
Abstract
Takotsubo cardiomyopathy (often referred to as broken heart syndrome) typically presents as apical ballooning, chest pain, shortness of breath, abnormal cardiac enzymes, and electrocardiogram changes. Although takotsubo cardiomyopathy mimics symptoms of an acute coronary event, in most cases it is a reversible cardiomyopathy with no long-term effects. Echocardiography is the noninvasive test of choice for initial presentation and follow-up of this syndrome. A case of takotsubo cardiomyopathy is presented and its clinical signs, echocardiographic features, and management discussed.
Introduction
Takotsubo cardiomyopathy, also referred to as broken heart syndrome as well as a variety of other terms, was initially recognized in Japan in the early 1990s.1–4 Subsequent reports began to arise in the United States in the mid-1990s with the first series of reported cases in 2003. 5 Features of takotsubo cardiomyopathy include apical ballooning, chest pain, shortness of breath, abnormal cardiac enzymes, and electrocardiogram (ECG) changes.1,5,6 Although takotsubo cardiomyopathy mimics symptoms of an acute coronary event, in most cases it is a reversible cardiomyopathy with no long-term effects. 7 It is often attributed to stressful or highly emotional events in the patient’s life. Echocardiography is the noninvasive test of choice for initial presentation and follow-up for the assessment of function and physiology in patients with the underlying syndrome. 8
Case Report
A 79-year-old postmenopausal woman presented to the emergency room with left-sided chest pain, mild shortness of breath, and ST-wave abnormalities on her ECG. Her cardiac enzymes were elevated with troponin T levels of 0.077 microg/L (normal < 0.015 microg/L) 9 and a creatine kinase-myocardial band fraction level of 40.6 (normal value 0-3). 