
Abstract
Bladder tumors are extremely rare in young adults and are usually linked to tobacco abuse, chronic infections, or occupational exposure to carcinogens. We present a case of a papillary urothelial neoplasm in a 19-year-old man with no significant risk factors, initially detected by sonography and later confirmed with computed tomographic urography and cystoscopy. The tumor was quickly resected and mitomycin C instilled in the bladder prophylactically. This is an atypical situation in a patient with none of the common risk factors.
Papillary urothelial neoplasms of low malignant potential (PUNLMPs) are premalignant bladder tumors that typically present in the sixth decade of life with gross or microscopic hematuria and a prevalence toward males.1-3 These noninvasive tumors were first classified as PUNLMPs by the World Health Organization in 1997, in an attempt to avoid using the word carcinoma for a premalignant tumor with such low potential for progression. 4 Histologically, PUNLMPs show increased cellular proliferation and thickened urothelium; however, the excess proliferation is not invasive and is limited to the basal layer.1,3,5 PUNLMPs are an important entity, as they do have a tendency to recur and, although low risk, can become malignant; therefore, tumor resection and close follow-up are recommended. 1 In this case report, we describe a rare occurrence of a PUNLMP with emphasis on quick diagnosis and treatment due to the patient’s young age.
Case Report
A 19-year-old male college student presented to the student health clinic with a 1-week history of recurrent hematuria and passing blood clots. He denied any other systemic symptoms or increased urinary urgency. Physical examination was unremarkable. He had no personal history of nephrolithiasis. Social history did not reveal any tobacco history or occupational exposures. He reported that his grandfather has prostate cancer; otherwise, there was no family history of malignancy.
Ultrasonography of the kidneys and bladder was done with a Philips iU-22 system (Philips Ultrasound, Bothell, WA) with a C5-2 curvilinear abdominal probe. The examination showed a polypoid mass (1.3 × 0.7 cm) in the area of the left ureterovesical junction that was fixed to the bladder wall, as demonstrated in the right lateral decubitus position (Figure 1). On color Doppler imaging, the lesion was seen to have significant vascularity (Figure 2). There was no associated hydronephrosis, and the kidneys were otherwise normal. The concern for a possible bladder malignancy versus ureteral polyp was raised, and the patient underwent a contrast-enhanced computed tomographic scan of the abdomen and pelvis, which showed a small filling defect at the left ureterovesical junction on delayed imaging (Figure 3). Cystoscopy showed a 1-cm bladder tumor (Figure 4). The tumor was resected and sent for pathologic analysis, followed by perioperative prophylactic installation of mitomycin C. Histopathologic analysis showed a PUNLMP. The patient is to be followed up by the Department of Urology in 3 months.
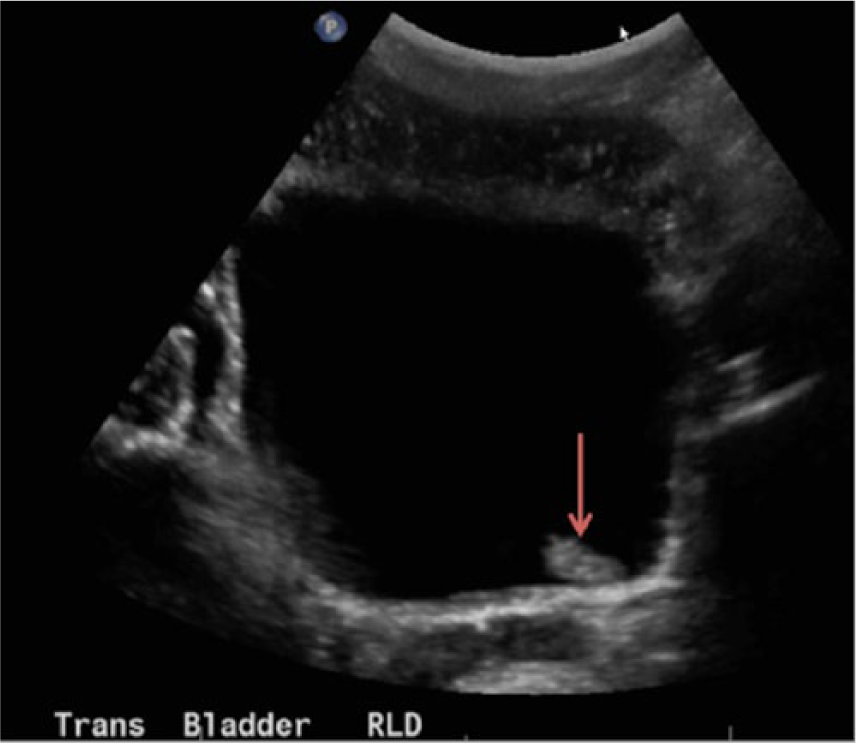
Transverse view of the urinary bladder in the right lateral decubitus position shows an adherent mass (1.3 × 0.7 cm) near the left ureterovesical junction (arrow).
