnancies occur within the fallopian tube, comprising 95% of all ectopic pregnancies. 2 However, the remaining 5% of ectopics are nontubal in origin. These sites can include the abdomen, the cervix, the ovary, and within a hysterotomy scar. Due to the rarity of these presentations and their associated diagnostic challenges leading to misdiagnosis, they are associated with a higher level of maternal morbidity. 2 Ovarian ectopic pregnancies are one of the rarest presentations, with an incidence rate of approximately 1% to 6% of all diagnosed ectopics.2,3 Despite the enhanced capabilities of modern sonographic equipment, preoperative diagnosis of ovarian pregnancy remains a challenge and is most often made at time of surgery. Increased awareness of these rare, but potentially life threatening, presentations by sonographers and health care providers can lead to earlier and possibly less invasive treatment options for the patient.
Case Study
A gravida 2 para 1 (G2P1) woman in her late thirties presented for a scheduled sonogram due to complaints of ongoing light vaginal bleeding. She was currently 7 weeks 5 days by her last known menstrual period. Her medical history was significant for secondary infertility, for which she was being treated with ovulation induction by means of clomiphene citrate (50 mg). She had no history of endometriosis, sexually transmitted disease, or pelvic inflammatory disease, nor had she any previous gynecological surgery. She had undergone a hysterosalpingogram as part of her infertility work-up, which reported a normal uterus and patent fallopian tubes bilaterally. The patient did not have any current laboratory values, with her most recent serum beta-human chorionic gonadotropin (beta-hCG) level being some 2 weeks prior. At that time, her beta-hCG was 186.8 mUI/mL, corresponding to a gestational age of 4 to 5 weeks of pregnancy.
A transvaginal sonogram was performed using an RIC5-9D intracavity probe on a GE Voluson E6 (General Electric Healthcare, Waukesha, Wisconsin, USA). The sonogram revealed an empty uterus (Figure 1) with a 10.2 mm endometrial stripe. The left ovary contained a simple corpus luteum cyst, as well as a 1.6 cm × 1.4 cm hyperechoic mass with thick walls and an anechoic center (Figures 2-3). Both of these masses demonstrated vascular flow around the periphery (Figure 4). This second mass could not be separated from the ovarian tissue, even with the application of gentle pressure with the endovaginal transducer. No yolk sac or fetal pole was seen. There was a second simple cystic structure located in the left adnexa as well, measuring 2.1 cm, as well as a complex, hypoechoic fluid collection, consistent with clot (Figures 5-6). The right adnexa appeared sonographically normal, with no additional fluid seen in the pelvic cavity.
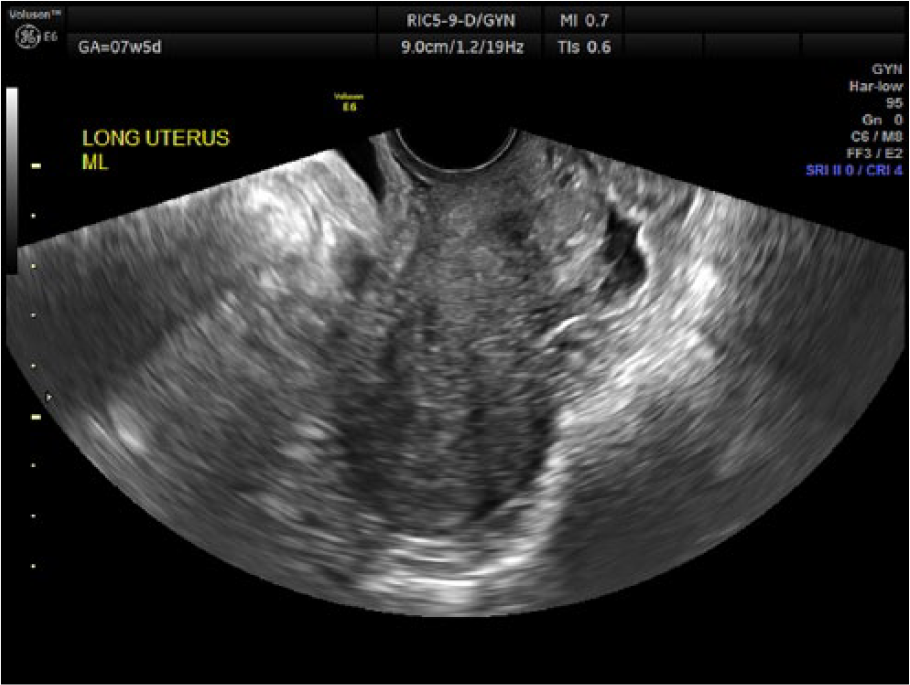
Transvaginal gray-scale image of the empty uterus in the sagittal plane.
