
Abstract
Ectopic thyroid tissue is a rare developmental abnormality. A case is reported here of ectopic thyroid tissue that presented as a midline mass, mimicking a thyroglossal duct cyst. The thyroid gland was not visualized in its normal position. This report highlights the importance of imaging in the preoperative evaluation of a midline neck mass.
Keywords
Introduction
Ectopic thyroid tissue is a rare developmental anomaly in which there is abnormal embryogenesis of the thyroid gland. The thyroid normally descends from the floor of the primitive foregut to reach the final position in front of the trachea in the seventh week of gestation. When the normal migration of the thyroid fails, it results in an ectopic thyroid.1–4 Ectopic thyroid is most common in females, 1 and it is more common in populations of Asian origin. 2 The prevalence is about 1 per 100 000 to 300 000 people. 3 It may occur at any age but is most common at younger ages; in the series of Gopal et al., 2 the mean age at presentation was approximately 14 years. A case is reported in the following of ectopic thyroid tissue presenting as a midline neck mass in a young male mimicking a thyroglossal duct cyst.
Case Report
A 19-year-old man with a provisional diagnosis of thyroglossal duct cyst (TGDC) was referred to the radiology department for sonographic examination. The patient gave a history of a midline neck mass for the past two years. The mass was small to begin with but had increased to its present size in the last few days. There was no history of dysphagia or dyspnea. There was no history suggestive of hypothyroidism or hyperthyroidism. On examination, the general health of the patient was good. A firm midline neck mass in the region of the hyoid, measuring approximately 4 × 3 cm, was seen moving with deglutition and protrusion of the tongue (Figure 1). Routine hematological parameters were within normal limits; thyroid stimulating hormone (TSH) was noted to be elevated at 37.71 mIU/L (normal values, 0.4–5.0 microIU/ml).

Photograph of the patient showing a 3 × 4 cm midline neck mass in the superior aspect of the neck in the region of the hyoid.
Sonography was done using an Esaote My Lab 60 (Esaote Ultrasound, Esaote, Genoa, Italy) with a 4 to 13 MHz broadband linear array transducer. The sonogram showed nonvisualization of the thyroid gland at its normal anatomical position (Figure 2). At the site of the midline mass, an oval-shaped lesion measuring 3.00 × 1.56 × 2.37 cm, extending from midline toward the right, with echogenicity resembling that of the thyroid was seen. Another contiguous rounded lesion was seen to be extending from the aforementioned lesion, from midline toward the left side and measuring 2.40 × 1.90 × 0.75 cm, with heterogenous echogenicity showing a honeycombing pattern (Figure 3). Sonographic image morphology was suggestive of ectopic thyroid. The patient was advised to have a Technetium-99m (99mTc) nuclear thyroid scan so that findings could be confirmed. The thyroid scan showed evidence of increased tracer uptake in the midline mass; no other thyroid tissue was seen (Figure 4). The findings were suggestive of ectopic thyroid gland. A computed tomographic (CT) scan was done to delineate the relationship of the mass to the surrounding structures of the neck (Figure 5).
