
Abstract
A vital component of clinical sonography is the approach the sonographer uses to analyze both the patient’s clinical history and the sonographic findings of each examination. Although every study is different, the sonographer is obligated to obtain the optimal information from both clinical history assessment and sonographic imaging in order for the interpreting physician to make an accurate diagnosis. One of the essential roles of sonography education is to provide instruction that allows students to gradually develop into clinically aware and proficient sonographers who are consistently capable of exploiting critical thinking and reasoning skills. Teaching both critical thinking and reasoning skills is a challenge for sonography educators, as both of these abilities tend to steadily improve with clinical experience. For the student, frustration can manifest as a result of this inexperience. Consequently, a standard framework for analysis would allow the sonography student a fundamental approach to use for every sonographic examination, thereby gradually, but possibly more rapidly, improving both reasoning and critical thinking skills in the clinical and classroom setting. The Sonographic Reasoning Method is a process created to provide this essential framework, combining critical thinking with reasoning skills, establishing structured thought, and promoting both competent and accurate patient care.
Keywords
Well-developed critical thinking skills are key for health care workers to provide quality patient care. Reasoning skills allow an individual to gather necessary information, recognize choice options, and make the best decisions possible in a given situation. In this article, we provide a brief analysis of critical thinking and varying reasoning methods and attempt to construct from this information a reasoning method that can be used in both the classroom and the clinical setting for sonography students.
Critical thinking is the process of evaluating one’s own thought process in order to improve one’s own decision-making abilities. Critical thinking is in essence thinking about thinking, and those who are great critical thinkers constantly tend to evaluate their own thought processes and search for ways to improve them. 1 Thinking allows conclusions to be drawn, which in turn leads to decisions. Our lives are determined by the outcomes or consequences of the decisions we make. For the sonographer, his or her thought processes during an examination can significantly affect the lives of others. For example, if a sonographer encounters hydronephrosis of the right kidney while performing a right upper quadrant sonographic examination, his or her critical thinking skills may lead to a further analysis of the ureter, urinary bladder, pelvis, and left kidney for evidence of associated obstructive uropathy. The sonographer’s obligation is to identify abnormalities and to image those abnormalities. But critical thinking involves analytic judgment and asking the “why” questions, until all the “why” questions have been answered to the best of the sonographer’s ability.
Analyzing the unique role of the sonographer offers some insight into how vital critical thinking is to the occupation. Although the sonographer has many daily tasks to perform, and some are physically demanding, reliance is placed on the sonographer’s intellectual aptitude as well. That is to say, the practice of diagnostic medical sonography is generally a cerebral occupation. Critical thinking in clinical sonography is ultimately used in the continual search for solutions and the rational search for, and recognition of, connections between pieces of objective case specific data. For this reason, interpreting physicians depend on the skills of sonographers and thereby develop close collaborative relationships with many of them. Health care educators face the challenge of developing teaching methods that encourage students to sharpen their critical thinking skills as they develop clinical scanning skills so that they can provide high-quality care.2,3 Several methods have been used to promote critical thinking in a classroom setting, although measuring the success of each method is difficult.
The Antidote Method
One such method, described by Mottola and Murphy, 4 is called the Antidote Method. This is an interactive group activity in which an instructor provides participants with a scenario or dilemma relating to their field of study. The participants are then asked to write a list of all factors that were thought of in order to come to a solution. The factors are compiled on a board for the entire group to examine. The instructor then leads a group discussion based on all of the ideas that were gathered. Afterward, participants try to come up with ideas that had not been thought of prior to the discussion. The Antidote Method is thought to encourage “practice thinking” for students, ultimately allowing them to evaluate their individual process of thinking.
Concept Maps
Concept maps have also been shown to be an effective teaching tool for promoting critical thinking. 5 In this method, students are asked to draw a box at the top of a piece of paper and then write inside it a scenario that describes a patient’s condition or complaint (e.g., right lower quadrant pain). Students are then asked to draw lines that lead to other boxes, in which related concepts are placed (e.g., abdominal surgery, appendicitis, sharp vs. dull pain). With each connecting box placed further down the page, the content becomes more detailed. As the students gain more clinical experience, the size of and details within the concept map typically increase.