10 She had a significant medical history of atrial fibrillation, cerebral vascular accident, and atrial septal defect with a CardioSEAL® septal closure device (NMT Medical, Boston, Massachusetts, USA) placed 3 years prior. In recent weeks, she had had difficulty controlling her gastroesophageal reflux and had complaints of stress and discomfort. The initial impression in the emergency department was that the patient was undergoing a ST-segment elevation myocardial infarction, and she was rushed to the cardiac catheterization laboratory to evaluate her coronary arteries. A left heart catheterization with coronary and ventricular angiogram was ordered to determine whether coronary artery atherosclerosis was causing a myocardial infarction. The left ventricular (LV) angiogram (Figure 1A) showed moderate LV systolic dysfunction with severe hypokinesis of the mid and distal anterior apical, and mid and distal inferior walls, with an ejection fraction ranging from 30% to 35%. However, the coronary arteries appeared normal on the coronary angiogram (Figure 1B), with no evidence of any atherosclerosis or stenosis.
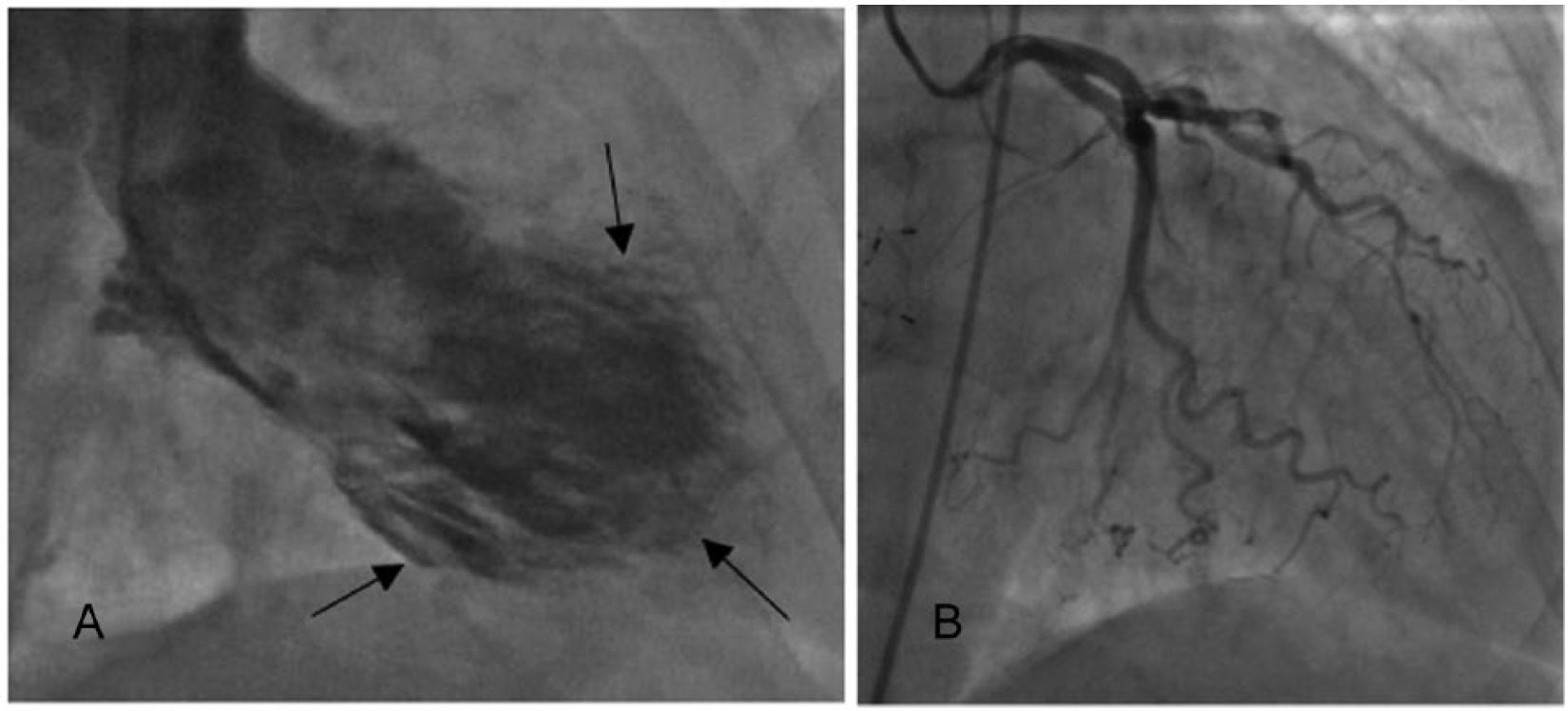
(A) Left ventricular (LV) angiogram demonstrating severe hypokinesia of the LV walls with ballooning of apical segments (arrows). (B) Coronary angiogram of this same patient showing normal coronary flow.
Further testing included a pulmonary ventilation/perfusion scan, which showed no evidence of pulmonary embolism, and a computed tomography scan of the chest with contrast that showed no evidence of aortic dissection. Using a Philips IE33 ultrasound machine (Philips Ultrasound, Bothel, Washington, USA) and S5-1 sector array probe, a transthoracic echocardiogram was done that showed moderately decreased LV systolic function with an ejection fraction estimated to be approximately 30% to 35%, abnormal LV diastolic function, and dilated akinetic apical wall segments (Figure 2). A transesophageal echocardiogram using a S7-2t probe showed thrombus attached to both sides of the atrial septal closure device along with a dilated, akinetic apex of the left ventricle (Figure 3).
