
Abstract
Takotsubo Syndrome (TTS) is a condition of transient left ventricular dysfunction that is typically triggered by emotional or physical stress. Since first described in Japan in 1990, it has increasingly been recognised in clinical practice, accounting for up to 2% of Acute Coronary Syndrome (ACS) presentations. In fact, the clinical presentation can be indistinguishable from a myocardial infarction. Although current evidence suggests a catecholamine induced myocardial stunning, the pathophysiological mechanisms remain unknown. Interestingly, it is more common in woman, particularly those who are post-menopausal. This review aims to summarise the current research and provide an overview of the diagnostic strategies and treatment options.
Introduction
Takotsubo Syndrome (TTS) – also known as Takotsubo Cardiomyopathy, stress-induced cardiomyopathy, transient apical ballooning and broken heart syndrome – is a condition that is generally triggered by emotional or physical stress and characterised by transient regional left ventricular (LV) systolic dysfunction. First described in Japan, the term Takotsubo is taken from the Japanese word meaning octopus trap due to the characteristic apical ballooning appearance of the left ventricle. Clinically, individuals present with chest pain with electrocardiographic changes, troponin elevation and left ventricular dysfunction mimicking acute myocardial infarction but in the absence of obstructive coronary artery disease or plaque rapture. 1 In most cases, the regional wall motion abnormality extends beyond one territory and not limited to a single epicardial coronary artery. Most recently, the European Society of Cardiology (ESC) released the first international expert consensus outlining a step wise diagnostic algorithm.
This review will consolidate our current understanding to describe the pathophysiology, diagnostic features including the emerging role of Cardiac Magnetic Resonance (CMR) imaging, current therapeutic strategies and the clinical outcomes of this interesting condition.
Epidemiology
TTS was first described in Japan over 30 years ago but in recent years, improved clinical awareness and widespread access to coronary angiography has led to an increase in diagnosis.2,3 Overall, TTS has been reported in approximately 1% to 2% of all ‘troponin-positive’ suspected ACS presentations 4 and almost 6% of all women presenting with suspected STEMI who undergo urgent angiography. 5
Some reports have suggested that with increasing rates of stress and anxiety experienced in some western populations, the true incidence of TTS may be higher than reported.6,7 In fact, several reports have documented more cases following natural disasters such as those that occurred in Japan, 8 New Zealand 9 and the United States. 10 More recently, the contribution of societal stress has been highlighted during the Corona Virus Disease (COVID) -19 pandemic where social isolation, financial stress and psychological anxiety has led to a significant (3-4x) increase in the incidence of TTS when compared with pre-pandemic incidence. 11
Globally, TTS occurs predominantly in older adults and more commonly in women, particularly those post-menopausal. Interestingly, in western countries, TTS is 9-times more prevalent in women compared to Japan where TTS is more commonly diagnosed in men.12-14 The large majority of patients (>80%) are 50 years of age and older at the time of diagnosis 13 ; women older than 55 years of age are 5x more likely to develop TTS than younger women.15-17
Pathophysiology
The precise pathophysiology of TTS has not been completely elucidated although a number of different mechanisms have been proposed that result in direct and indirect myocardial damage from catecholamine excess, however none offer a complete explanation.18-21 In fact, it is likely that a number of separate pathophysiological mechanisms and pathways may act individually or in an collective manner. 21 One suggestion unifying these separate pathophysiological hypotheses centres on the activation of the sympathetic nervous system stimulating the release of adrenaline from the adrenal glands leading to coronary vasospasm, microvascular dysfunction, acute myocardial dysfunction and inflammation.
