
Abstract
The objective was to evaluate the utility of the “pocket ultrasound” in making clinical decisions in urologic emergencies. From May to September 2011, 105 patients were assessed for urologic emergencies: acute flank pain, macroscopic hematuria, urinary retention, and lower urinary tract symptoms. All patients underwent an ultrasonographic examination whereby the pocket ultrasound was used to evaluate the kidneys and bladder, followed by another appropriate diagnostic test to verify the suggested diagnosis. Urinary retention was diagnosed in 10 patients. Of 48 subjects with hematuria, 34 had an immediate diagnosis: there were 18 cases of a bladder tumor, 13 cases of urolithiasis, and 2 cases of renal cell carcinoma; one ureteral stent was detected. Of 30 patients referred with lower urinary tract symptoms, 14 showed a high post micturition residual and 2 were seen to have bladder diverticula. Of 17 patients with acute flank pain, 1 had a kidney abscess, 5 had hydronephrosis, and 11 had urolithiasis. Ultrasonography provided a conclusive diagnosis in 67.6% of cases. Point-of-care pocket ultrasound allows a rapid diagnosis for treatment or triage of patients for appropriate referral to other diagnostic methods.
Ultrasonography (US) plays an important role in the evaluation of medical or surgical diseases, allowing the clinician to avoid ionizing radiation and contrast material injection. In urology, US is a rapid, cost-effective, and time-saving modality for obtaining diagnosis, undertaking appropriate management, and conducting further assessment of patients.1–7 From the first clinical applications in the 1940s, a great number of advances have been made in US technology, with a consequent improvement in the diagnosis of urologic disorders.8–11 This technology is now available as a pocket-size visualization tool (V-Scan, GE Vingmed Ultrasound A/S, Horten, Norway) that provides clinicians with a noninvasive method to secure immediate diagnostic information at the bedside, giving black and white anatomic as well as color-coded blood flow images in real-time. The instrument is approximately the same size as a smartphone and can easily be taken from room to room to be used in a variety of clinical, hospital, and primary care settings. The purpose of the current study was to evaluate the utility of the “pocket ultrasound” in making clinical decisions in urologic emergencies.
Methods
This was a prospective clinical study carried out in the Policlinic of San Donato Milanese between May and September 2011. As the pocket ultrasound is noninvasive and is routinely used in our clinical practice, the hospital ethics committee (institutional review board) approved the study and waived the requirement for informed consent. Consecutive patients presenting with a urologic emergency were enrolled. All patients had a complete history taken and physical examination followed by an US evaluation using the pocket ultrasound, equipped with a linear phased array probe with a frequency range of 1.7 to 2.8 MHz. The US evaluation was followed by another appropriate diagnostic test (e.g., abdominal computed tomography [CT], cystoscopy, or transrectal or abdomen US) to verify the diagnosis suggested by US. All US examinations were performed by an experienced urologist with formal sonographic training and followed the Guidelines of the Italian Society of Ultrasonology in Medicine and Biology. 12 For the purposes of data collection, all symptoms recorded were defined according to Campbell’s Urology. 13
Kidney stones were visualized in the ultrasonographic image as a bright object casting a posterior shadow. Bladder tumors were defined by an echogenic structure of the bladder wall without acoustic shadowing suggestive of a mucosal irregularity, characterized by heterogeneous, irregularly shaped masses within the bladder. Renal masses were noted as hyperechoic, hypoechoic, or anechoic and could appear anywhere within the kidney; all suspected renal masses were verified by a CT assessment with contrast enhancement to distinguish benign structures from renal cell carcinomas. Hydronephrosis, secondary to any cause of obstruction to flow, appeared as an anechoic area beginning at the renal pelvis distending the normal bright white (hyperechoic) central area of the kidney, with calyces enlargement. With progressive obstruction, the renal parenchyma becomes compressed, showing thinning pyramids. CT evaluation was done in all patients with suspected obstruction to determine the true cause of urinary obstruction. Both longitudinal (long axis) and transverse (short axis) views were obtained to evaluate the bladder volume and to calculate the post micturition residual.
Results
During the study, 105 consecutive patients (80 men [76.2%] and 25 women [23.8%]) with a mean age of 62 years (range, 31-89 years), who were either hospitalized or in the emergency department, were evaluated for an urologic emergency. The patients presented with acute flank pain (17 patients), macroscopic hematuria (48 patients), urinary retention (UR, 10 patients), and lower urinary tract symptoms (LUTS, 30 patients). (Table 1) The average time spent by the urologist on the US examination for each patient was approximately 10 minutes.