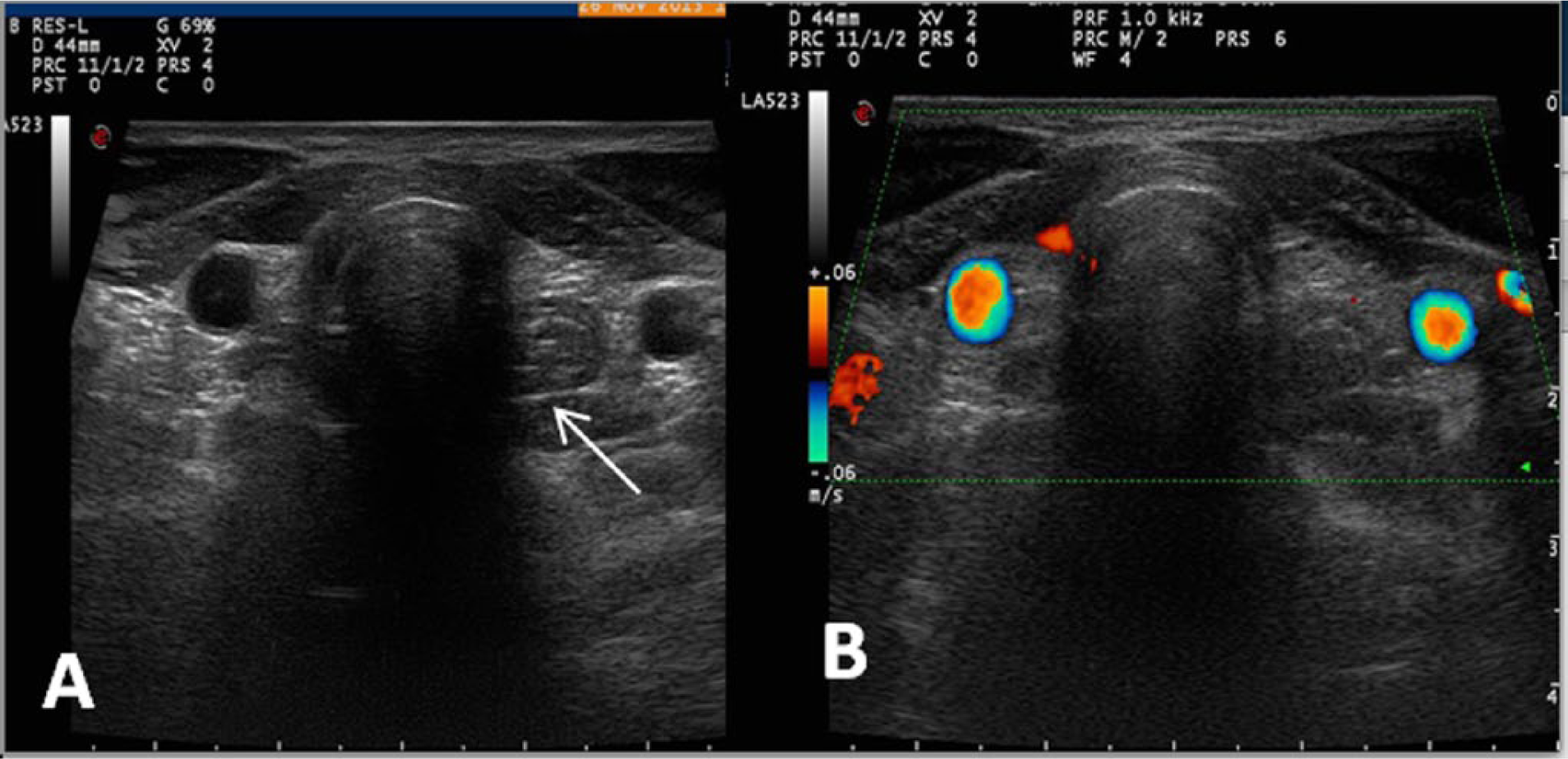
(A) Gray-scale and (B) color Doppler transverse images of the neck showing no thyroid tissue in its normal anatomical position; the arrow points to the esophagus.
