
Abstract
Ectopia cordis is a rare congenital anomaly in which the heart is displaced outside of the thoracic cavity. This case report describes the in utero diagnosis of thoracic ectopia cordis in conjunction with fetal acrania, both of which were thought to result from an amniotic band located near the fetal head.
Introduction
Ectopia cordis is defined as partial or complete displacement of the heart outside of the thoracic cavity. 1 It may be an isolated malformation or associated with ventral wall defects that affect the thorax or abdomen.1,2 In some cases, ectopia cordis is thought to be the result of amniotic band syndrome, in which strands of the amnion adhere to the fetus, resulting in an open defect.2–4 This is a case report of thoracic ectopia cordis with acrania diagnosed in utero.
Case Report
A 23-year-old gravida 2 para 1 female was referred for an ultrasound examination at 16 weeks 6 days because of suspected fetal anomalies seen at an outside facility. Sonography was done using a Philips iU-22 ultrasound system (Philips Medical, Bothell, Washington) with a C5-1 curved array transducer. Multiple fetal anomalies were visualized, including thoracic ectopia cordis, acrania, a single umbilical artery, and bilateral clubbed feet (Figures 1 and 2). A possible amniotic band was also seen near the fetal head (Figure 3). The patient was counseled regarding available testing and fetal prognosis and desired termination of the pregnancy. A dilation and evacuation (D&E) was done the following day. Chromosomal microarray testing was done on DNA extracted from the fetal tissue, and cytogenic studies showed a normal, 46XY karyotype. Confirmation of the diagnosis of amniotic band syndrome was not possible following the D&E.
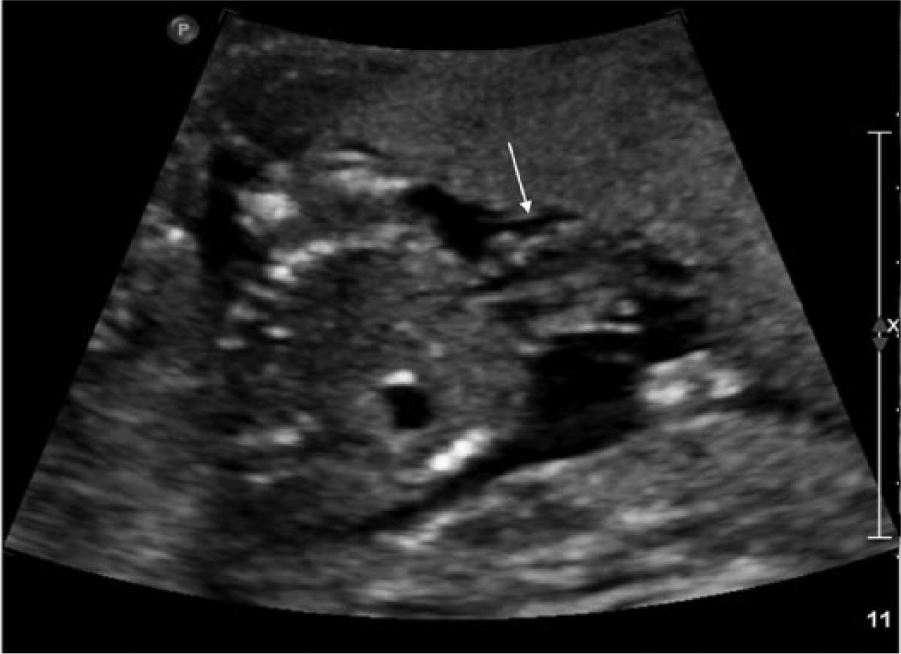
Transverse gray-scale image through the fetal chest showing displacement of the fetal heart (arrow) outside of the thoracic cavity.
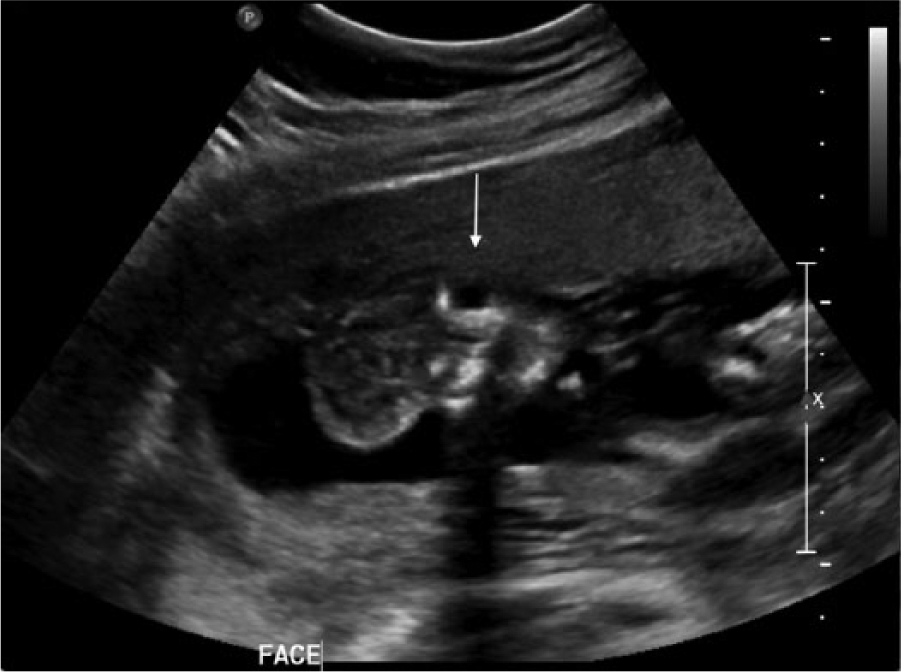
Coronal gray-scale image of the fetal face (arrow) showing absence of the cranium with cerebral tissue exposed directly to the amniotic fluid.