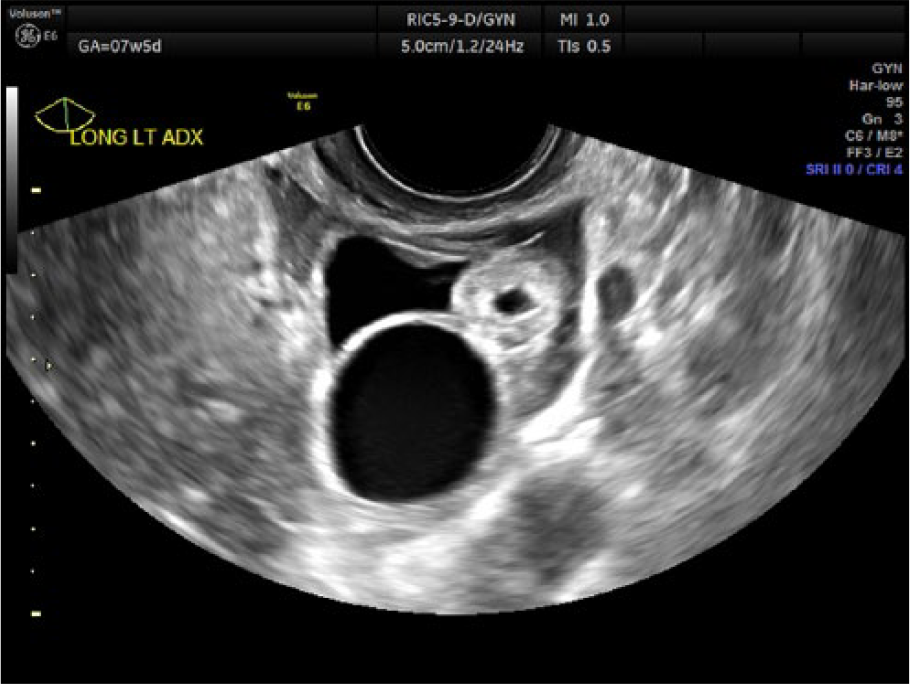
Transvaginal gray-scale image of the left ovary showing a corpus luteum cyst and an echogenic mass.
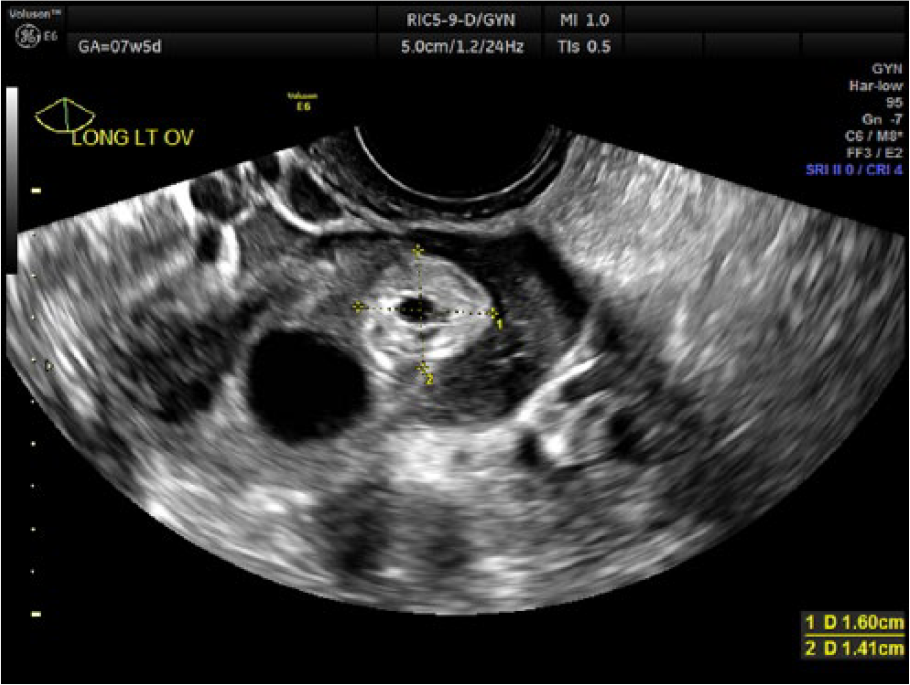
Transvaginal gray-scale image of the echogenic mass within the left ovary.