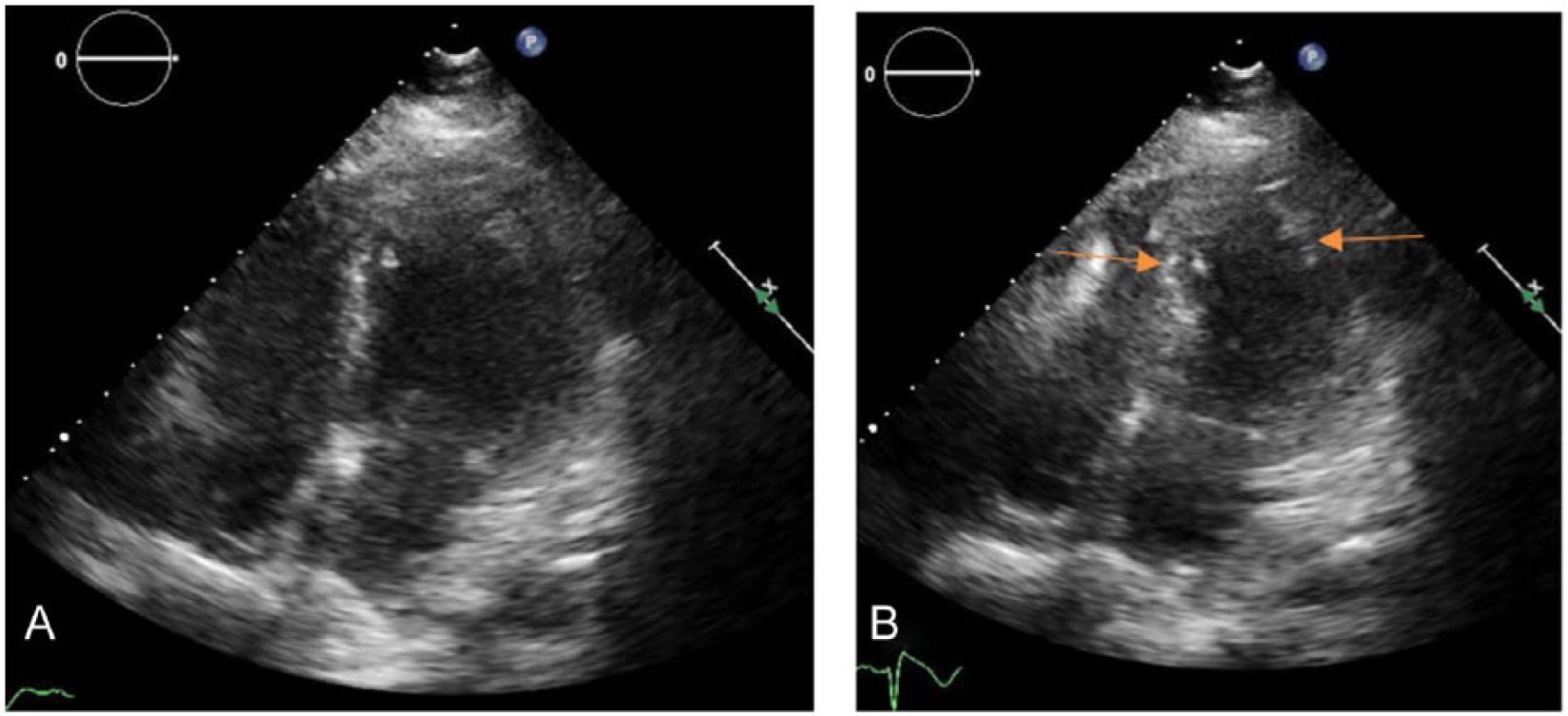
(A) Transthoracic echocardiographic apical four-chamber view in diastole showing ballooning of the apical segments. (B) Transthoracic echocardiographic apical four-chamber view in systole showing akinesis of the apical region (arrows).
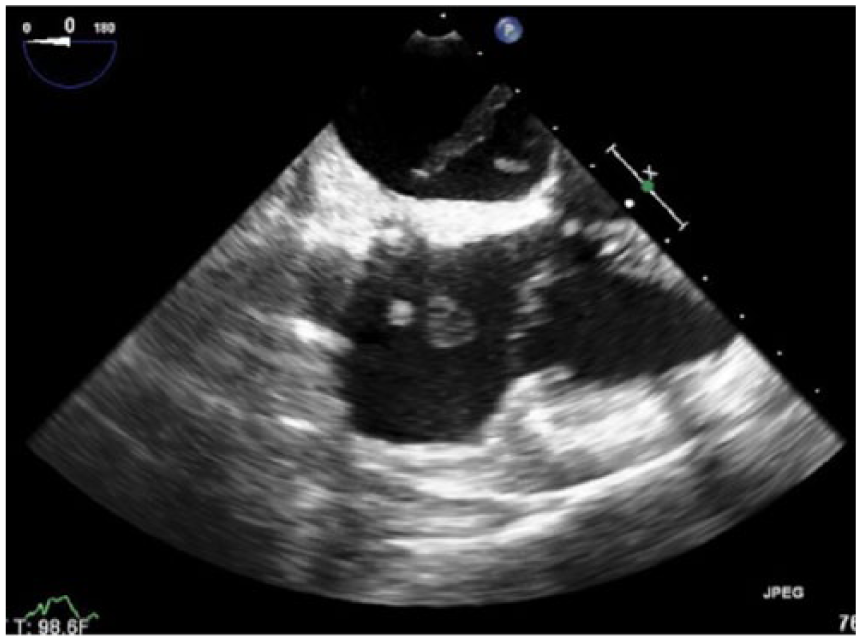
Transesophageal echocardiographic image showing the atrial closure device and thrombus forming on both sides into the right and left atria.