Role-Playing Scenarios
A third method of teaching critical thinking was developed by Eerden. 6 It involves placing students in a role-playing situation in which they are given a case study with all pertinent patient information, including a clinical history, reason for procedure, and signs and symptoms. The educator plays the role of the patient and is asked questions by the students. This role-playing method helps students learn how to interact with patients effectively in a controlled setting. Concurrently, the method assists in the development of appropriate patient communication skills, while improving the skill of extracting clinically relevant information through practice patient interviews. Using computer-assisted instruction in conjunction with these methods is thought to be useful in encouraging critical thinking. Case studies are typically used while students practice the progression of asking appropriate questions, prioritizing the information that is gathered, making a plan of how to care for the patient, and then evaluating the results.
Reasoning Strategies
Intuition
Several reasoning strategies are commonly used to reach a conclusion. Perhaps most useful is an intuitive strategy, which is based on personal experience. 7 As a concept, intuition is subjective and is based on an individual’s experiences and perceptions of reality. When confronted with a problem, the use of intuition allows a person to recognize how the problem is the same as, or similar to, a problem that has already been solved. It is a subconscious decision-making tool and is therefore nearly impossible to teach.7,8
The use of intuition involves a complex mental process that includes pattern recognition and the ability to rapidly retrieve a suitable answer on the basis of personal experience.7,9 This concept is evident in everyday life and can be easily examined by simply comparing the amount of life experiences a 6-year-old has with those of a 35-year-old. One can assume that merely on the basis of accumulated life knowledge, a 35-year-old would make superior, more well-informed decisions compared with a 6-year-old. Nevertheless, even though one accrues knowledge through decision making and observation, one still has the choice of whether to use that knowledge or to ignore prior decision-making consequences in the hopes of reaching a different conclusion.
The vital role of intuition in reasoning is readily apparent in one’s occupation. For example, experienced health care professionals tend to have better understanding of clinical symptoms because they have a greater range of past experiences from which to reference when analyzing the connections between symptoms. 8 The disadvantage of this strategy is that it is obviously not available to those who are novices in their fields. 9 Nonetheless, it is evident that the more clinical experience and practice one gains, the more intuition can be used.
Inductive and Deductive Reasoning
There are other reasoning strategies that can be used when one lacks the initial experience to use intuition to solve problems. These strategies include inductive and deductive methods of reasoning. 8 Inductive reasoning is a bottom-up strategy in which one is given facts and then seeks a general pattern that relates those facts. With inductive reasoning, one makes observations or premises and then draws conclusions on the basis of those observations. In inductive reasoning, the conclusions are based on the evidence but are not proven. For example:
Premise 1: Many people who smoke develop lung cancer.
Premise 2: Person A smokes.
Conclusion: Person A will develop lung cancer.
Although the conclusion is possible and perhaps even probable, it is not guaranteed. That is to say, just because a person smokes does not mean he or she will develop lung cancer. This type of reasoning is commonly used in a health care setting when a patient provides symptoms, laboratory values, and other clinical history elements. One would use this information to try to determine the cause of the symptoms. The diagnosis would be probable but not proven. The following example provides a sonographic application of inductive reasoning:
Premise 1: Patient A reports right upper quadrant pain in the gallbladder region.
Premise 2: A common cause of gallbladder pain is gallstones.
Conclusion: Patient A has gallstones.
Deductive reasoning is a top-down approach to logic. This form of reasoning draws specific conclusions from general statements or premises. The conclusions that are derived from deductive reasoning are certain, provided that the initial premises are true. For example:
Premise 1: All men are mortal.
Premise 2: Person A is a man.
Conclusion: Person A is mortal.
Although these strategies are discussed as separate methods, they are often used simultaneously to solve a single problem. Inductive reasoning and intuition are used to come up with hypotheses based on the information at hand. Subsequently, deductive reasoning is then used to test the hypotheses that were found and ultimately draw a conclusion. This is the basis of the scientific method, which is a standard framework that is used in many decision-making scenarios. The scientific method consists of the following steps: observation, hypothesis, data collection, data analysis, and conclusion.8.9
The Sonographic Reasoning Method: Steps in the Process
Although other research has attempted to associate the steps of the scientific method with medical sonography, the act of instructing students in the use of such an intricate method can be difficult. 9 Simplification of the method into a more clinically applicable and, importantly, memorable process of thinking for students is fundamental for proper instruction. The Sonographic Reasoning Method (SRM) is a simple five-step process that can provide an essential framework for reasoning in sonographic practice, combining critical thinking with reasoning skills, thus establishing structured thought and ensuring both competent and accurate patient care (Figure 1). The ultimate goal of the SRM is to assist educators in cultivating more clinically mindful students. Provided below are the steps of the SRM and a means whereby a student can practice the process in the clinical and classroom settings.