Urologic Disorders Evaluated
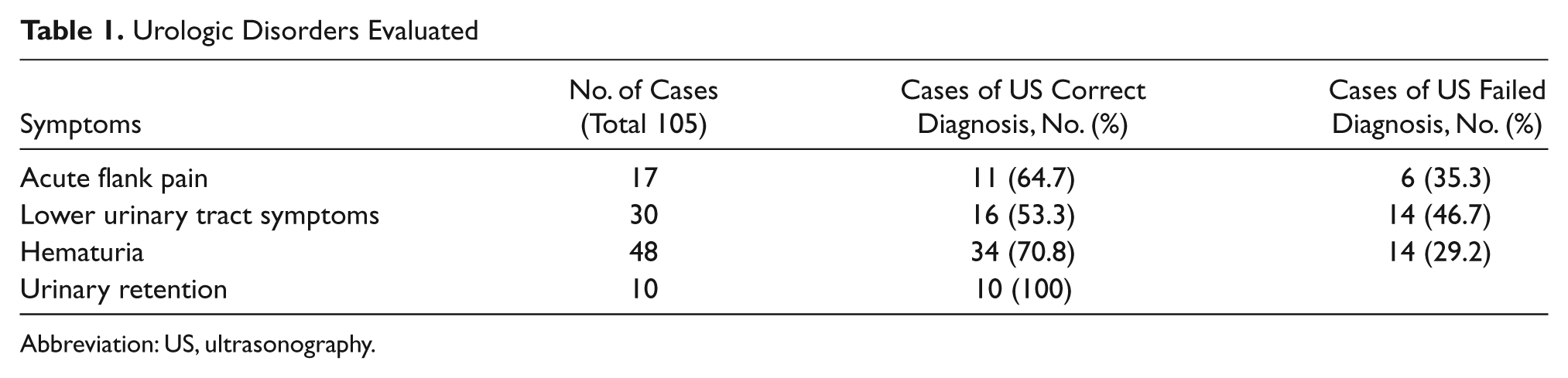
Abbreviation: US, ultrasonography.
The pocket ultrasound correctly diagnosed UR in all 10 patients, and these were directly managed through catheterization. Of 48 patients with hematuria, 34 had an immediate diagnosis. In 2 patients, sonography suggested a renal cell carcinoma (RCC), 13 patients were diagnosed with urolithiasis (confirmed by the following abdominal CT), 18 patients had a bladder cancer shown by US, and in 1 male a ureteral stent was visualized and confirmed by the subsequent cystoscopy. Patients noted to have urolithiasis were treated by extracorporeal shock wave lithotripsy (ESWL), by percutaneous nephrolitholapaxy (PNL), or by endoscopic removal on the basis of size and location of the stone according to the European Association of Urology guidelines. 14 Eighteen patients with US evidence of bladder tumor were sent for an immediate transurethral resection of the bladder (TURB), avoiding further delay in the histological diagnosis. Of the 14 patients in whom US failed to demonstrate a diagnosis, 8 were subsequently found to have ureteral stones, 2 had urothelial cell carcinoma of the upper urinary tract, and 4 had a small (<0.5 cm diameter) or flat bladder cancer.
Of 30 patients referred for LUTS, 14 showed a high post micturition residual due to benign prostatic enlargement, and 2 were affected by bladder diverticula, confirmed by suprapubic US and cystoscopy, respectively. The other 14 patients needed further evaluation such as cystoscopy, transrectal US, uroflowmetry, or multichannel urodynamics to reach a definitive diagnosis.
Of 17 patients presenting with acute flank pain, 11 were diagnosed with kidney stones. Eight of these were sent for ESWL without the need for further diagnostic tests; the other 3 underwent abdominal CT before the PNL or endoscopic removal. One patient had a hypoechoic area in the kidney seen with an associated fever, confirmed by subsequent abdominal CT to be a kidney abscess. In 5 patients with a high or medium grade of hydronephrosis, an immediate abdominal CT was requested for definitive diagnosis (Table 1).
The pocket ultrasound was used to make a conclusive diagnosis in 71 patients (67.6%), which was verified by further testing. In 34 patients (32.4%), 14 with hematuria, 14 with LUTS, and 6 with acute flank pain, an additional investigation was needed to reach a conclusive diagnosis. The pocket US made a correct diagnosis in 100% of cases of UR and in 70.8% of patients with macroscopic hematuria. In 64.7% of cases of acute flank pain, a definitive diagnosis was reached, whereas in patients with LUTS, only 53.3% had a definitive treatment decision made on the basis of US evaluation.