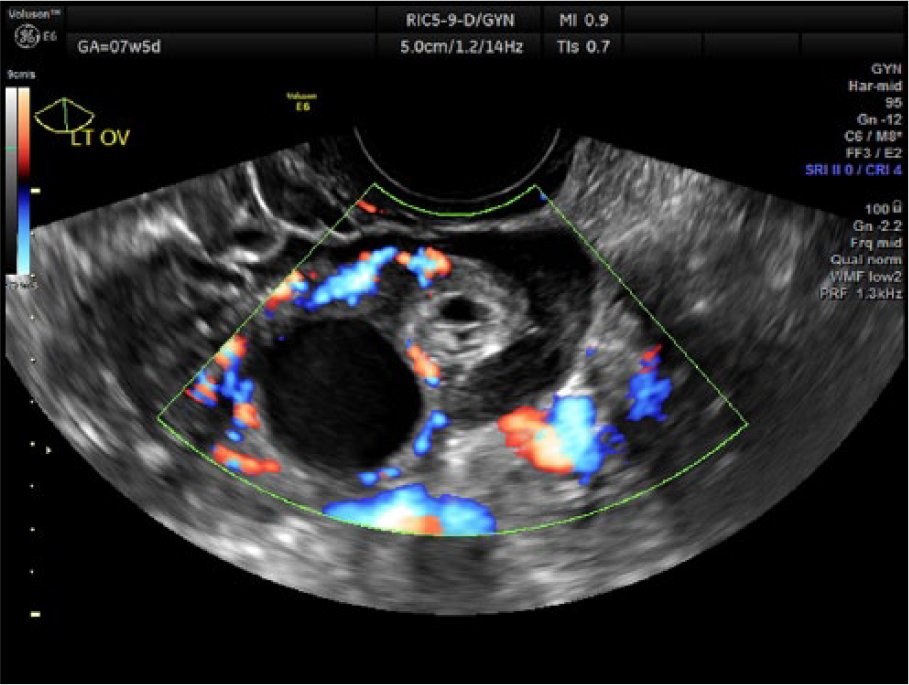
Transvaginal color Doppler image showing the vascularity around both ovarian structures.

Transvaginal gray-scale image of the left adnexa demonstrating a complex fluid collection and an additional cystic structure.