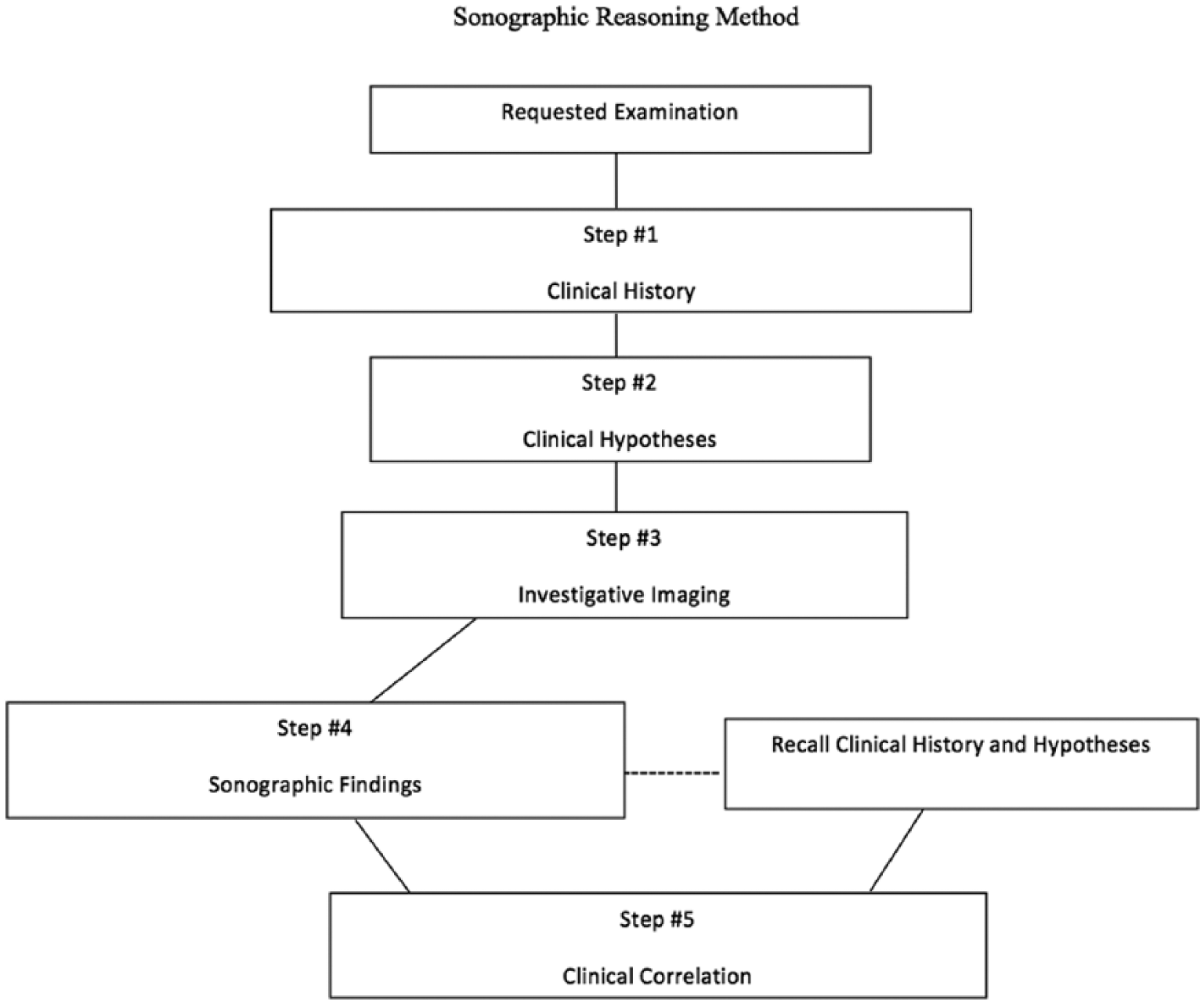
The Sonographic Reasoning Method. Step 1: clinical history—the information gathered by obtaining a clinical history; step 2: clinical hypotheses—educated guesses based on clinical history findings; step 3: investigative imaging—a technique used by sonographers whereby they obtain sonographic protocol images while searching for and identifying abnormalities; step 4: sonographic findings—information gathered by performing the sonographic examination; step 5: clinical correlation—the process of recalling clinical history and clinical hypothesis, contrasting that information with sonographic findings, and evaluating the information for connections.