Discussion
Ultrasonographic examinations are routinely used in the urologic clinical practice for the emergent evaluation of several diseases and conditions, such as acute flank pain, urinary retention, macroscopic hematuria, and hydronephrosis. Patients presenting with acute flank pain are more frequently affected by renal or ureteral stones. If it is not possible to identify ureteric stones sonographically, dilatation of the pelvicalyceal system is also considered by many as evidence of an obstructed ureter and can be used qualitatively to assess its grade as mild, moderate, or severe. The pocket ultrasound allows the immediate evaluation of these patients in the emergency department, facilitating the decision to admit the patient for moderate or severe hydronephrosis with altered renal function or to treat as an outpatient with an abdominal CT or other appropriate medical therapy to facilitate stone passage. This avoids unnecessary hospitalizations and thus allows significant cost savings, not an insignificant outcome considering that between 120 and 140 per 1,000,000 people will develop urinary stones each year. 14 Moreover, a renal or ureteric stone visualized by US can be directly treated by ESWL, without the need for further investigation. 15
Because of its widespread availability, ease of use, and noninvasive nature, sonography is also the preferred initial examination in the clinical evaluation of macroscopic hematuria for the detection of bladder tumors. The success of sonographic examination does depend on size and location of the tumor; bladder cancers larger than 0.5 cm and/or localized in the bladder neck or in the dome areas are difficult to detect. Diagnostic accuracy may approach 95% for tumors larger than 0.5 cm situated on the posterior or lateral walls of the bladder.16–18 If a bladder tumor has been clearly visualized by US, the patient can undergo TURB directly and avoid any delay in diagnosis and risk of progression. Renal, ureteral, or bladder stones may also be responsible for hematuria, and as noted above these are easily evaluable by US, allowing an immediate differential diagnosis and rapid therapeutic decision making.
In patients with an absence of spontaneous micturition, a sonographic evaluation of the urinary bladder volume allows a rapid diagnosis of urinary retention, leading to an immediate catheterization and typically a discharge from the emergency department after a relatively short stay.
The study reported has shown that the availability of the small, lightweight US unit in clinical practice has been both time-saving and cost-effective. A conclusive diagnosis was reached in 67.6% of patients evaluated, with all cases of UR correctly diagnosed and followed by immediate treatment and discharge. A conclusive diagnosis was reached in 70.8% of cases with macroscopic hematuria; 18 patients noted to have bladder cancer were selected for an immediate TURB, and 13 with a diagnosis of urolithiasis were triaged directly to ESWL. Two patients with suspected renal cell carcinoma went on to an abdominal CT to achieve a conclusive diagnosis. US failed to demonstrate a conclusive diagnosis in 8 patients with ureteric stones, 2 with urothelial cell carcinoma of the upper urinary tract, and 4 with a small or flat bladder cancers. In cases of macroscopic hematuria, the US evidence of bladder cancer should not necessarily be accepted as conclusive, as many clinicians would advocate a follow-up cystoscopy and/or CT scan to evaluate the lower urinary tract and to rule out upper urinary tract diseases, respectively. However, the pocket US evaluation still remains of value as an initial test that may triage patients with suspected bladder tumors into high-risk and fast-track groups.
Patients with an acute flank pain were correctly diagnosed in 64.7% of cases, whereas in the remaining 35.3% an abdominal CT was necessary to reach a diagnosis. Several cases of urolithiasis needed a CT scan for a definitive diagnosis and management, although a quick assessment of hydronephrosis rapidly differentiated urinary obstruction from nonurinary cause of pain. When US identified stones smaller than 2 cm, an immediate ESWL could be planned. In the group of patients referred for LUTS, only 53.3% had a definitive treatment decision made on the basis of the pocket US evaluation, whereas 46.7% needed further imaging studies for diagnosis and management.
In all of the reported cases, the small ultrasonographic unit allowed a more rapid diagnosis, resulting in an immediate treatment plan, or readily demonstrated the need for further imaging studies to reach a definitive diagnosis. 19 The 10 minutes required for the US scan significantly reduced patients’ wait time, providing faster and more efficient patient care, with a considerable cost savings and, in many cases, the avoidance of an unnecessary hospitalization. It is difficult to estimate the exact financial effect, although several factors would indicate cost savings: the short examination time can be weighed against the €15 that it costs per hour in hospital staffing for direct patient care, the pocket ultrasound unit costs considerably less than a conventional US machine, and the portability of the pocket unit allows ultrasound examination with the need for formal referrals in many cases. The data suggest that the pocket ultrasound should be included in the armamentarium of urologists, based on their familiarity with evaluation of the urinary tract, and should be considered an extension of the physical examination that can be used to simplify and speed the diagnostic algorithm without the need for a formal, written report. It is of utmost importance that urologists obtain proper training in the techniques required for image optimization and in the recognition of artifacts before using such devices in their routine clinical practice. This also will alleviate one of the main concerns of many urologists regarding the medico-legal consequences of missing a diagnosis. 20 In our own urologic center, we have established a training program in US designed to provide all urologists with a satisfactory level of competence.
Conclusion
Bedside ultrasonography is a rapid, safe, and noninvasive imaging examination for the evaluation of urologic emergencies and in routine urologic clinical practice. Our results suggest that the availability of a portable pocket ultrasound system allows a more rapid diagnosis and management of several urologic conditions. Moreover, the pocket ultrasound is likely also of value in its ability to rapidly triage patients for other appropriate diagnostic testing such as CT.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.