With the lack of physiological causes of a myocardial infarction demonstrated by the various diagnostic tests and the recently incurred medical stress, the patient was diagnosed with takotsubo cardiomyopathy. The patient was taken to surgery to evaluate and remove the atrial thrombi. A follow-up echocardiogram was done 10 months later showing LV systolic function only slightly diminished, normal ventricular size throughout, and no atrial thrombus.
Discussion
Takotsubo cardiomyopathy accounts for approximately 2% of suspected acute coronary syndrome cases each year. 8 It is named after the word takotsubo, meaning “octopus pot,” which describes its pot-like features seen on ventricular angiograms (Figure 4). Although the etiology cannot be precisely determined, the predisposing factor among most experts remains the theory of a stress-induced cardiomyopathy. Sharkey et al 1 have reported that 85% of cases suggestive of takotsubo syndrome were triggered by physical or emotional stress. These have included such highly stressful life events as death of a loved one, illness, loss of job, and asthma; however, in some circumstances, no stressors have been identified. 11 Patients who have high levels of catecholamines also may be at higher risk for takotsubo cardiomyopathy. 12 When a person is under stress, catecholamines are released into the blood stream. The more common types of catecholamines are known as dopamine, epinephrine, and adrenalin. Takotsubo has a high female predominance, with 90% of diagnosed patients being postmenopausal women. 13 A deficiency in estrogen and a heightened sympathetic release (catecholamines) are aspects of the currently favored theory of this female predominance.
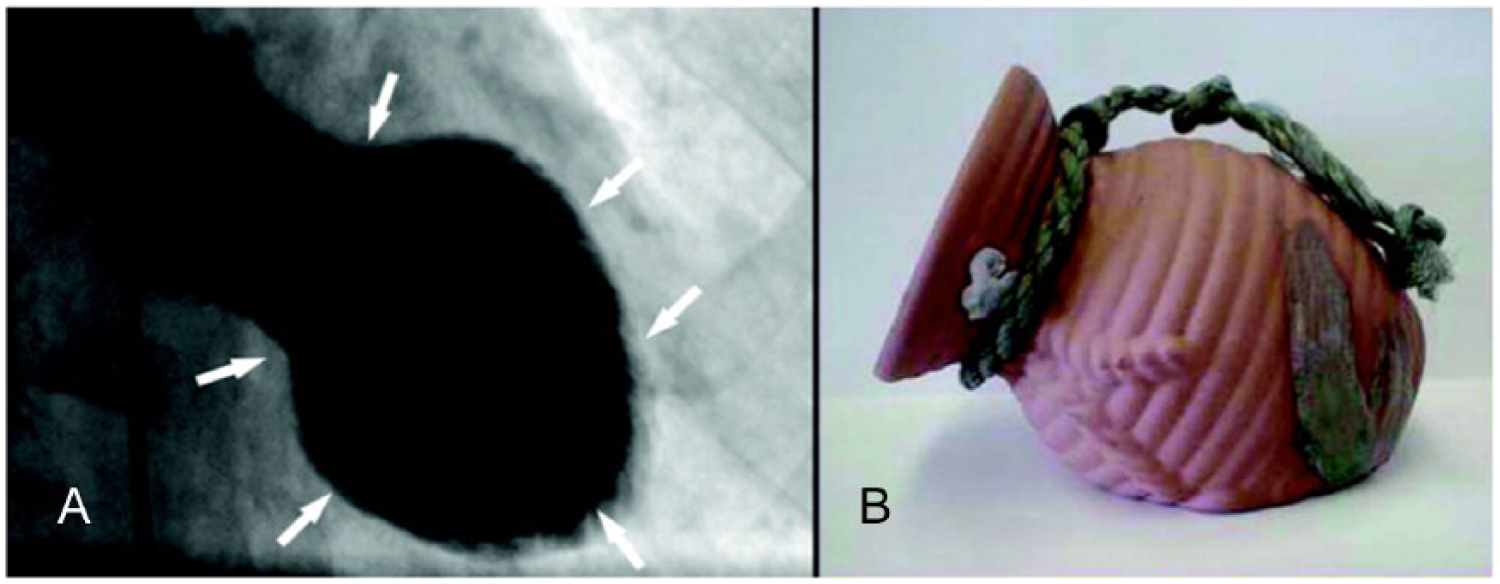
(A) Left ventriculogram of the heart during systole in patient with takotsubo cardiomyopathy. Note the narrow neck and abnormal ballooning of the left ventricle (arrows). (B) The ceramic pot used to trap octopi in Japan; notice the similarity of shape to the ventriculogram in (A). (Printed with permission from Sharkey et al. 1 )
Patients with takotsubo cardiomyopathy typically present in a similar manner to a patient with a myocardial infarction. Chest pain is the most common symptom among this group of patients. In a study done by the European Society of Echocardiography, chest pain was reported in 185 of 273 patients. 