The role and consequences of catecholamines
The role of catecholamines has been extensively implicated in the pathophysiology of TTS, highlighted by the fact that episodes are often triggered by emotional or physically stressful situations.13,22 Evidence exists that supports this hypothesis of catecholamine excess being essential in the pathophysiology of TTS. Serum catecholamine levels in patients with TTS are significantly higher than patients with myocardial infarction and heart failure, and remain elevated for a longer period of time.18,23 In addition, elevated levels of noradrenaline levels have been found in the coronary sinus of patients with TTS, suggesting an increase in the local release of myocardial catecholamines. 24 Conditions that are known to cause catecholamine excess – such as pheochromocytoma and subarachnoid haemorrhage (via sympathetic stimulation) – are associated with TTS 25 and are included as part of the InterTAK diagnostic criteria. 26 Furthermore, administration of catecholamines (adrenaline and noradrenaline) and β-adrenoreceptor (βAR) agonists such as salbutamol have been demonstrated to directly trigger episodes of TTS.19,20,23,27-29
The exact mechanism causing the unique regional ballooning patterns remains unknown but it has been postulated that catecholamines have a role in macrovascular and microvascular dysfunction. 21 Supporting this hypothesis, coronary vasospasm has been noted during invasive angiography in patients with TTS. 21 In addition, elevated catecholamines have also been linked to coronary spasm in the microcirculation leading to further myocardial injury. 20 This is further compounded by the effect of the sympathetic nervous systems on increasing cardiac workload leading to supply-demand mismatch. In both epicardial and microvascular spasm studies, administration of intracoronary adenosine has demonstrated improvement.30-33 Of note, the microcirculatory dysfunction has been shown to be transient and correlating with improvement in myocardial function however, it is unclear if the macro- and microvascular dysfunction observed are causal, or the result of the TTS episode. 21 One study of 101 patients identified that patients with coronary slow flow (CSF), thought to be secondary to microvascular dysfunction had worse short and long-term outcomes. Not only did CSF patients have higher rates of in-hospital complications such as acute pulmonary oedema, cardiogenic shock and death from any cause, but at follow up were more than twice as likely to have died compared with those with normal coronary flow, highlighting that CSF and degree of microvascular dysfunction could be a predictor of outcomes. 34
Catecholamine excess may also have a direct effect on cardiomyocyte function, with evidence suggesting either a neurogenic or catecholaminergic stunning phenomenon 21 resulting in arrythmias and irreversible cellular injury. This occurs via calcium overload, reactive oxidative species production, and mitochondrial dysfunction following the activation of βARs. This is supported by mammalian studies that showed the highest density of βAR at the LV apex with sympathetic innervation density lowest in this area but highest in the basal left LV area. This is suggestive of the apical myocardium being more sensitive to catecholamines.35-38
The transient nature may represent a protective mechanism in the setting of supraphysiological catecholamine levels, 22 where ‘ischaemic stunning’ can preserve energy by downregulating contractile function allowing the LV to recover. 39 Fluorodeoxyglucose-positron emission tomography (FDG-PET) and T2-weighted cardiac MRI studies (CMR) have demonstrated reduced myocardial metabolism in the area corresponding to WMAs during the acute phase.40-42
Role of inflammation
Myocardial inflammation has been demonstrated in the acute phase, with some evidence of persistence in the subacute and chronic phases contributing to long-term cardiac dysfunction and symptoms. 21 CMR has been used to demonstrate oedema in affected segments during the acute phase, 41 whilst also low-grade features in the chronic phase in a subset of patients. 43 Additionally, there are examples of TTS triggered by patients receiving vaccinations for influenza, as well as cancer treatment with immune checkpoint inhibitors which activate T lymphocytes. This suggests that TTS can be triggered via immune activation and inflammation. 21 Targetting the inflammatory response may be a future avenue of treatment.
Subtypes
There are 4 subtypes of TTS defined by the distribution of wall motion abnormalities (Depicted in Figure 1 below). The InterTAK registry highlighted that the Apical Type was by far the most typical in TTS, but emphasised that other subtypes did exist. 22 The subtypes described are:
Apical ballooning type (81.7%)
Mid ventricular wall motion pattern (14.6%)
Basal wall motion pattern (2.2%)
Focal wall motion pattern (1.5%)

A depiction of the subtypes of Takotsubo syndrome shown during both diastole (left) and systole (middle). The right column depicts diastole in red and systole in white, with the blue lines representing the region of WMA.
Clinical Manifestations
In the acute phase, most patients have typical chest pain indistinguishable from myocardial infarction while others present with heart failure symptoms such as dyspnoea, orthopnoea and/or acute pulmonary oedema or syncope. 44 Alternatively, some patients are asymptomatic with electrocardiogram or biomarker abnormalities detected incidentally in the setting of an acute underlying illness such as sepsis.
Typically, the physical examination is unremarkable but some patients may be diaphoretic, hypotensive and with clinical features of acute heart failure (with or without haemodynamic compromise).45-47 Although rare, mitral regurgitation, brady arrhythmias, ventricular arrhythmias and cardiogenic shock have been reported in addition to LVOT obstruction induced by basal hyperkinesis. 44
Presentation to hospital may be in the context of emotional or physical stress, or occurs in hospital inpatients with other illnesses who develop a sudden deterioration in left ventricular (LV) systolic function, coinciding with ECG changes, elevation in cardiac biomarkers or haemodynamic compromise.44,48
Risk Factors
Despite encountering psychological and physical stressors frequently as a consequence of our daily life, TTS is relatively uncommon. As such it is hypothesised that there exists risk factors which render some people more susceptible to this condition than others. 22
Hormonal
The significantly increased prevalence of TTS in postmenopausal females suggests a potential role that declining oestrogen levels can play in increasing susceptibility in this group. In support of this theory is the noted 5-fold increased risk in women above the age of 55 compared with those younger than 55. 15
It is known that oestrogen improves coronary blood flow at the coronary microcirculatory level 49 so oestrogen deprivation which leads to endothelial dysfunction may be implicated in the observed higher prevalence in postmenopausal women. 20 However, the exact role of oestrogen in the development of TTS needs further investigation and clarification.