Gray-scale image of an amniotic band-like structure (arrow) that appeared to be attached to the fetal cerebrum.
Discussion
Ectopia cordis is a rare congenital anomaly that occurs with an incidence of 5.5 to 7.9 per million live births.1,4 Around the fourth week of gestation, the embryonic disc goes through the process of gastrulation and neurulation, forming a tube-like structure consisting of three germ cell layers: ectoderm, endoderm, and mesoderm.5,6 The endoderm and mesoderm ultimately form the gut tube and body wall, which if it fails to close properly results in a ventral wall defect such as ectopia cordis, gastroschisis, omphalocele, bladder, or cloacal exstrophy. 5
Ectopia cordis is classified into five types according to the location of the heart2,3,7:
cervical (3%), in which the heart is in the neck with an intact sternum;
thoracocervical (<1%), in which the heart is displaced through the superior portion of a split sternum;
thoracic (60%), in which there is a sternal defect and the heart lies partially or completely outside of the chest;
thoracoabdominal (7%), in which the heart is displaced through a defect in the lower sternum in association with diaphragmatic and ventral wall defects;
abdominal (30%), in which the heart is displaced into the abdomen through a defect in the diaphragm.2,3,7,8
Of these types, thoracoabdominal has the best prognosis while cervical and thoracocervical are incompatible with life.3,8
The thoracoabdominal type accounts for 7% of cases. Pentalogy of Cantrell is the most common presentation of this anomaly. In its complete form, it consists of a thoracoabdominal ectopia cordis in association with defects of the inferior sternum, ventral diaphragm, diaphragmatic pericardium, and a midline supraumbilical abdominal wall defect (usually omphalocele). Congenital heart anomalies are commonly seen in fetuses with pentalogy of Cantrell.7,9,10
The exact cause of ectopia cordis is variable. Failure of the heart to migrate from its embryonic location in the neck would result in cervical ectopia cordis. Other forms are thought to be the result of defective formation and differentiation of the ventral mesoderm at about 14 to 18 days of gestation. A thoracoabdominal ectopia cordis results from failure of formation of the transverse septum, which develops into the anterior diaphragm and its corresponding pericardium. The sternal and abdominal wall defects result from failure of migration of the paired anterior body folds.5,7,10
Intracardiac anomalies are commonly associated with ectopia cordis. The most common include ventricular septal defects (VSD), atrial septal defects (ASD), tetralogy of Fallot (TOF), pulmonary stenosis, and left ventricular diverticula.2,3,7,8,10 Ectopia cordis has also been associated with chromosome anomalies such as trisomy 13, trisomy 18, trisomy 21, XXY, and Turner syndrome (45X). Chromosomal analysis should be considered with this anomaly.3,7,11
Many extracardiac anomalies have also been reported to occur in conjunction with ectopia cordis, including amniotic bands, body stalk anomalies, diaphragmatic hernia, cleft lip and palate, anencephaly, encephalocele, skeletal malformations, gastroschisis, and most commonly omphalocele.3,4,7 As with any fetal anomaly, if one abnormality is visualized, a thorough investigation of all fetal systems should be carefully analyzed.
In some cases, ectopia cordis may be the result of amniotic band syndrome.12,13 In this setting, amniotic bands may be seen attached to the ectopic heart or a defect in the thorax or abdominal wall.2,7,8 Amniotic band syndrome is a sporadic condition that has an incidence of approximately 1:1200 to 1:15 000 live births. In most cases, the risk for recurrence in a subsequent pregnancy is very low.12,13 There are two theories regarding the pathogenesis of amniotic band syndrome. The intrinsic theory suggests abnormal development of the embryonic germinal disk. The more accepted is the extrinsic theory in which early amnion rupture leads to fibrous bands attaching to fetal parts, resulting in a range of abnormalities.12–14 Depending on the region of attachment or constriction, webbing of the fingers or toes, limb amputations or defects (including clubfeet), craniofacial abnormalities, and visceral abnormalities may occur.12,15
Treatment options for ectopia cordis most commonly require a multisurgical approach. Repair of the omphalocele, sternal, diaphragmatic, and pericardial defects are included in the initial phase, followed by a soft tissue covering for the heart. The soft tissue covering prevents fluid loss and cardiac desiccation and provides protection for the heart. Repair of intracardiac anomalies and reducing the heart into the chest cavity is usually done in the second phase. Surgical correction can be challenging due to hypoplasia of the thoracic cavity. Reducing the heart into the small thorax can cause compression of the heart and kinking of the great vessels. The overall prognosis of ectopia cordis is poor and is dependent on the size of abdominal wall defect, the type and severity of ectopia cordis, and also the associated intra- and extracardiac anomalies present.3,7,8,16
Conclusion
Sonography can have an important role in identifying ectopia cordis and its associated abnormalities. Early diagnosis is important for counseling the patient on outcomes as well as determining treatment options if warranted.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.