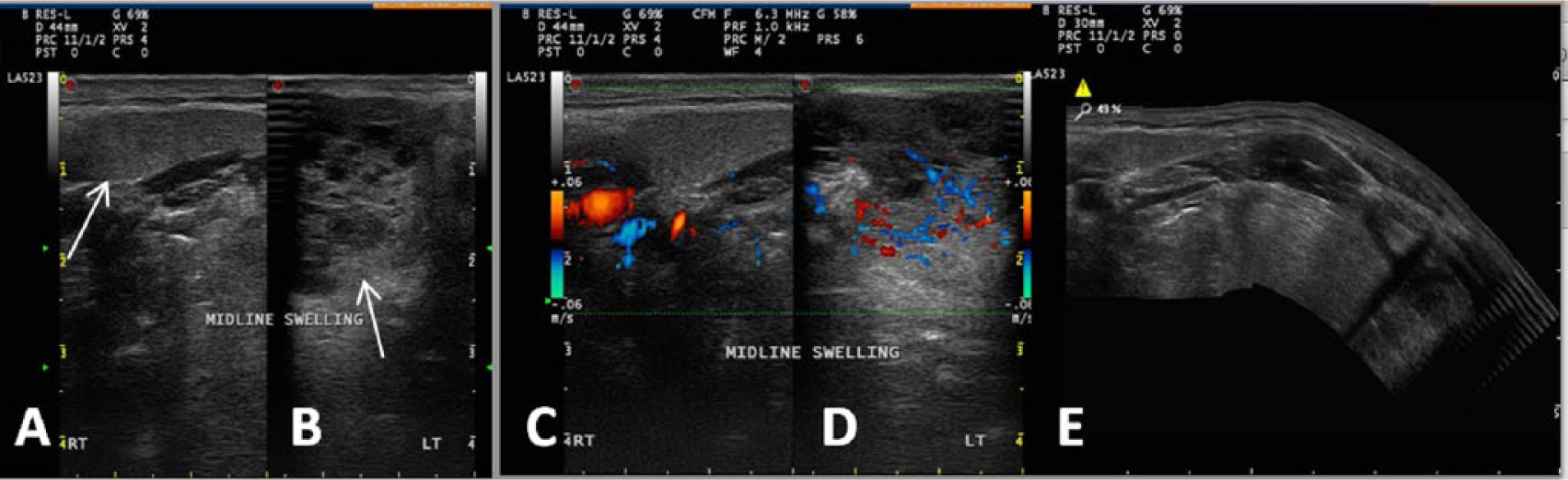
(A, B) Transverse gray-scale and (C, D) color Doppler images of the midline mass showing swelling and edema of the neck near the midline with the mass extending to the right and left of midline (arrows). The lesion extending to the right (A and C) has echogenicity similar to the thyroid; the lesion extending to the left (B and D) shows more of a honeycombing pattern of echogenicity. (E) Extended field of view transverse gray-scale image showing the anatomic relationship of the mass to other structures of the neck.
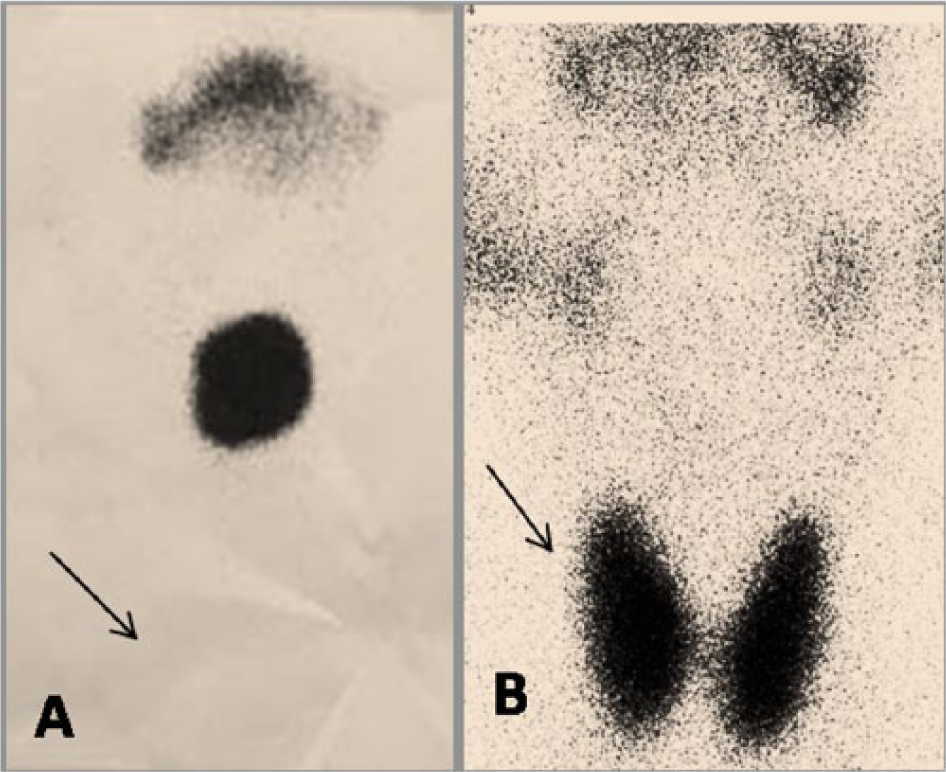
Technetium-99m nuclear scans of the neck showing (A) enhanced uptake by the midline mass with no other uptake noted at the normal site of the thyroid (arrow) and (B) a normal neck scan (in a different patient) for comparison with normal uptake by the thyroid (arrow).