Genetic
Recent reports have described familial cases of TTS raising the possibility of a genetic predisposition while others have described genetic heterogeneity implying a potential polygenic basis.50,51 In one study, inducible pluripotent stem cell derived cardiomyocytes (IPSC-CMs) from 4 unrelated patients with a severe TTS phenotype demonstrated a strong and exaggerated catecholamine sensitivity associated with β-adrenergic signal alterations which suggested a genetic predisposition to catecholamine excess. 27
Psychiatric disorders
There is a strong association between pre-existing psychiatric illness and TTS, in particular anxiety, depression and chronic stress.52-54 When matched for age and sex, psychiatric and other neurological disorders were much higher in the TTS patients when compared to those with ACS. 54
Triggers
The onset of symptoms in a majority of TTS cases is usually preceded by an identifiable acute emotional or physical stressor, or a combination of both. 29 Among 1759 patients in the International Takotsubo Registry study, 36% had a physical trigger, 28% reported an emotional trigger and 8% had both. 26 In up to one third of patients a trigger is not identified however an absence of one does not exclude the diagnosis. Reported stressors can include emotional triggers such as bereavement, gambling and financial losses, arguments, domestic abuse, anxiety related to public speaking and fear, including anticipated fear of medical procedures; whilst physical triggers include pain, sepsis, respiratory failure, post-surgical and malignancy.29,44,55
Whilst mainly secondary to negative or unpleasant emotions and experiences, pleasant emotional stressors have also been observed to trigger TTS, aptly dubbed the “Happy Heart Syndrome”. 56
Patients with an emotional trigger are more likely to be female, present with typical chest pain, and remain hemodynamically stable. In contrast, patients with physical triggers may present with atypical symptoms such as dyspnoea or atypical chest pain, and are more likely to be haemodynamically unstable with worse left ventricular function at presentation, higher incidence of cardiogenic shock requiring mechanical or inotropic/vasopressor support. 57 Patents with physical triggers typically have a higher prevalence of cardiovascular risk factors and other underlying comorbidities.13,58
Diagnostic Evaluation
TTS can be difficult to diagnose as the clinical presentation is often similar to acute myocardial infarction. As such, TTS should be considered as a differential diagnosis in any patient presenting with chest pain and possible ACS, particularly when accompanied by a preceding intense emotional or physical stress or illness.
Over the years, a number of diagnostic criteria have been developed, with the most recent being the InterTAK Diagnostic Criteria (Table 1 below) developed by the Takotsubo International Registry. 26 The most significant changes from the preceding modified Mayo Clinic criteria acknowledges that significant coronary artery disease can co-exist with TTS and is not mutually exclusive, and that while an absence of pheochromocytoma was previously required, the InterTAK diagnostic criteria acknowledge that pheochromocytoma may function as a trigger for TTS.
International Takotsubo (InterTAK) diagnostic criteria.

Source: Adapted from Ghadri et al. 22
Wall motion abnormalities may remain for a prolonged period of time or documentation of recovery may not be possible. For example, death before evidence of recovery is captured.
Cardiac magnetic resonance imaging is recommended to exclude infectious myocarditis and diagnosis confirmation of takotsubo syndrome.
A diagnosis of TTS is more likely in institutions with primary percutaneous intervention (PCI) for ST elevation myocardial infarction and non-ST elevation myocardial infarction (NSTEMI) who undergo early invasive management. Therefore, a high index of suspicion is required for non-intervention facilities with first line fibrinolysis for STEMI; however suspicion for TTS should not preclude administrating fibrinolytic therapy when indicated. 44
Investigations
Electrocardiogram
Electrocardiographic (ECG) should be performed in any patient with chest pain or suspicion of TTS. The priority should be identifying those patients who require urgent coronary angiography. Most patients with TTS have an abnormal ECG with ST-segment elevation and/or T-wave inversion.48,59 Similar to acute myocardial infarction the ECG in TTS can demonstrate localised and dynamic ischaemic changes that evolve over time.
ST-segment elevation was previously reported to be present in up to 80% of TTS cases, however this may be an overrepresentation as these patients are more likely to undergo diagnostic coronary angiography.4,47 Other features of myocardial infarction have also been noted, such as transient Q waves and flattening T waves with the return of prominence. 47 The ECG may be unremarkable with non-specific changes noted (see Table 3).
Regardless of ECG findings, the majority of patients will develop QT prolongation that normalise within 48 hours. 18 Q wave abnormalities typically resolve with restoration of normal R-wave progression before discharge from hospital while T-wave inversion may take longer if at all.