5 Less common symptoms include dyspnea, arrhythmias, and cardiogenic shock. Upon evaluation, patients are often found to have ECG changes such as ST-elevation and T-wave inversion. Most patients will have incurred a stressful event preceding medical attention. Based on the presenting symptoms, laboratory work often shows abnormal cardiac enzymes such as those found in the patient presented (creatinine kinase, troponin T). Characteristically, takotsubo cardiomyopathy patients will show high levels of brain natriuretic peptide (BNP), a substance that is secreted from the heart in response to pressure changes that occur in heart failure. 7 Although high levels of BNP can be due to a variety of causes, such as kidney disease, high levels are also frequently seen in patients with a myocardial infarction. Although most takotsubo patients will not show evidence of coronary blockage on an angiogram, there is no clinical reason that a patient with known coronary artery disease could not also be at risk for takotsubo cardiomyopathy. 14 Based on the typical laboratory findings and their association with an acute myocardial infarction, patients are almost always tested further to evaluate the coronary arteries. In addition to echocardiography and coronary angiography, LV function is usually also evaluated using ventriculography.5,15
The Mayo Clinic has developed criteria to classify takotsubo cardiomyopathy. 16 This proposed criteria for the diagnosis of takotsubo cardiomyopathy is now referenced throughout the literature and is the standard used to diagnosis and classify takotsubo cardiomyopathy (Table 1).7,14,17–19
Mayo Clinic Diagnostic Criteria for Takotsubo Cardiomyopathy (Apical Ballooning Syndrome). a
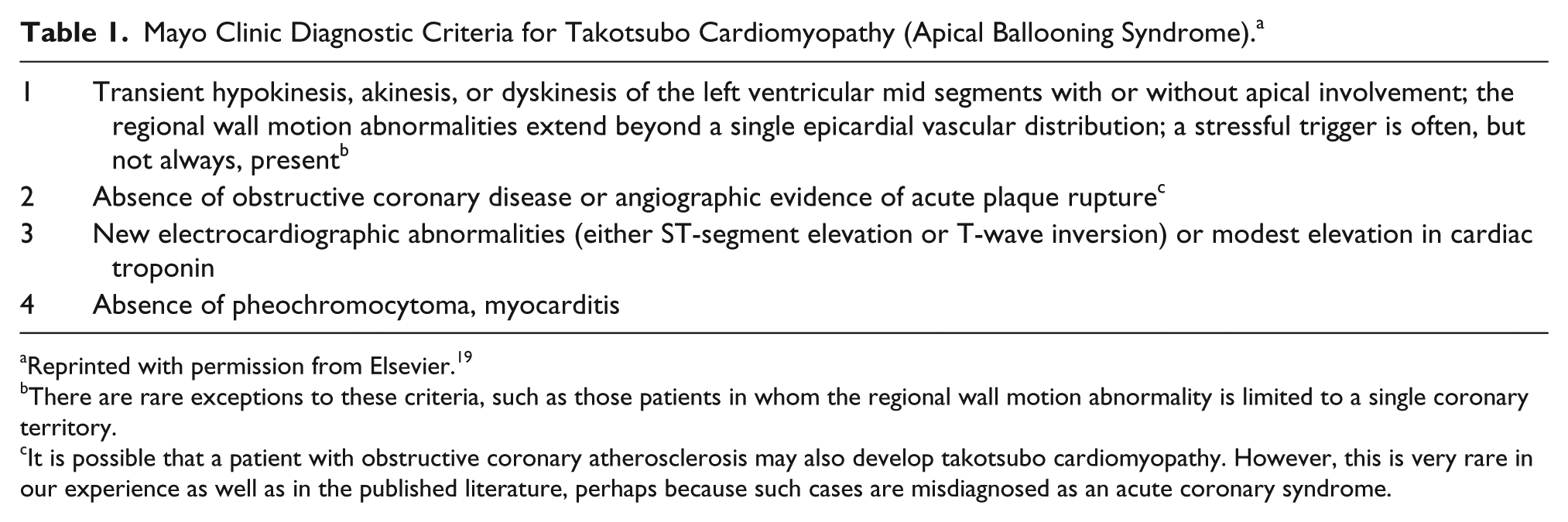
Reprinted with permission from Elsevier. 19
There are rare exceptions to these criteria, such as those patients in whom the regional wall motion abnormality is limited to a single coronary territory.
It is possible that a patient with obstructive coronary atherosclerosis may also develop takotsubo cardiomyopathy. However, this is very rare in our experience as well as in the published literature, perhaps because such cases are misdiagnosed as an acute coronary syndrome.
Another commonly used name for takotsubo is apical ballooning syndrome, which is how it presents on echocardiography.4,5 The classic appearance in real-time of takotsubo is apical or mid-ventricular akinesis. The septal region and base of the heart are spared, whereas the right ventricular function remains intact. 