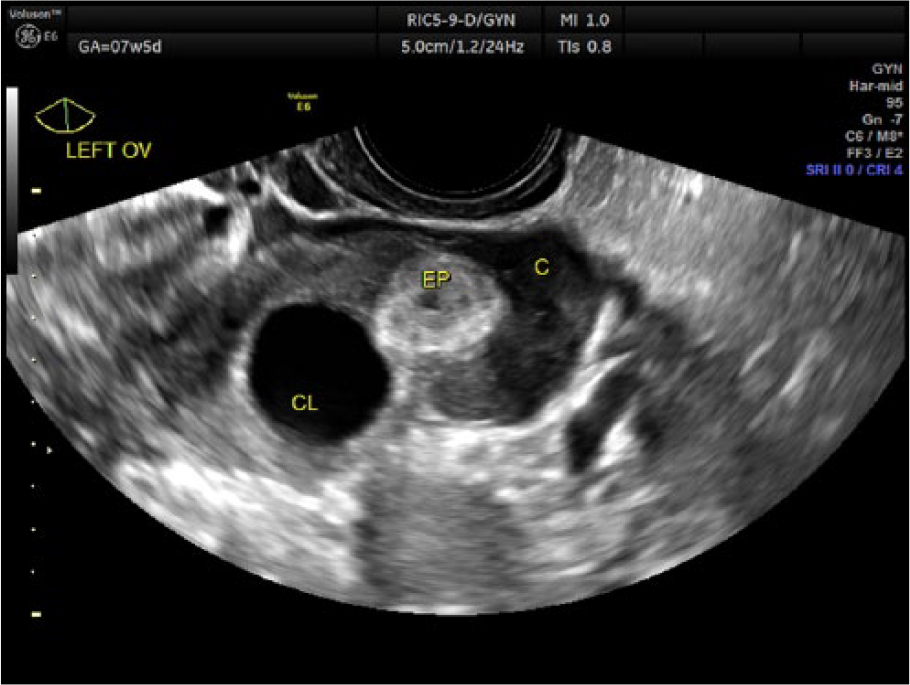
Transvaginal gray-scale image of the left ovary. c, clot; CL, corpus luteum; EP, ectopic pregnancy.
Laboratory work completed after her sonogram revealed a beta-hCG level of 2,442.0 mUI/mL, demonstrating an abnormal rise over the past 2 weeks and not consistent with her gestational age of nearly 8 weeks. This information, taken along with the sonographic findings, was highly suggestive of an ectopic pregnancy. The exact location of the suspected ectopic could not be confirmed with certainty. The patient denied any pelvic pain, dizziness, or shoulder pain. Her vital signs were stable, with no palpable adnexal mass. The patient was counseled on the suspected ectopic pregnancy. As she was in no acute distress, it was decided that she would follow up in 2 days’ time for additional serum beta-hCG levels before determining her course of management. Ectopic precautions were reviewed with the patient.
Two days later, the patient presented to an emergency room complaining of significant pelvic pain and increased vaginal bleeding. Her beta-hCG level had dropped to 1235.5 mUI/mL. Physical exam revealed tenderness in the left adnexa and a palpable mass. A transvaginal pelvic sonogram was ordered and completed using an Acuson Sequoia 512 with an EV8C4-S transducer (Siemens Medical Solutions, Mountain View, California, USA). This scan revealed a moderate amount of free fluid in the pelvic cavity and a large complex mass in the left adnexa (Figure 7). The previously described echogenic left ovarian mass was no longer visualized. The patient was taken for a laparotomy for suspected ruptured left ectopic pregnancy. During the surgery, 300 cubic centimeters of clot and dark blood were removed. What appeared to be a ruptured hemorrhagic cyst was noted on the left ovary with active bleeding. Attempts to completely dissect this were unsuccessful. A simple left ovarian cyst as well as a left paratubal cyst were also noted and drained. The left fallopian tube was otherwise unremarkable, as were the right ovary and tube. Subsequent histopathologic analysis of the left ovarian mass revealed immature placental villi and clot, confirming the presence of an ovarian ectopic pregnancy. The patient’s recovery was unremarkable, and she was discharged home on postoperative day 1.