One group has proposed an ECG criteria to distinguish TTS from acute myocardial infarction that includes absent abnormal Q waves, absent reciprocal changes, lack of ST-elevation in lead V1, and the presence of ST-elevation in AVR. The authors found these features to have a 91% Sensitivity and 96% specificity for TTS. 60
Laboratory tests
Cardiac biomarkers of myocardial necrosis, such as Troponin I, Troponin T and Creatinine kinase (CK) are normally elevated with levels comparable to patients with acute myocardial infarction.13,48 Troponin levels usually peak within 24 hours but are deemed to be mild in contrast to the dramatic ECG changes, severe wall motion abnormalities and possible haemodynamic instability that can be encountered (See Table 3). 44
Plasma B-Type natriuretic peptide (BNP) and N-terminal prohormone of brain natriuretic peptide (NT-pro BNP) concentrations have been found to be elevated in the acute phase of presentation, likely reflecting stretch in the ventricular wall and degree of left ventricular impairment. These levels peak within 48 hours of symptom onset and gradually normalise over the next few months of presentation. 59
Coronary angiography
Coronary angiography has an important role in the diagnosis of TTS, in particular for those with ST-segment elevation. TTS is commonly diagnosed with coronary angiography and left ventriculography that shows akinesis of the mid and apical LV segments and hyperdynamic basal segments4,18,29,44,47,55 (Figure 2). Patients may have angiographically normal coronary arteries, or findings of atherosclerosis that is incongruent with the degree of LV dysfunction or regional wall-motion abnormalities demonstrated. In addition, invasive haemodynamic assessment can be used to assess for end-diastolic pressure (LVEDP), and the presence of a pressure-gradient in the outflow trac. Left ventricular outflow tract obstruction (LVOTO) is present in approximately 20% of patients with TTS and has implications for management(see below),48,61 while LVEDP has been shown to be a good predictor of patients likely to have in-hospital complications. 62
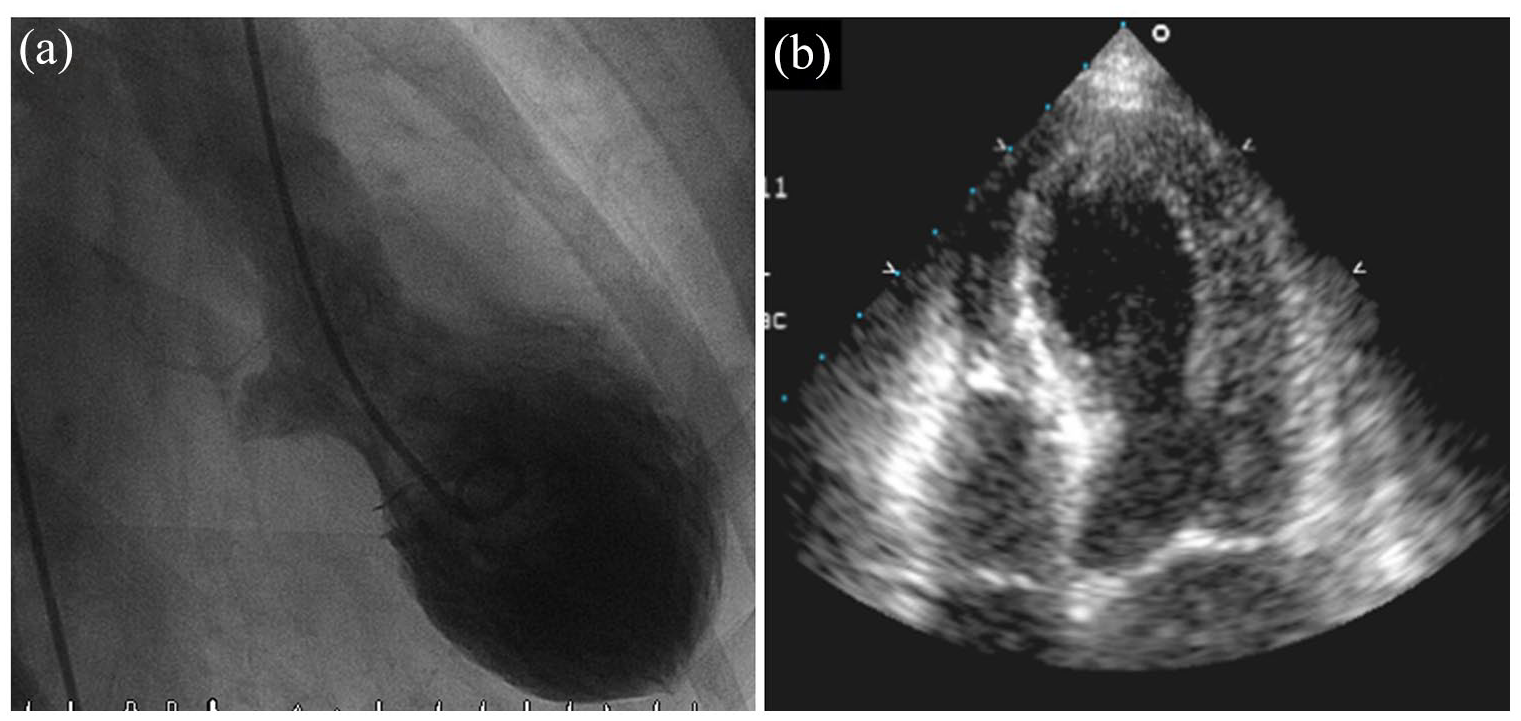
(a) Left ventriculogram right anterior oblique projection in end-systole demonstrating apical ballooning. (b) Four chamber transthoracic echocardiogram in end systole demonstrating apical ballooning. The area around the apex shows akinesis, and the basal segments display hypercontraction.
Echocardiography
Transthoracic echocardiography (TTE) is often the first imaging modality utilised in the acute phase of TTS and typically shows apical and mid ventricular wall motion abnormalities that appear akinetic or dyskinetic compared to the basal segments, giving the appearance of ‘apical ballooning’. 32 Typically, the wall motion abnormality is not limited to one arterial territory differentiating it from acute myocardial infarction (See Table 3).