Step 1: Clinical History
The first step is to gather a thorough clinical history. For the sake of generalization, a clinical history is defined here as the patient’s age, race, signs and symptoms, laboratory findings, results of other previous diagnostic testing, pertinent illnesses, and past surgical procedures. That is, both medical history and clinical findings are combined in the term clinical history for case-specific information-gathering purposes. Many times, both laboratory findings and diagnostic testing results can be accessed electronically before the student meets the patient. This process allows the student to establish a pertinent line of questioning specific to the study at hand.
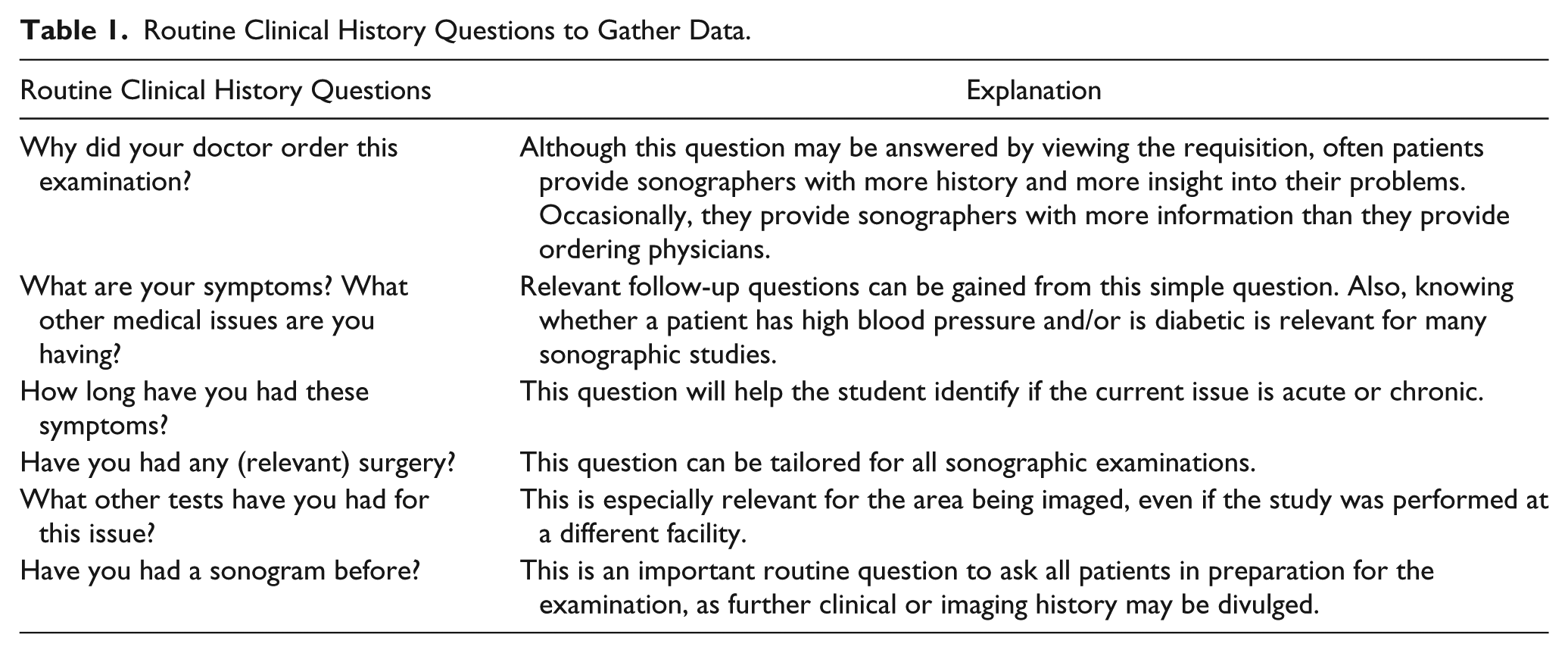
Gathering clinical history also requires that the student interact and communicate effectively with the patient. This would necessitate that both fundamental questions and case-specific questions be asked of the patient. Table 1 provides some routine clinical history questions that can be asked of almost every patient. Numerous relevant and detailed questions can be asked in sonographic examinations, as in obstetrics, vascular assessment, and echocardiography. Students must gather all available clinical history before proceeding to step 2.