17 In a study by Hurst et al, 14 as many as 40% of takotsubo patients demonstrated a mid-ventricular variant. Although the apical ballooning is transient, the LV function appears low during the peak cardiomyopathy period. Overall, however, echocardiography has been underused and, many times, only represented in case studies. Serial echocardiograms can be done as noninvasive, low-cost examinations to track the LV changes and monitor any complications that patients may have. Successful studies have also been documented to demonstrate coronary flow reserve using Doppler transthoracic echocardiography. 20 By using this technique, transient left apical ballooning syndrome can be evaluated to prove that acute transient microcirculatory damage may have caused the akinesis and ballooning.
The majority of patients diagnosed with takotsubo cardiomyopathy have an excellent prognosis. Patients are initially treated similarly to a patient with an acute myocardial infarction. 14 At this time, there are not any evidence-based guidelines for treatment. 15 There also is much debate on what type of medication should be used on this particular group of patients. Some experts recommend beta blockers and angiotensin-converting-enzyme inhibitors to reduce the effects of adrenaline and to decrease contractility. 14 Diuretics are often used to decrease fluid volume, and blood thinners are administered to decrease the risk of thrombus.
Although prognosis for takotsubo cardiomyopathy is excellent, it is not completely without complications. With decreased LV function, thrombus is always a concern. As with this case study, complications become more prevalent if the patient has additional cardiac anomalies. Dysrhythmias, cardiogenic shock, and death are less common side effects, although mortality is rare. 5 It is believed that dysrhythmias such as atrial and ventricular dysrhythmias are due to the high levels of circulating catecholamines. The report by Gianni et al 5 showed that out of 286 patients, only 3 were in-hospital mortalities. The study by Brinjikji et al 21 showed an in-hospital mortality of 4.2%. Most abnormalities in systolic function and wall motion return to a normal state with complete recovery in less than 2 months.5,6,15
Conclusion
Although takotsubo cardiomyopathy was described more than 20 years ago, uncertainty in its diagnosis and management persists. Most patients present with chest pain and are characteristically treated for a myocardial infarction until the correct diagnosis is made. With angiography and echocardiography, an accurate diagnosis can be made in a timely manner to assist physicians with patient care. Recovery remains a positive outcome, but with all cardiac events, complications still arise and should be treated with the greatest of care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.