In the initial phase of TTS, LV function is reduced, however this dysfunction recovers with the resolution of myocardial stunning. 44 Serial TTE is used in the recovery phase to monitor the improvement in LV function, with resolution seen on average by Day 18. 44
TTE is also important in identifying acute complications of TTS, such as left ventricular thrombus formation due to apical dysfunction, 63 mitral regurgitation (from leaflet tethering or papillary muscle dysfunction), dynamic left ventricular outflow tract obstruction due to basal hyperkinesia 45 and in rare cases, ventricular rupture. 64
Cardiac computed tomography angiography
TTS is associated with several triggers such as intracranial bleeding, terminal malignancy and septic shock where invasive coronary angiography may not be appropriate. In these cases and those with low suspicion of ACS, previous TTS and established coronary anatomy on prior recent angiography, computed tomography coronary angiography (CTCA) may be more appropriate. 48
Cardiac magnetic resonance imaging (CMR)
CMR imaging has been previously used in those with atypical features, bystander coronary artery disease or when there is suspicion for myocarditis. 65 There is emerging evidence that routine use, particularly in the acute phase, assists in confirming the diagnosis, as well as identification of complications not evident on other imaging modalities.32,48
In the acute phase, reversible myocardial inflammation and oedema are hallmark findings of TTS22,66 and can be readily assessed with CMR through the utilisation of T2-weighted sequences.22,48,65-68 In TTS, myocardial oedema is typical transmural and has been shown to resolve in six months.41,67,69 In the sub-acute phase, identifying subtle RWMAs makes CMR the ideal modality to accurately assess for resolution of regional dysfunction, with full-recovery being critical in confirming the diagnosis. 22
Additionally, late gadolinium enhanced imaging (LGE) can be used as an important discriminator to assist in diagnosing TTS. Whilst previously believed that an absence of LGE on CMR was critical for TTS, more recently LGE has been noted in the acute phase of patients with TTS in a transmural distribution appearing at the hinge points between the dyskinetic ballooning segments and the hypercontractile segments.69-71 LGE in this setting is transient and resolves on serial imaging to confirm the diagnosis of TTS. Presence of LGE in the acute setting has been associated with increased incidence cardiogenic shock and a longer timeframe for resolution of wall motion abnormalities.32,72 In comparison, patients with myocardial infarction will have focal sub-endocardial or transmural LGE evident, while those with myocarditis typically will have a mid-wall distribution of LGE. 42
CMR has been shown to be highly accurate in diagnosing TTS and useful in excluding other aetiologies that can present with similar biochemical, echocardiographic and angiographical findings such as myocarditis or myocardial infarction. 42 In one recent study, 148 patients with myocardial infarction and non-obstructed coronary artery disease (MINOCA) underwent CMR imaging within five days of presentation. The authors found that 35% of patients had TTS despite no apparent prior evidence on TTE or ventriculography. 73 Additionally, CMR has superior tissue characterisation and higher special resolution than TTE allowing it to better assess RWMAs beyond a single coronary artery distrubtion.48,74 Furthermore, CMR is the modality of choice in assessing the RV and although it was initially thought that TTS only affected the LV, with increasing use of CMR imaging, studies have found RV involvement in some cases41,66,67
Finally, ventricular and apical thrombi that are often not able to be visualised on TTE can be seen during early Gadolinium (EGE) sequences. These thrombi will appear as a low signal intensity without gadolinium uptake, in comparison to the high intensity signal from the blood pool.67,69
InterTAK diagnostic score and algorithm
To assist in identifying the likelihood of TTS and attempt to distinguish patients from ACS, the Takotsubo International Registry have produced a novel scoring system called the InterTAK Diagnostic Score 26 (see Table 2). This score is simple to use, can be calculated at the bedside in the emergency setting as it utilises 7 easily identifiable parameters that do not require additional imaging modalities. 48 It has been demonstrated to have a high sensitivity in diagnosis of TTS and has been showed to discriminate TTS from ACS with high specificity. 26
InterTAK diagnostic score. 26

Comparing diagnostic features of Takotsubo syndrome, ST-elevation acute coronary syndrome, non-ST-elevation acute coronary syndrome and myocarditis.

Abbreviations: +, mild elevation; ++, moderate elevation; +++, severe elevation; CAD, coronary artery disease; LGE, late gadolinium enhancement; WMA, wall motion abnormality.
The InterTAK diagnostic score can be used in conjunction with the International Expert Consensus Document on Takotsubo Syndrome 48 diagnostic algorithm for assessment of patients presenting with chest pain and/or dyspnoea for whom TTS is suspected.
Management
To date, there are no established guidelines for the treatment of TTS, and hence the optimal management relies on expert consensus based on retrospective analysis.