Routine Clinical History Questions to Gather Data.
Step 2: Clinical Hypotheses
On the basis of clinical history, the student can now establish several working clinical hypotheses. A clinical hypothesis is simply an educated guess based on the clinical history gathered. Baum, 9 who initially recommended the application of the scientific method to sonography, referred to this step as developing a working diagnosis. Like step 1, this process can present a challenge for the novice, though with increased and repetitive use of the method, one can improve one’s ability to make an educated guess. By using textbooks and with the assistance of instructors or experienced sonographers, students can learn more about the importance of clinical history in the development of a clinical hypothesis. Classroom instruction can be guided toward correlating clinical history with sonographic findings. To enhance the ability of the student to obtain a thorough clinical history, instructors can perform some of the critical thinking teaching techniques mentioned above. Figure 2 provides an example of how the SRM could be accomplished during a first-trimester obstetric examination.
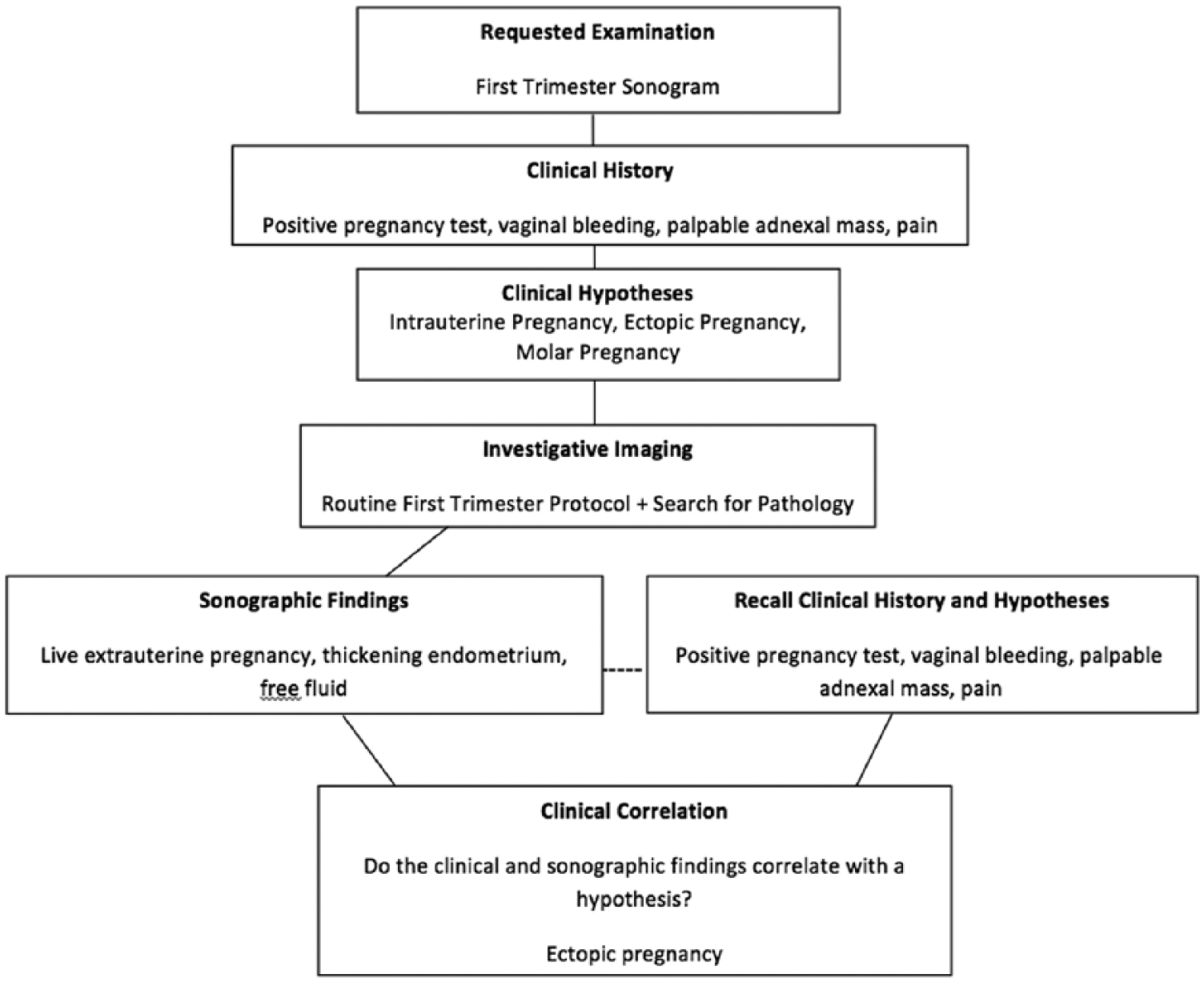
An example of the Sonographic Reasoning Method as applied to a first-trimester sonographic examination.