Computed tomographic scan of the neck showing (A) transverse, (B) sagittal, and (C) coronal views of the midline mass (arrows).
Replacement therapy with L-thyroxin, 50 microgm/day, was started, and no surgery was performed. On follow-up after 6 months, the patient was doing well. A repeat TSH measured 1.26 mIU/L, in the normal range. There was also a slight reduction in the size of the mass noted.
Discussion
Ectopic thyroid tissue, defined as thyroid tissue not located antero-laterally to the second and fourth tracheal cartilages, is rare. It was first described by Hickman in 1869. 5 It is a congenital disease caused by abnormal migration of thyroid tissue in the embryonic stage. The embryonic thyroid gland travels through thyroglossal duct to reach its normal position. It may never travel and remain at the base of the tongue, resulting in a “lingual thyroid,” or the descent of the thyroid may not proceed normally, leading to a variety of possible anomalous locations of the gland. In the majority of cases, it is located in the midline, between the foramen caecum and the proper location of the thyroid. 6
Thyroglossal duct cyst (TGDC) is another congenital defect. When the thyroid gland forms during embryonic development, it begins at the base of the tongue and moves down the neck through a canal called the thyroglossal duct. This duct normally disappears once the thyroid reaches its final position in the neck, but sometimes portions of the duct remain. They form cysts, filled with fluid or mucus, which can become infected. 7 Confusion can arise, and it may not be possible to differentiate an ectopic midline thyroid from a TGDC clinically. Up to 1% to 2% of patients, presenting with what appears to be a thyroglossal duct cyst, have an ectopic thyroid gland. 3 This is the case of the patient being reported, who was clinically diagnosed as having TGDC but was a case of ectopic thyroid. Of note, TGDC and ectopic thyroid can coexist. The wall of a thyroglossal duct cyst is the second most common site for ectopic thyroid tissue, the most common site being a lingual thyroid. 8
Ectopic thyroid is mostly asymptomatic, but like the normal thyroid tissue, it can become goitrous, can be hyper- or hypo- functioning, and can also undergo benign and neoplastic changes. These conditions cause enlargement of the gland, resulting in obstructive symptoms. Ectopic thyroid is commonly detected during periods of increased demand for thyroid hormones such as puberty and pregnancy. 2 Our patient also noticed the midline mass only in recent years and never gave a history of having such a mass before.
Imaging, specifically sonography and nuclear thyroid scans, is a must before planning any surgery for a midline neck mass. Sonography can identify and localize the midline mass, and it can determine the solid versus cystic nature of the mass. It also shows the presence or absence of the thyroid in its normal location. CT, if done, shows the mass in relation to other neck structures in all three dimensions. A thyroid scan using 99mTc is the most important diagnostic tool to detect ectopic thyroid tissue and should confirm the sonographic findings. It may also highlight additional sites of thyroid tissue. It has been shown to be greater than 95% sensitive and specific for differentiating ectopic thyroid tissue from other midline neck masses.9,10
Conclusion
Ectopic thyroid tissue poses difficult diagnostic and management challenges. This case report demonstrates the essential role of sonography and the nuclear thyroid scan in the evaluation of a midline neck mass to prevent unnecessary or inadvertent removal of the only functioning thyroid tissue and subsequent complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.