
Abstract
Objective
This study aimed to describe cases of cesarean scar pregnancies that were successfully treated with suction curettage under ultrasound guidance and their outcome.
Methods
This retrospective, descriptive case-series study was performed on 17 patients diagnosed with cesarean scar ectopic pregnancy in Sulaimani Maternity Teaching Hospital from May 2022 to April 2023. The patients’ sociodemographic and clinical data were collected. The patients were treated with suction curettage alone or in combination with local injection of methotrexate under ultrasound guidance.
Results
Patients with a viable fetus (n = 4) received local intrinsic methotrexate injection into the gestational sac and suction curettage, while those in whom the fetus had died (n = 13) underwent only suction curettage. Five patients required intrauterine balloon insertion to stop bleeding without further treatment, and only three required a blood transfusion owing to severe bleeding.
Conclusions
Cesarean scar ectopic pregnancy is a dangerous and complex disorder with an increasing occurrence in recent years. Accurate early diagnosis and effective management are essential to reduce maternal mortality and mortality of this type of pregnancy.
Keywords
Introduction
Cesarean scar pregnancy (CSP) is one of the most severe complications of cesarean delivery, and is defined as gestational sac implant into the hysterotomy site of a previous cesarean delivery. 1 With the increasing rate of cesarean section (C/S), there has been a substantial increase in CSP. The incidence of CSP is 0.15% in those with previous C/S and is 6.1% of all ectopic pregnancies.2,3 Many treatment options have been reported for CSP, including expectant management, medical treatment, uterine artery embolization, surgical intervention, and combination approaches. Recent reviews recommend a minimally invasive method that removes the gestational sac and C/S transvaginal or laparoscopic treatment rather than medical treatment.1,4 Additionally, if CSP is not diagnosed early, there are no unique clinical features at the early stage until serious complications occur, such as bleeding and death. 5 In most cases, CSP has no specific symptom and can be easily misdiagnosed, which can lead to life-threatening hemorrhage during pregnancy or curettage, uterine rupture, disseminated intravascular coagulation, and even death. 6 Undiagnosed CSP can sometimes present with heavy bleeding, hemoperitoneum, and shock after termination of early pregnancy or missed abortion. Therefore, an early and accurate diagnosis of CSP is essential for effective treatment to prevent these catastrophic complications.7,8 Ultrasound is widely used to diagnose CSP, with a sensitivity of 84.6%. 9 The diagnosis of CSP depends on symptoms/clinical manifestations, a history of previous scars, serum beta-human chorionic gonadotropin concentrations, and transvaginal sonography.10,11
Surgical management can be offered to hemodynamically unstable patients, including hysteroscopy, which is an essential mini-invasive strategy for managing this type of pregnancy, together with laparoscopy, laparotomy, and uterine artery embolization. 12 Non-invasive therapy with systemic methotrexate (MTX) may be considered when the gestational age is <8 weeks without fetal cardiac activity. 13 This study aimed to investigate patients with CSP who were successfully treated with suction curettage under ultrasound guidance with local MTX injection for a viable pregnancy.
Patients and methods
This retrospective, descriptive case-series study was conducted on 17 consecutive patients diagnosed with type 1 CSP in their first trimester of pregnancy from May 2022 to April 2023. The patients were at Sulaimani Maternity Teaching Hospital, Sulaimaniyah, Iraq.
Inclusion criteria
Hemodynamically stable women in their first trimester diagnosed with type 1 scar ectopic pregnancy with a history of previous C/S were enrolled in this study.
Questionnaire
A self-created/validated questionnaire (Supplementary data) was used to collect patients’ data, such as sociodemographic features (maternal age, residency, and parity) and clinical features (presenting symptoms, number of previous C/Ss, history of previous miscarriage, fetal age, and fetal heart activity), at the time of presentation.
Ethical considerations
The Scientific and Ethical Committees at the College of Medicine, University of Sulaimani, Sulaimaniyah, Iraq, approved the study protocol (7/23/532). The Institutional Review Board at Sulaimani Maternity Teaching Hospital, Sulaimaniyah, Iraq provided exemption for the patients’ informed consent because of the study’s retrospective nature. The study was conducted in accordance with the Declaration of Helsinki. Additionally, all patients’ details were de-identified and kept confidential.
Study protocol
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14 Women with a positive pregnancy test and prior C/S underwent an early assessment by transvaginal sonography, which was performed by the author (a consultant gynecologist with 20 years of experience). The ultrasound criteria included an empty uterus and cervical canal, a gestational sac at the cesarean scar site, a vascular area at the previous cesarean scar in a Doppler scan, and thin/absent myometrial tissue between the bladder and the gestational sac. 15 The type of CSP was defined as a gestational sac growing towards the uterine cavity, and the thickness of myometrial tissue at the cesarean scar was not <0.3 cm (a thinner myometrium indicates a greater possibility of deep implantation). Consequently, gynecologists (including the author) made the final diagnosis of CSP and decided on the mode of treatment.