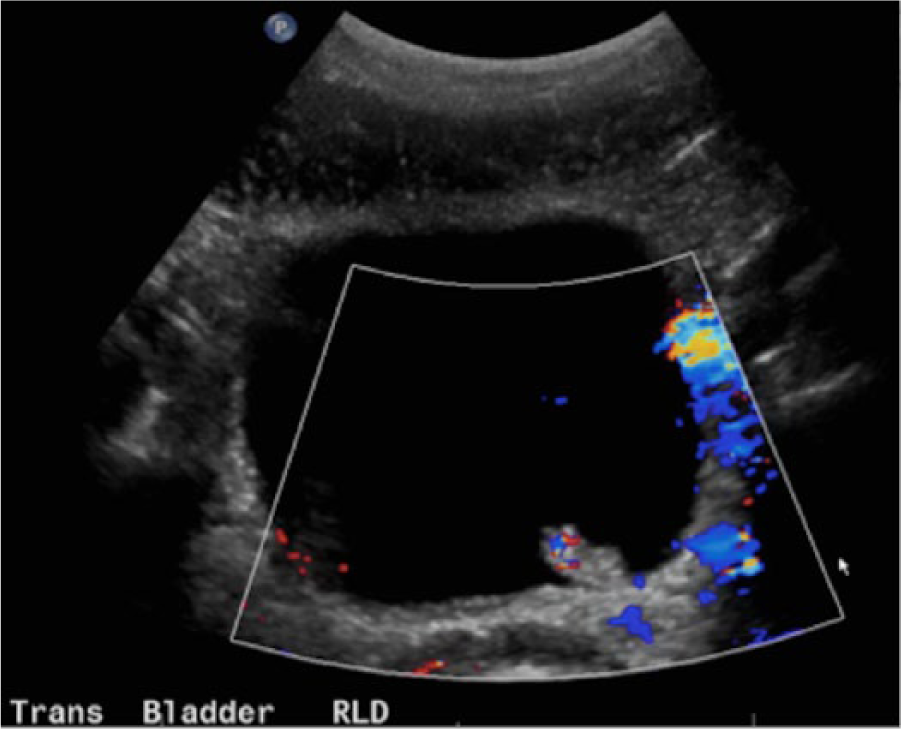
Color Doppler image of the same mass shows significant internal vascularity.