Step 3: Investigative Imaging
With the clinical hypotheses and history in mind, the sonographer can perform an examination with greater accuracy compared with a limited clinical history. Investigative imaging is a unique role for the sonographer. It is a technique used by sonographers whereby they obtain sonographic protocol images while searching for and identifying abnormalities. Although multiple routine sonographic images are acquired with the use of a standard protocol, the role of the sonographer is also to evaluate, identify, and demonstrate any abnormalities noted during the examination.
From the information gathered during step 1 and the hypotheses developed in step 2, the sonographer has the ability to modify the examination to match the gathered clinical history information. A thorough clinical history may clarify the need for an examination and thereby focus the examination on a more specific concern. For example, a patient may present to the sonography department for an abdominal sonographic study with an unclear indication of abdominal pain. By collecting a thorough clinical history, the sonographer discovers that the patient had a cholecystectomy for gallstones 1 week earlier and is currently reporting severe right upper quadrant pain, nausea, and vomiting. Although the sonographer will certainly perform a thorough examination, including providing all standard-protocol images of the entire abdomen, the sonographer may concentrate more on the liver, biliary tree, and pancreas, as a possible retained gallstone may be present in the biliary tree. With time, and the use of the SRM, students will become more aware of variations required to standard protocols when pathology is suspected before and/or discovered during an examination.
Step 4: Sonographic Findings
Sonographic findings include all imaging findings that are noted during the sonographic examination. The student can collect all sonographic findings from the sonographer or from the sonographer’s report. As the student becomes more familiar with the process, the primary focus should be placed on relevant abnormal findings. Relevant abnormal findings can be defined as those imaging findings related to the patient’s report of symptoms at the time of the examination. For example, if a patient currently reports epigastric pain and back pain and has elevated pancreatic laboratory results, the relevant findings would be associated with pancreatic and biliary tree abnormalities. Although an incidental simple renal cyst may be noted during the examination, only relevant findings should be collected to complete step 4.
Step 5: Clinical Correlation
Clinical correlation is the process of recalling the obtained clinical history in step 1 and the clinical hypotheses established in step 2, combining that information with the sonographic findings from steps 3 and 4, and evaluating the information for connections. In this step, instruction can really commence. The gradual accumulation of knowledge is ongoing in sonography. However, once one has recognized the definite links between clinical history and sonographic findings, a solid base of knowledge is established. Educators must be aware, however, that clinical correlation ambiguity is common. Clinical correlation ambiguity is the uncertainty about common links between clinical history and sonographic findings. It is a hurdle for inexperienced students to overcome but one that can be conquered with practice. This step will likely enhance the student’s ability to recognize the need for the correlation of clinical history and imaging findings in clinical practice and also promote reasoning and test taking skills in the classroom.