Acute management
TTS is generally transient and can be managed with supportive therapy in most cases. However some patients develop acute complications such as Cardiogenic Shock (CS) and acute heart failure that require intensive therapy. Most importantly, the immediate management should be directed towards excluding and treating possible ACS, with the administration of antiplatelet agents, anticoagulation, vasodilators and continuous ECG monitoring, as well as planning towards urgent/semi-urgent coronary angiography.
CS is common and has been reported in up to 10% of cases 13 associated with a 5-fold increase in mortality. 75 Unfortunately, managing CS in this setting is dependent on the presence of LVOT obstruction so before any management is implemented, LVOT pressure gradients should be quantified either with Doppler echocardiography or invasive angiography 48 However, due to elevated levels of catecholamine the use of exogenous catecholamines should be limited and used only as a bridge to further treatment such as mechanical support. Levosimendan is a calcium sensitiser and has been shown to have some benefit in these patients and should be considered first when transitioning from catecholamine inotropic agents. 76 Due to the cost and limited availability, levosimendan may be limited resource-poor settings. On the other hand, in patients with significant LVOT obstruction, inotropes are contraindicated and should not be used as they may worsen the degree of obstruction and shock. In these patients, intravenous fluid resuscitation and short acting beta-blocker therapy, may help improve CS and resolve the LVOT obstruction. The use of diuretics, nitroglycerin or insertion of an intraaortic balloon pump should be avoided. In patients with refractory LV dysfunction with LVOT obstruction, mechanical circulatory support can be considered.29,48
Acute heart failure management is driven by guideline directed therapy and includes a combination of Angiotensin enzyme inhibitor (ACEI) or Angiotensin II receptor blocker (ARB), beta blockers ± diuretics and nitroglycerin to reduce ventricular filling pressures (in the absence of significant LVOT obstruction).44-46 Beta blockers have been proposed to add further benefit of blunting the effect of catecholamine excess, 48 and preventing cardiac rupture. 59 Their use, however, should be used cautiously in patients with bradycardia and QTc >500 ms, due to the potential for pause-dependent torsades de pointes. 48 There are no specific recommendations for anti-platelets in TTS in the absence of coronary artery disease.16,44
Left ventricular thrombus formation
The potential risk of intraventricular thrombus formation and systemic embolisation should be addressed in patients with severe LV systolic dysfunction. TTE or CMR should be used to evaluate for LV thrombus. While LV thrombus is said to complicate 1% to 2% of TTS patients, routine prophylactic anticoagulation is not recommended,16,77 but should be considered in patients with severe LV systolic dysfunction that is slow to recover functionally to reduce the risk of thromboembolism. 48
When considering TTS patients with known LV thrombus, the role of anticoagulation to prevent further embolisation and thrombus progression is extrapolated from observational studies in the myocardial infarction population. Recommendations in that population suggest a period of therapeutic anticoagulation for 3 months. In TTS patients with LV thrombus anticoagulation duration should be continued for at least 3 months, or until LV function has resolved. 48
Long term management
Complete recovery is an essential part of the diagnosis of TTS and can occur within a few days or can take several weeks. 47 As TTS is a transient condition, left ventricular failure therapy with ACEI/ARB, Beta blocker and diuretics (as required) should continue for a minimum of 3 months, or until left ventricular function has recovered. 63 In the case that the underlying process was an irreversible cardiomyopathy rather than TTS, appropriate heart failure medication would have already been commenced.
While the use of ACEI or ARB in the International Takotsubo Registry demonstrated improved survival at 1-year-follow up and was associated with a lower prevalence of TTS recurrence, there was no survival benefit or reduction in recurrence seen in those on beta-blocker therapy despite the proposed catecholamine blunting effect. Given the low recurrence rate, and conflicting results in other studies78,79 the significance of these findings requires further investigation and validation. Aspirin and statin therapy should be given for secondary prevention in patients who have co-existing coronary artery disease 48
Clinical outcomes and prognosis
Despite the transient nature of LV dysfunction, traditional views of TTS being a benign syndrome may be misguided and underestimate the risk of in-hospital complications. In the acute phase, hospital complications are comparable to ACS patients in composite cardiovascular endpoints such as cardiogenic shock, catecholamine use, the need for invasive or non-invasive ventilation, cardiopulmonary resuscitation, and death(19.1% vs 19.3% respectively). 77 There is some evidence of long-lasting clinical consequences with subclinical cardiac dysfunction, 43 and rate of recurrence at approximately 5% occurring between 3 weeks and 3.8 years post event.77,80 The InterTAK registry found that long-term mortality outcomes were, overall, similar between TTS and ACS patients. 58 However, in this group, patients whose TTS was triggered by emotional stress had favourable both short- and long-term prognosis. The long-term mortality in patients whose trigger was from physical activity, medical conditions or procedures was up to 3 times higher compared with emotional triggers, whilst those with neurological disorders were almost 6 times higher. Whilst this likely represents the long-term mortality being a reflection of the underlying disease prognosis and associated comorbidities, further studies are warranted.