Among the studied patients, women who still had a viable fetus in their first trimester underwent a single local injection (intrinsic) of MTX (50 mg/2.0 mL) using a 22-G needle into the gestational sac with an adaptor under transvaginal ultrasound. This injection was followed by suction curettage under ultrasound guidance to aspirate their amniotic fluid and fetal tissue, and their beta-human chorionic gonadotropin concentrations were monitored. The other women with non-viable fetuses underwent only suction evacuation under ultrasound guidance.
Statistical analysis
IBM SPSS (version 26; IBM Corp., Armonk, NY, USA) was used to analyze the data, and descriptive and inferential statistics were used. A p value ≤0.05 was considered statistically significant.
Results
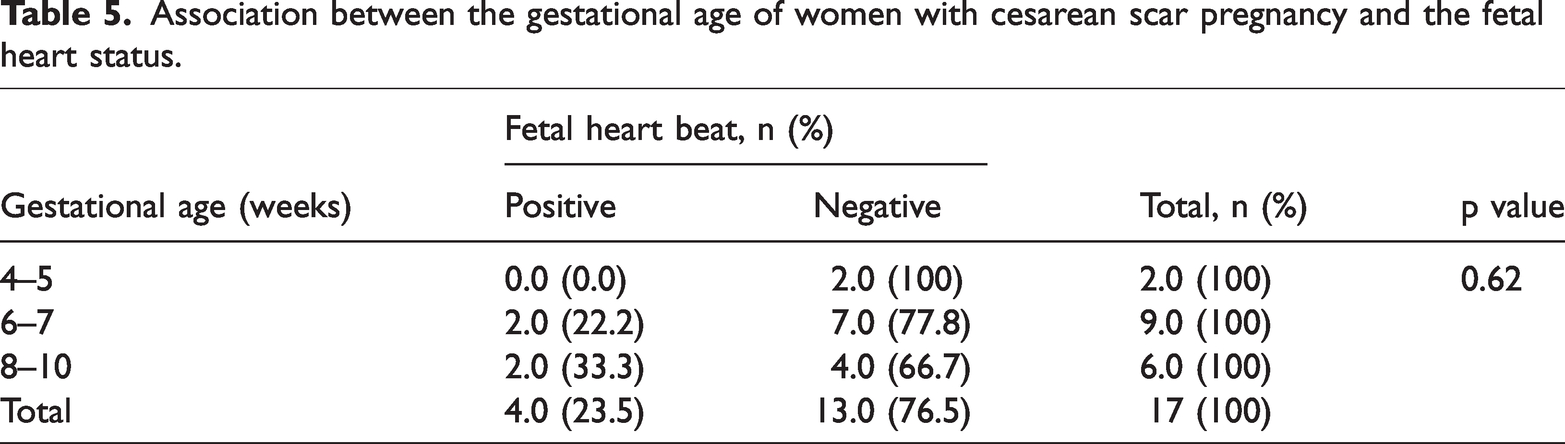
Seventeen patients were studied. The mean maternal age was 34.94 ± 4.93 years, with an age range of 23 to 43 years, while the mean parity was 2.36 ± 1.33 times, with a range of 2 to 6 times. Most patients were from urban areas (Table 1). The most common presenting symptom was a missed period, followed by vaginal bleeding, and then abdominal pain. Regarding a previous history of C/S, five patients had two, seven had three, four had four, and only one had six C/Ss. Additionally, most patients had no previous history of miscarriage (Table 2). Regarding fetal viability, the fetal heart rate could only be detected in four (23.5%) patients, with a gestational age ranging from 4 to 10 weeks, as shown by ultrasound (Table 3). Therefore, these women had local intrinsic MTX injection under ultrasound guidance, while the remaining women underwent suction curettage under ultrasound guidance (Table 4). Among the patients, five had an intrauterine balloon following suction curettage to stop bleeding, and only three patients required a blood transfusion. Using ultrasonography, a non-significant association was observed between fetal heart viability and gestational age (Table 5).
Sociodemographic characteristics of the patients.

Obstetric history of the patients.

Fetal heart status and fetal age of patients with cesarean scar pregnancy.

Treatment approaches used for patients with cesarean scar pregnancy.

Association between the gestational age of women with cesarean scar pregnancy and the fetal heart status.
Discussion
CSP is a rare ectopic pregnancy, and its precise pathophysiology has not been identified yet. however, the most accepted theory is the occurrence of scar dehiscence or defects at the scar site secondary to vascularization deficiencies and fibrosis that compromise healing. 8 To the best of the author’s knowledge, this is the first report on CSP cases in Iraq, their treatment modalities, and outcomes.