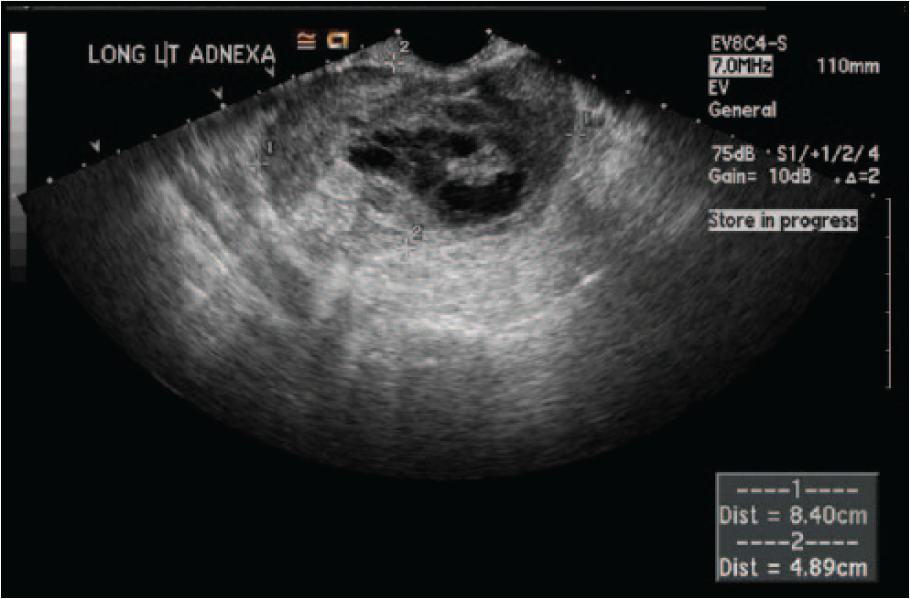
Transvaginal gray-scale image of the left adnexa showing a complex mass.
Discussion
Primary ovarian pregnancies are one of the rarest types of extrauterine pregnancies, with an estimated incidence rate of approximately 1% to 6% of all diagnosed ectopic pregnancies.2,3 Ovarian ectopic pregnancies (OEPs) result from secondary implantation on the ovary or from failure of follicular extrusion. 4 Although many earlier studies linked OEP to the use of intrauterine contraceptive devices, more recent research has refuted this ascertion. 5 Other risk factors for OEP include a history of endometriosis, ovulation induction and other assisted reproductive technologies, and advanced maternal age.1,6,7 The clinical presentation of OEP is similar to other ectopic pregnancies, namely, mild-to-moderate pelvic pain, vaginal bleeding, abnormal beta-hCG levels, and a palpable adnexal mass.6-8 The patient in this case had a few risk factors, including being of advanced maternal age and the use of ovulation induction medication. Differential diagnoses of an OEP can include a corpus luteum cyst, a hemorrhagic ovarian cyst, appendicitis, tubal ectopic, or an early or failed intrauterine pregnancy (IUP).6,9
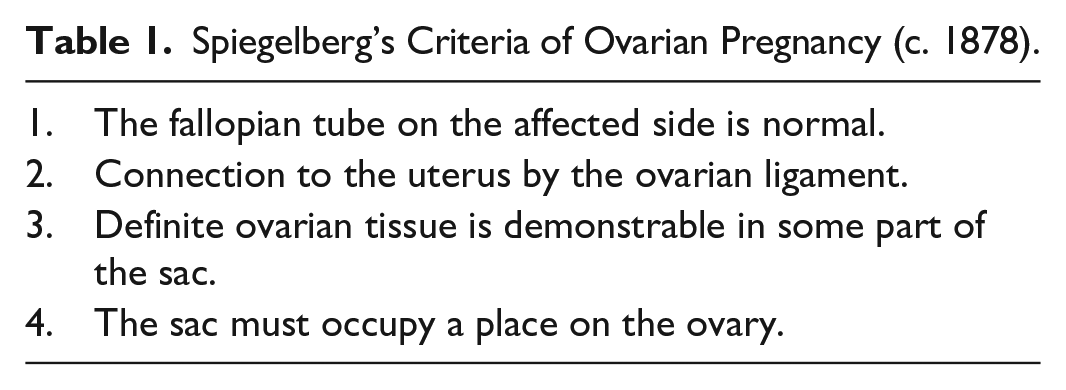
More than a century ago, Otto Spiegelberg, MD, described four main criteria (Table 1) that remain the standard in diagnosing a primary ovarian pregnancy to this day. 10 It is unfortunate that the Spiegelberg criteria are all surgical and cannot be proven sonographically.