Stroke or transient ischaemic attack rate of 1.7% per patient-year has been reported in 1 registry, 32 with Some advocating the use of the CHA2DS2VASc score to predict the incidence of cerebrovascular events and anticoagulate as appropriate. 81
An approach to the patient with suspected Takotsubo syndrome
In the evaluation of patients with clinical suspicion of TTS, the diagnosis should only be made after excluding an acute coronary syndrome. As per the proposed algorithm in Figure 3, all patients with chest pain and/or dyspnoea should be evaluated with an ECG and for those without ST-elevation, the InterTAK Diagnostic score should be performed. In these patients, TTE should evaluate for apical, midventricular or basal ballooning with circumferential pattern and potential complications such as LVOT obstruction, RV involvement, significant MR or ventricular thrombus. Based on the clinical situation, patients should be evaluated with either CT-CA or invasive coronary angiography. In cases with no identifiable diagnosis, MINOCA or co-existing CAD, CMR with LGE should be performed within 5 days to confirm the diagnosis or identify possible mimics such as of acute myocarditis or myocardial infarction. For those diagnosed with TTS, treatment with an ACE-I and beta blocker therapy should be started for at least 3 months. When RWMAs have not resolved, CMR should be considered to evaluate for alternative diagnoses. Heart failure and complications identified are treated as per Figure 4.
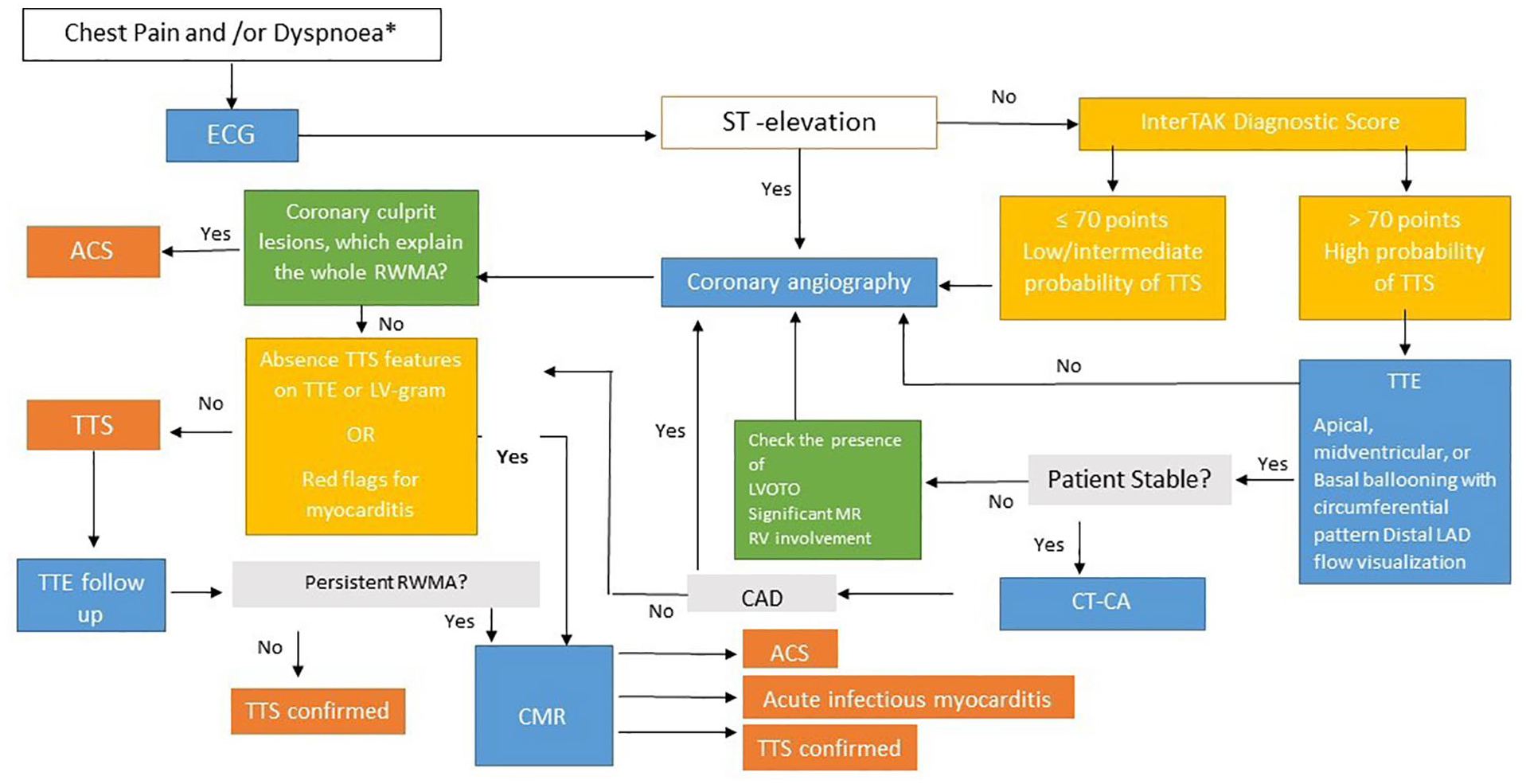
Proposed diagnostic algorithm for patients presenting with chest pain or dyspnoea.
