
Abstract
Sonography of the lung has been shown to be a useful bedside diagnostic tool in critical care units for pneumothorax (PNX). A case of PNX is reported in which all the standard sonographic findings were present but coexisting with the lung pulse sonographic sign. Descriptions of the sonographic findings of PNX, the lung point sign, and the lung pulse sign are given and discussed, with the characteristics that should be used to avoid misdiagnosis.
Keywords
In recent years, sonography of the lung has been shown to be a useful diagnostic tool for pulmonary consolidations, pulmonary edema, pleural effusions, pleural masses, and pneumothorax (PNX).1–3 It is of particular interest for the evaluation of critically ill patients at the bedside. In PNX, air is confined to the pleural space, making penetration of the ultrasound beam beyond the parietal pleura impossible. Accordingly, parenchymal lung structures cannot be visualized. However, the recognition of certain artifacts allows appropriate diagnoses. Moreover, sonography can also be useful for the quantification of the volume of PNX.
In critical care settings, PNX is frequent, given the widespread use of mechanical ventilation and the complications of central venous canalization techniques.
A missed diagnosis can have significant consequences if not resolved quickly. The gold standard for diagnosis is computed tomography (CT), but a portable chest radiograph is usually performed when the patient cannot be transferred from critical care to the radiology department. Obtaining these tests can take significant time, and there are frequent false negatives as bedside chest radiography misses a substantial proportion of cases, independent of the expanse of the PNX. 4
A systematic review of the literature from 1995 to 2010 provided the accuracy of sonography and currently accepted descriptions of the sonographic signs of PNX and their superiority over conventional radiology. 3 Several reports have shown that lung sonography is more sensitive than supine chest radiography and similar to CT in the detection of PNX.4–6
We report a case of PNX where all the signs described are present but coexisting with the lung pulse sonographic sign, which could lead to misdiagnosis.
Case Report
An 85-year-old woman was admitted to the critical care unit because of gastrointestinal bleeding. On admission, a central venous access catheter was placed in the left subclavian vein without complications. A few hours later, the patient was stable, asymptomatic, and with spontaneous breathing when a subcutaneous emphysema in the area of the left chest was noted. A portable anteroposterior chest radiograph was done, which showed no characteristic lines of PNX (Figure 1).
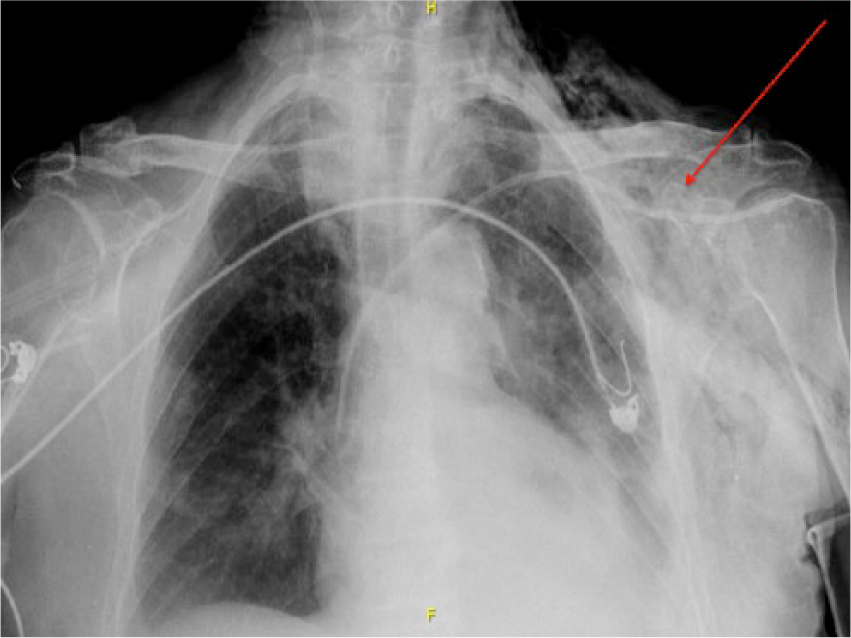
Anteroposterior chest radiograph with hyperclarity of the left chest and subcutaneous emphysema (arrow).