Spiegelberg’s Criteria of Ovarian Pregnancy (c. 1878).
Sonographic diagnosis of ovarian ectopic pregnancies remains extremely difficult, as their appearance can be easily misdiagnosed as a hemorrhagic cyst, a tubal ectopic, or a corpus luteum cyst (CLC). 8 Comstock et al 6 reported on the sonographic characteristics of proven primary ovarian pregnancies. Their study reported that OEPs present on sonogram as thick-walled, echogenic rings with anechoic centers that are located within or on the surface of the ovary. This differentiates them from a tubal EP ring, which was much thinner by comparison. The echogenicity of the OEP is increased when compared to the ovarian stroma, whereas a CLC is usually less echogenic.
A true ovarian pregnancy cannot be separated from the ovarian tissue (a negative “sliding organ sign”). This can be evaluated by applying gentle pressure to the mass by means of the endovaginal probe from within or with manual compression of the patient’s abdomen by hand. Most extrauterine pregnancies will be clearly separated from the ovary using this technique, although there can be some overlap in appearance, as a tubal pregnancy can become adherent to the ovary. 11
The use of duplex Doppler to distinguish between an ovarian ectopic pregnancy and a corpus luteum cyst is unreliable. They can each display the so-called “ring of fire” sign, as both the ectopic ring and the walls of a corpus luteum can have significant vascularity.12,13 In addition to the use of color Doppler, pulsed wave Doppler is likewise of limited value. Studies have shown that there is no significant difference between the peak systolic velocities (PSV) of an ectopic pregnancy compared to that of a corpus luteum. The same study also concluded that although a very high resistive index (RI > 0.7) or a very low one (RI < 0.39) can be useful in differentiating an EP from a CLC, there is a significant overlap between the two.14,15
The presence or absence of an identifiable embryo or yolk sac is also not useful when distinguishing between a tubal pregnancy and an OEP. The Comstock et al 6 study found that the appearance of an ovarian ectopic “was not as advanced as one would expect from the gestation dates,” that is to say, a yolk sac or identifiable embryo was very rarely visualized. However, this is true of all forms of ectopic pregnancy, as EP in general typically presents as a nonspecific adnexal mass, with a live embryo seen in less than 10% of sonographically detected ectopics. 16 The American College of Radiology continues to rate transabdominal and transvaginal sonography as usually appropriate for patients with acute pelvic pain, gynecologic etiology suspected, and a positive beta-hCG. 17
Laparoscopy is considered the gold standard in the definitive diagnosis of, and treatment for, OEP, and conservation of the ovary is possible in many cases.9,18 Even with direct visualization during surgery, an ovarian pregnancy can still be mistaken for a hemorrhagic cyst (as the surgeon did in this case), and histologic confirmation may be required to confirm the diagnosis.19-21 In the case presented, the diagnosis of an ectopic pregnancy was presumed due to the abnormal serum beta-hCG levels, empty uterus, and suspicious sonographic adnexal findings. Given her lack of symptomology, features of rupture, or palpable mass at the time of her initial presentation, combined with the rarity of the condition, a definitive diagnosis of primary ovarian pregnancy (versus a tubal ectopic) would have been very difficult. At the time of surgery, all four of Spiegelberg’s criteria were met: the ipsilateral tube was normal and separate from the ovary, the pregnancy occupied a normal position on the ovary, the ovary was attached to the uterus by the ovarian ligament, and there was pathologic confirmation of placental tissue attached to the ovarian stroma.
Conclusion
Ectopic pregnancies are one of the leading causes of morbidity and mortality in a woman of reproductive age, and sonography plays a critical role in the diagnosis and evaluation of a suspected extrauterine pregnancy. This case presents an example of an ovarian ectopic pregnancy that was not conclusively diagnosed until after surgery. Although preoperative diagnosis of OEP remains very challenging, the presence of a hyperechoic, thick-walled mass in the ovary with the absence of an identifiable intrauterine pregnancy, along with suspicious clinical symptoms and serum beta-hCG values, should prompt the clinician to consider OEP as a potential diagnosis.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.