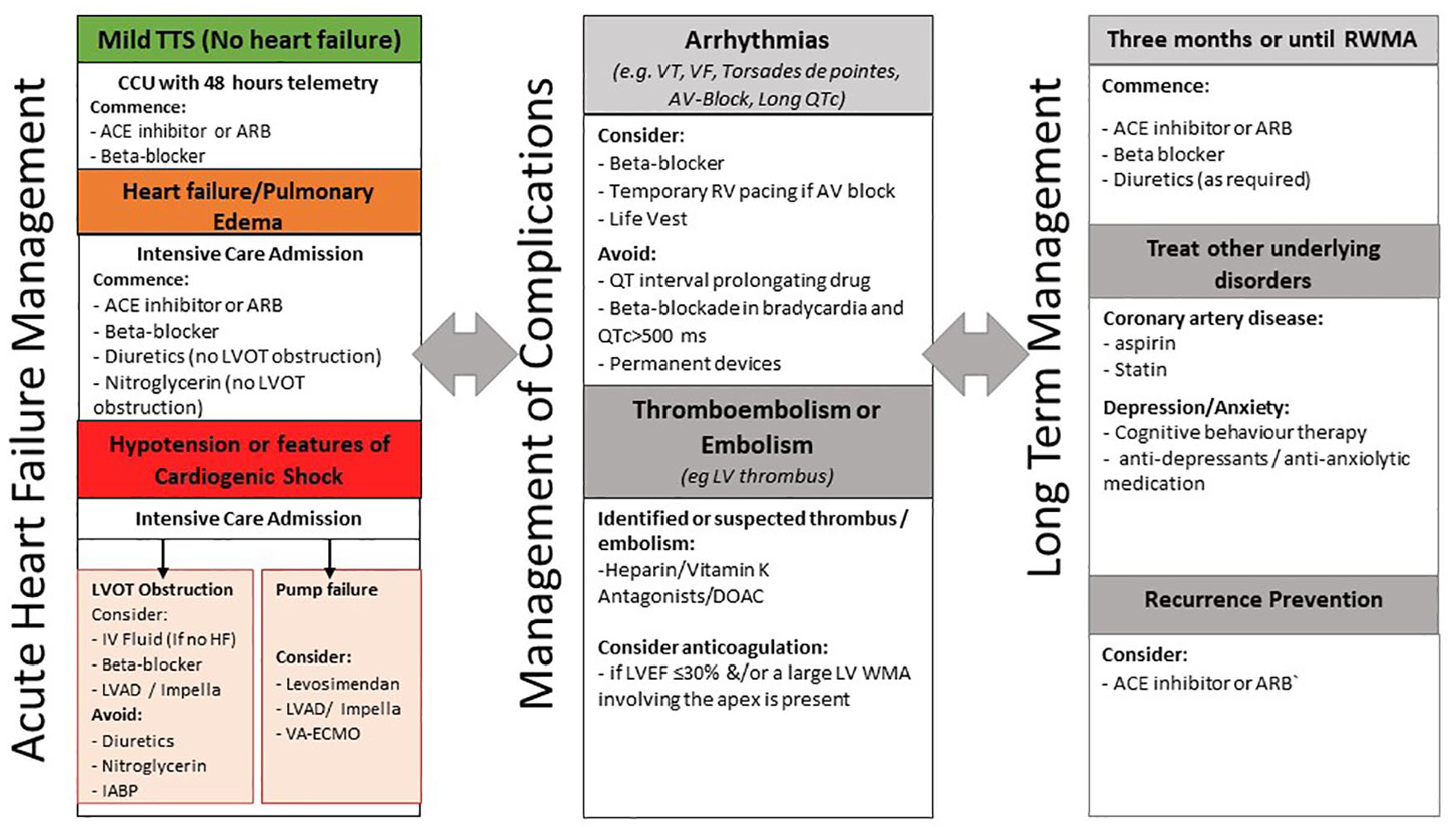
Management of takotsubo syndrome. Reproduced from international expert consensus document on takotsubo syndrome (part II): diagnostic workup, outcome and management.
Conclusion
Takotsubo Syndrome is an increasingly recognised condition characterised by transient LV dysfunction in the absence of significant obstructive coronary artery disease. Signs and symptoms can mimic those of acute coronary syndrome including electrocardiography changes, raised cardiac biomarkers and clinical symptoms of chest pain, dyspnoea or syncope. While the pathogenesis is not completely understood, proposed mechanisms appear to correlate with catecholamine excess in the setting of stressful triggers. The role of CMR in both diagnosis and identification of complications is currently underutilised but shows extreme promise and should be utilised in all patients where resources allow.
It is increasingly recognised that TTS is not a benign condition and can be associated with significant event rates similar to those of acute coronary syndrome. Treatment modalities in the acute setting are largely focussed on excluding acute myocardial infarction and supportive care for the subsequent LV dysfunction. Current evidence suggests a role for ACEI and ARBs in the management of TTS with improvement in long-term mortality. Moving forward, larger studies will be necessary to help guide clinicians to treat TTS.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed significantly to the final manuscript