Clinical and Classroom Applications of the Sonographic Reasoning Method
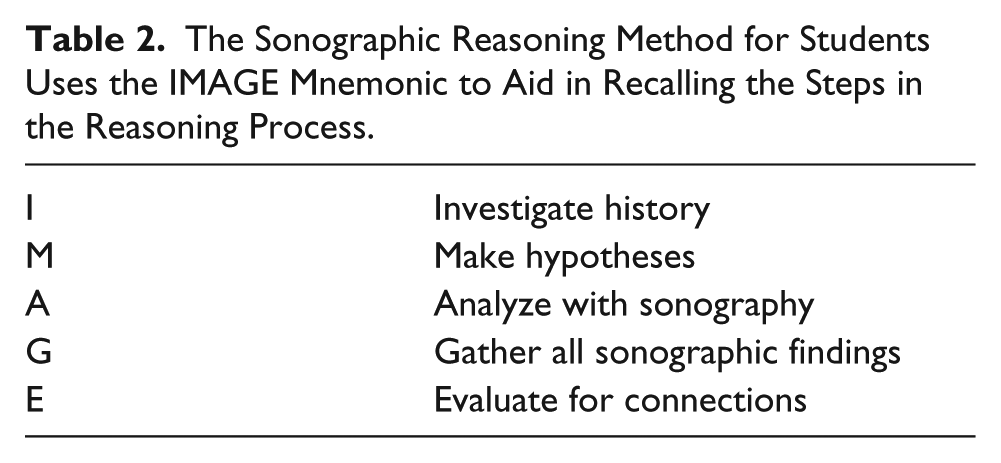
As discussed, the SRM can be exploited in the clinical setting. For students, often a simple mnemonic helps provide a memory tool that can be used for quick recall. The word image can be used as a mnemonic to facilitate recall of the five successive steps of the SRM: investigate history, make hypotheses, analyze with sonography, gather all sonographic findings, and evaluate for connections (Table 2). Students can be encouraged to use the IMAGE mnemonic in the clinical setting before, during, and after a sonographic examination. They could be required to document a specified number of cases using IMAGE and furthermore be required to discuss these with sonographers, other students, and/or their instructors.
The Sonographic Reasoning Method for Students Uses the IMAGE Mnemonic to Aid in Recalling the Steps in the Reasoning Process.
Using the provided form based on the IMAGE mnemonic in Figure 3, students can easily follow the steps of the SRM. Additionally, as noted on the SRM form for students, a final question—“What did you learn?”—provides a commentary section for students to offer their personal reflections. Once clinical use has commenced, students can share interesting cases with other students online using IMAGE, so that collaborative learning can take place. During clinical rotations, it may be wise to have students document these noted connections in a clinical log or online through an educational portal. In the classroom setting, instructors may ask students to provide case study presentations based on the SRM using IMAGE. As a cautionary note, instructors need to strongly emphasize that to maintain privacy standards, all personal patient identifiers must be removed, so that the pathology becomes the main topic. Additionally, in the practice of sharing any information in the classroom or online, all Health Insurance Portability and Accountability Act of 1996 guidelines must be followed to ensure that patient confidentiality is protected.
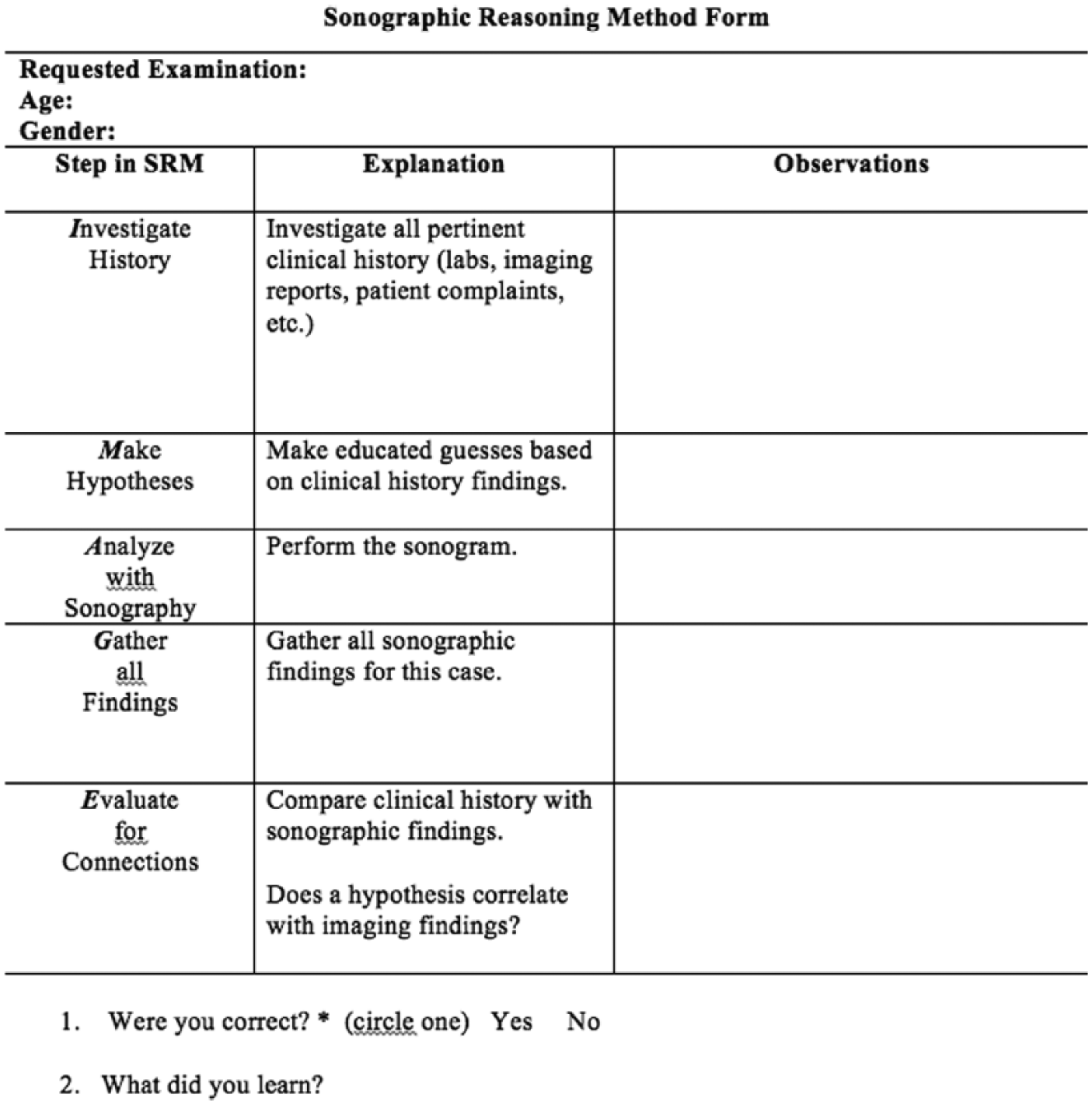
The Sonographic Reasoning Method (SRM) form for students using the mnemonic IMAGE for clinical and classroom application.
Limitations