A sonographic examination of the lungs was done using a Mindray DP-50 ultrasonography system with a 12-MHz linear transducer (Mindray Ultrasound, Mahwah, NJ) to evaluate for pneumothorax after a central venous canalization. Initial evaluation was done in a mid-clavicular line at the left fifth intercostal space. There was an absence of comet tail artifacts and lung sliding, both in 2D and time-motion mode (M-mode) imaging, suggesting an anterior PNX. These characteristic findings of normal lung were seen in a similar exploration of the contralateral hemithorax. In an evaluation along the left anterior axillary line at the eighth intercostal space, a lung point sign was detected, confirming the diagnosis of PNX. However, a lung pulse sign was also identified at this level (Figure 2).
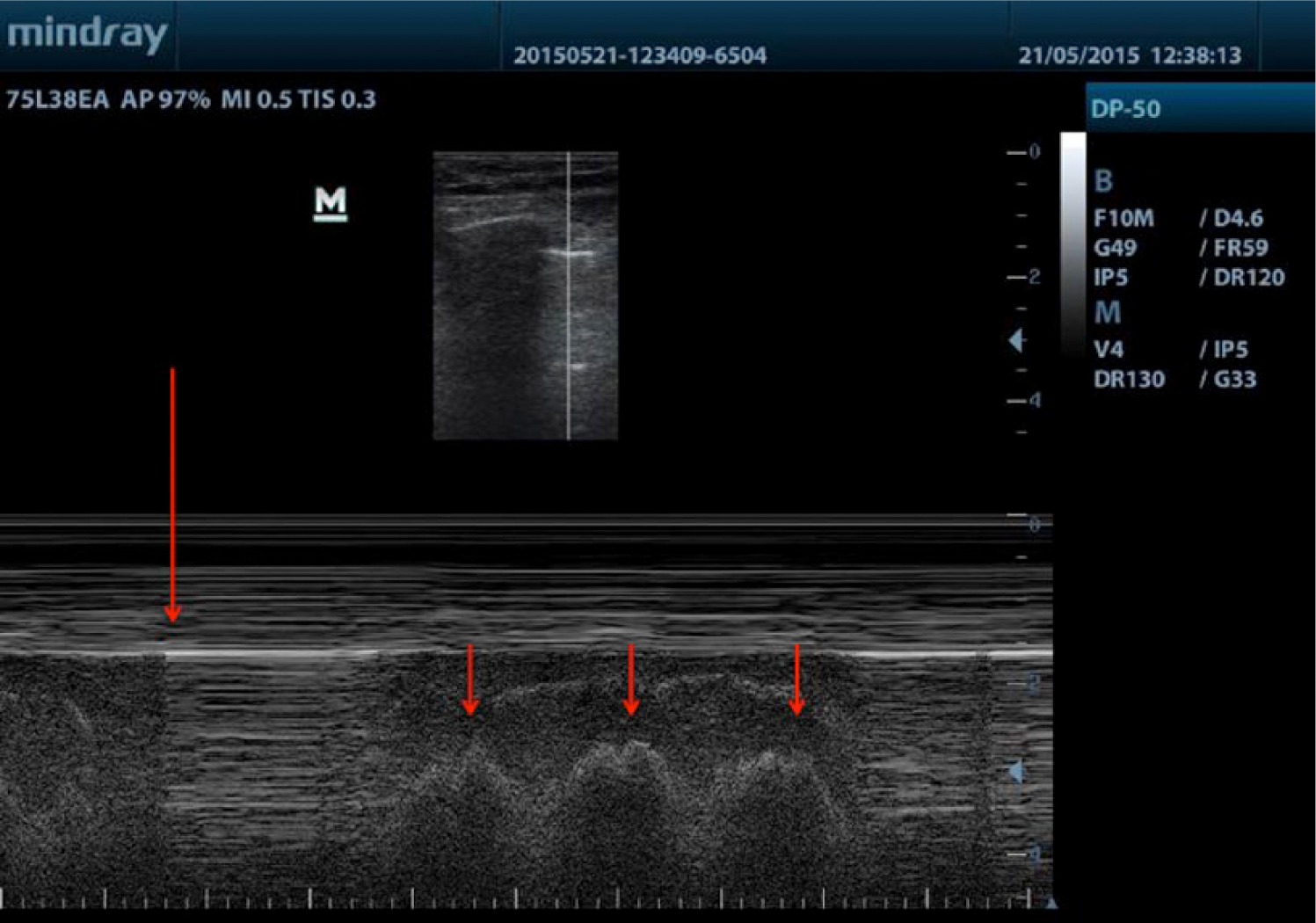
M-mode evaluation in the left anterior axillary line at the eighth intercostal space. A lung point sign with respiratory movements of the patient is seen (large arrow). When the lung is insonated, a lung point sign appears as well (small arrows).