Four theories have been hypothesized for the pathophysiology of CSP, the first of which is a low or cervical uterine incision. 16 In the current study, all women had at least one previous C/S, and the majority had at least two previous C/Ss. Additionally, all women had a history of lower segment incisions for their prior C/S, which supports the first theory of the pathophysiology of CSP. 16
Additionally, in this study, women with CSP were diagnosed by transvaginal sonography, and their number increased when their gravidity progressed. Therefore, this finding is likely related to the increased awareness of women when the frequency of their gravidity increases. Consequently, most elective patients were operated on by a senior obstetrician. However, emergent cases were operated on by a registrar obstetrician. The clinical features of patients with CSP are similar to those in patients with cervical and tubal ectopic pregnancies. 10 Only one patient who had a ruptured uterus presented with abdominal pain alone in the current study. however, five (29.4%) women presented with vaginal bleeding. Additionally, 10 women who were diagnosed by ultrasound presented with a missed period, and the interval between the prior scan was only 1 month. Therefore, most CSPs were the endogenous type. CSP is a precursor for a morbidly adherent placenta, which is an obstetric complication caused by the placenta’s invasion of the myometrium. 11 Shamshiraz et al. 17 and Timor-Tritsch et al. 8 suggested elective cesarean hysterectomy without removing the placenta to decrease maternal morbidities. However, suction and aspiration of the CSP for the first and second CSPs and laparotomy to excise the prior scar and repair the uterine wall for the third CSP have been mentioned in the literature.15,18 Curettage is a procedure in which contents from the inside of the uterus are aspirated and removed using suction. This procedure is used primarily as a diagnostic procedure to sample the endometrium, and it may be used to treat incomplete miscarriage. 19 Shen et al. reported that most (70.4%) patients were managed by transcervical aspiration of the gestational sac and open surgeries were used to manage 22.2% of the patients. 10 The remainder of their patients had transcervical aspiration of the gestational sac and MTX (14.8%) or MTX alone (7.4%).
In this study, only women with viable fetuses (n = 4.0) received local intrinsic MTX injections. Levin et al. reported that 80.6% of patients were treated by systemic infusion of MTX, while 19.4% had combined systemic and local MTX treatment. 20 Therefore, MTX therapy is a safe and effective strategy for treating CSP, with favorable subsequent reproductive results and a low conversion rate to surgical management.
There is no uniform guideline for managing CSP. Previous studies have described different approaches for CSP, such as elective cesarean hysterectomy, 11 aspiration of CSP, intra-gestational injection of MTX with or without potassium chloride, 21 and systemic MTX. 22 In the current study, different, less invasive, and patient-tailored methods were used. The risk of CSP increases when the frequency of gravidity increases. Therefore, women should be advised that performing more C/Ss increases the risk of CSP.
Generally, retrospective studies have a lot of bias. Therefore, in this retrospective study, a limitation was the small sample size, which meant that our technique may not be universally applicable to all patients with CSP. Additionally, because of the small sample size, statistical analysis could not be carried for comparison with other techniques. Future larger studies should follow all patients until their last pregnancies to obtain more data.
In conclusion, effective treatment of CSP may be carried out in the first trimester to achieve optimal treatment because CSP can also lead to severe hemorrhage, uterine rupture, and hysterectomy. Therefore, the safety and availability of surgery in the form of ultrasound-guided suction curettage should be fully considered for patients with CSP.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241281692 - Supplemental material for Outcome and treatment of cesarean scar ectopic pregnancy under ultrasound-guided vacuum aspiration
Supplemental material, sj-pdf-1-imr-10.1177_03000605241281692 for Outcome and treatment of cesarean scar ectopic pregnancy under ultrasound-guided vacuum aspiration by Naz Azad Abdullah in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241281692 - Supplemental material for Outcome and treatment of cesarean scar ectopic pregnancy under ultrasound-guided vacuum aspiration
Supplemental material, sj-pdf-2-imr-10.1177_03000605241281692 for Outcome and treatment of cesarean scar ectopic pregnancy under ultrasound-guided vacuum aspiration by Naz Azad Abdullah in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605241281692 - Supplemental material for Outcome and treatment of cesarean scar ectopic pregnancy under ultrasound-guided vacuum aspiration
Supplemental material, sj-pdf-3-imr-10.1177_03000605241281692 for Outcome and treatment of cesarean scar ectopic pregnancy under ultrasound-guided vacuum aspiration by Naz Azad Abdullah in Journal of International Medical Research
Footnotes
Acknowledgements
The author would like to thank the healthcare staff from Sulaimani Maternity Teaching Hospital for their support and assistance in this research.
Author contributions
NAA: Conceptualization, data collection, data analysis, and writing the original manuscript.
Data availability statement
The datasets used and analyzed during the current study are available within the manuscript.
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.