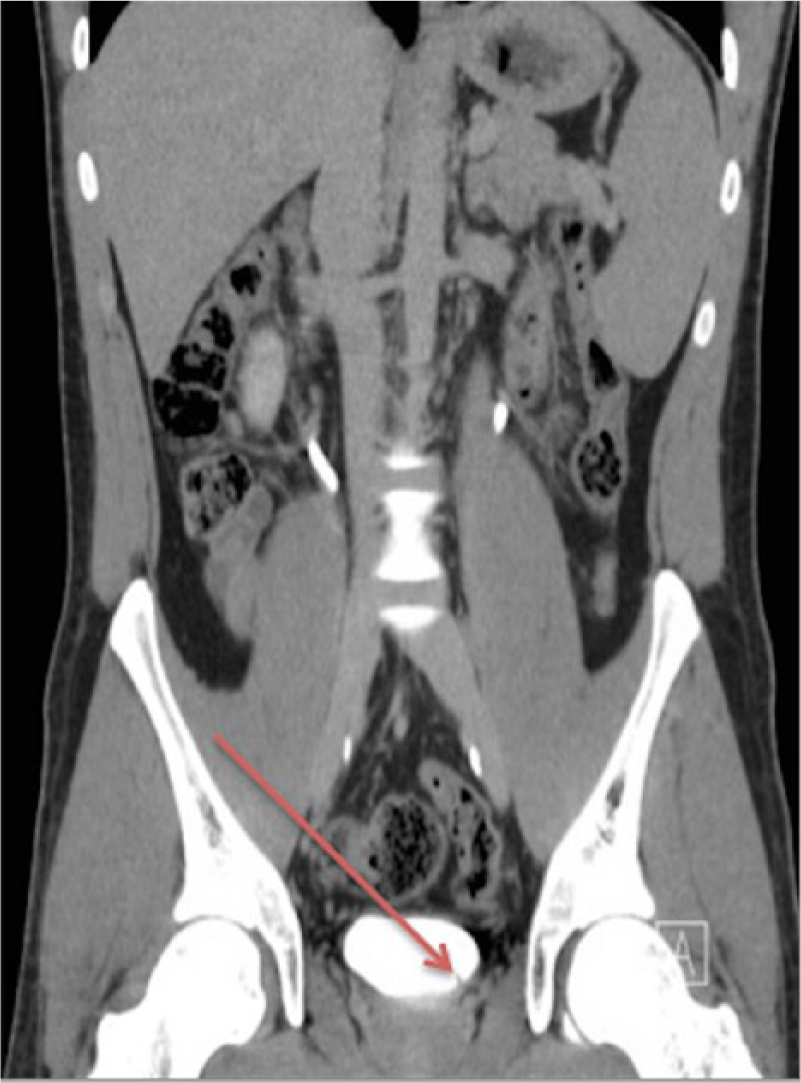
Coronal delayed imaging by computed tomography shows a tiny filling defect (arrow) consistent with a bladder mass. Early enhancement was not seen on the initial contrast computed tomography, as the bladder was empty.
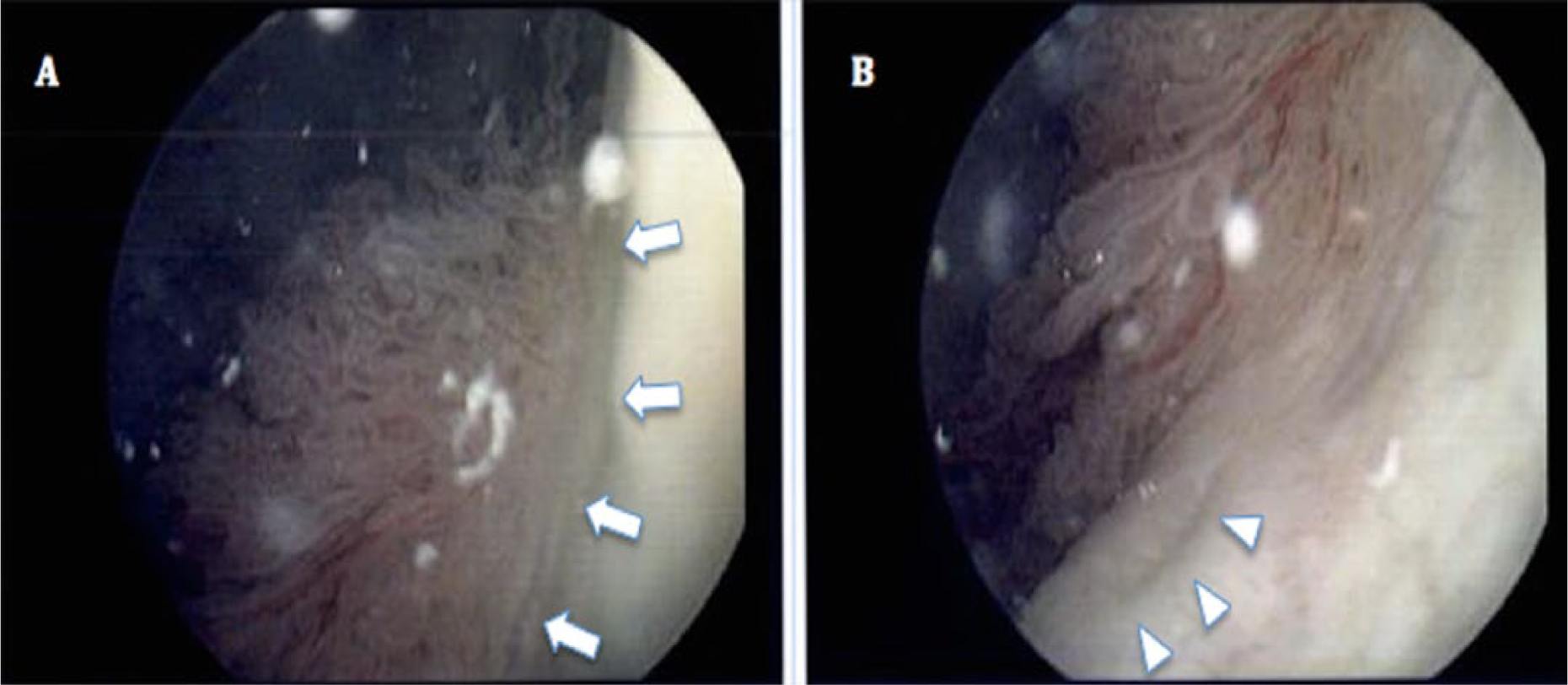
Cystoscopy images showing the 1-cm papillary tumor (A; arrows) and that it was approximately 1 cm above the left ureteral orifice (B; arrowheads).
Discussion
Bladder cancer is the fourth-most common malignancy in the United States and is predominantly seen in adults 60 years of age and older. 2 Risk factors include smoking, exposure to aniline dyes, certain chemotherapeutic agents, chronic bladder infections, and family history. It is rare to find both premalignant and malignant bladder tumors in pediatric patients and the young adult population. Paner et al. presented a series of patients younger than 30 years with bladder tumors and showed that only 3.0% had invasive carcinoma and 1.7% had high-grade tumor. 6 In a similar series of 59 young patients, Stanton et al. found ten invasive urothelial tumors (17%) and 8% of patients with high-grade noninvasive carcinomas. 7 Another small series showed very favorable outcomes for young patients with bladder tumors, observing a recurrence rate of 13% treated with repeat resection. 8
Grayscale ultrasonography is frequently used to evaluate patients with hematuria, especially in young patients. Primary bladder neoplasms are rare in young adults, and the differential diagnosis for a sonographically detected bladder mass should include other entities, such as edema from cystitis, blood clots, prostatitis causing prostate enlargement, or normal bladder trabeculae. 9 Previous studies have verified that sonography may be used as an effective tool for the detection and staging of bladder tumors.9,10 The presence of a full bladder, as seen in this case, allows for excellent contrast, aiding in the detection of small papillary lesions. Reevaluating the patient in the decubitus or prone position, along with the use of color Doppler imaging, helps to differentiate such tumors from blood clots. Computed tomography helps to detect other associated tumors in the upper urinary tract and may also help confirm lesions within the urinary bladder.
Conclusion
Tumors of the bladder, benign and malignant, are rare in young people and tend to be low grade and noninvasive with favorable outcomes. Typically, as age increases, so does the tumor grade, with progression to malignancy. The first-line treatment remains surgical resection.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.