The patient ultimately improved without pleural drainage, and a complete resolution of the PNX by sonography was seen at 48 hours, although in the following days, the lung pulse sign remained in the left lung.
Discussion
The sonographic diagnosis of PNX is based on the recognition or exclusion of some dynamic artifacts seen during the ultrasonography examination.4,5 A bright horizontal movement of the pleural line with respiratory movements, the lung sliding sign, allows exclusion of PNX in a critically ill patient, with a negative predictive value of100%.1,7 However, absence of the lung sliding sign does not necessarily confirm PNX, since several other conditions such as massive atelectasis, main-stem intubation, pulmonary contusion, acute respiratory distress syndrome, and pleural adhesions may also cause a motionless pleural line. 8
Using M-mode imaging, lung sliding appears as a homogeneous granular pattern below the pleural line. If PNX is present with absent lung sliding, horizontal lines are visualized beyond the pleural line. 2 B-mode imaging showing comet tail artifacts represents the adherence of the visceral pleura to the parietal pleura, 1 which rules out PNX with a true-negative rate of 100%, 9 but its absence also is not a powerful indicator of PNX. (See also the online video “Lung Sliding and Comet Tail Signs.)
A lung point sign is the detection of a point on the chest wall where a respiratory pattern is visualized intermittently (see the online video “Lung Point Sign in Pneumothorax”). This is where the lung adheres to the parietal pleura and corresponds to the lateral edge of the intrapleural air layer. This sign allows confirmation of PNX with 100% specificity, but it may be difficult to find. 10 Care must be taken not to confuse it with the lung pulse sign, which is simultaneous to the heart rate (see online video “Lung Pulse Sign”), whereas the lung point sign is synchronous with the patient’s breathing. A lung pulse sign caused by the transmission of the heart beat to the lung parenchyma may in some cases rule out PNX. 8 The usefulness of lung sonography in the diagnosis of PNX is based on a thorough examination and the careful application of the correct combination of the above-mentioned sonographic signs. As in the case presented here, a lung pulse sign detected in a lung sonography examination could lead to an erroneous rejection of PNX. Locating the lung point sign showed that heartbeat transmission to the pulmonary parenchyma was isolated to the area where the parietal pleura was adherent to the lung (see online videos “Simultaneous Lung Point” and “Lung Pulse”).
Conclusion
A case of iatrogenic pneumothorax not evident on plain film chest radiography but diagnosed by lung sonography was presented. A potentially complicating factor in reaching the appropriate diagnosis was the presence of a lung pulse sign as well. Without the other sonographic findings, this lung pulse sign could have mistakenly ruled out pneumothorax. The diagnosis was confirmed sonographically by an absence of lung sliding and the presence of the lung point sign at the eighth intercostal space.
Footnotes
Acknowledgements
We thank Susana Álvarez-González for her help in revising the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.