As most experienced sonographers and educators know, one’s hypotheses concerning the clinical findings of a sonographic examination can intermittently be flawed. This is not because the sonographer is inept but rather because unique cases arise occasionally that are beyond the established knowledge base of even the most experienced practitioners. A hypothesis is simply an educated guess, and although one can make an accurate guess occasionally, the process does not always work. There can be a long list of differential diagnoses in many cases. For beginning students, the SRM may be overwhelming in clinical practice because they are not experienced at collecting, much less correlating, clinical and sonographic findings. This limitation can be overcome with more experience and instruction of how to use the IMAGE mnemonic in both the classroom and clinical settings. Students may be asked to demonstrate the function of IMAGE during case studies to other students. Printing out the IMAGE outlines (Figure 3) for students to complete themselves throughout the clinical day can assist them in the collection of data as well.
An additional limitation involves struggles with a patient who is a poor historian, ultimately leading to an imperfect clinical history. Unfortunately, this would result in an IMAGE form that is exceedingly limited. Students should be instructed not to be discouraged but rather accept the reality that limited clinical history is a challenge. As a result, their awareness should be even more discriminating during the sonographic examination, as the examination results will strongly be dependent on the sonographic findings.
Conclusions
Developing ways to teach critical thinking lies partly in the creativity and awareness of the educator and partly in the student’s foundation of knowledge. Therefore, methods of instruction must be malleable, for what works well for one class might not work for another. Even among classmates, there can be a wide range of suitable learning styles. With time, the process of reasoning in the clinical setting becomes innate for most sonographers, but initially it is a challenge for every student. The SRM offers a standardized structure for students to follow in every sonographic examination and thereby provides a means to assist educators in cultivating more clinically mindful students and, ultimately, more skilled and clinically aware sonographers.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.