
Abstract
Atherosclerotic cardiovascular disease is the leading cause of mortality in patients with chronic kidney disease (CKD). Measurement of the carotid artery intima-media thickness (CIMT) is being used by many investigators to detect an increased risk of coronary artery atherosclerotic disease and document treatment effects. This study compares CIMT measurements in 75 patients with chronic kidney disease to a matched cohort of 75 subjects with normal kidney function. In plaque-free arterial segments, the CIMT was measured manually in the longitudinal plane from the far walls of a segment of the common carotid artery 3 cm in length adjacent to the carotid bifurcation. Patients with CKD had a significantly higher mean CIMT compared to those with normal renal function (0.86 ± 0.42 mm vs 0.69 ± 0.21 mm; P < .01). Mean CIMT values did not differ significantly between patients with different stages of CKD (stage 3: 0.88 ± 0.14 mm; stage 4: 0.89 ± 0.18 mm; and stage 5: 0.87 ± 0.14 mm, P = .94). These data indicate that CIMT is significantly higher in patients with CKD compared with controls, regardless of the stage of their disease, and may be a readily available noninvasive means of further assessing cardiovascular risk in CKD patients.
Introduction
Chronic kidney disease (CKD) is defined as a glomerular filtration rate (GFR) less than 60 ml/min/1.73m2 or evidence of kidney damage lasting at least 3 months. 1 The affected kidneys may show evidence of structural or functional abnormalities ranging from derangements in markers of kidney function to abnormalities on imaging. Irrespective of the etiology, kidney damage often progresses to end stage renal disease (ESRD), a stage in which the affected individual requires renal replacement therapy over a variable time period. 1
Cardiovascular complications are among the most common complications of CKD, with atherosclerotic cardiovascular disease being the leading cause of mortality in CKD patients. 1 Cardiovascular mortality is 10 to 20 times higher in CKD patients than in the normal population, even after adjustments for age, sex, and hyperglycemia. 2 This association is even more evident in patients on maintenance dialysis, where cardiovascular complications account for 45% of all mortality. 3 The pathologic hallmark of cardiovascular disease is the development of generalized atherosclerosis.
Measurement of the carotid artery intima-media thickness (CIMT) is being used increasingly to detect the presence of atherosclerosis, monitor the progression of atherosclerotic disease, as well as evaluate the effects of treatment. 4 The technique of measurement of CIMT was initially described by Pignoli et al, 4 who demonstrated a correlation between sonographic and histological measurements of the CIMT in vitro. An increased CIMT measurement is now considered a marker of early atherosclerotic vascular changes and increases the risk of future occurrence of stroke and acute coronary syndromes. 5 What is considered to be a significant intima-media complex thickening is defined differently in various studies. 6 However, a CIMT greater than 1.0 to 1.3 mm is generally considered abnormal, and an increase of 0.1 to 0.2 mm in thickness over 5 to 10 years is considered evidence of significant progression and increased risk of cardiovascular events. 7
High-resolution B-mode sonography is a noninvasive, reproducible, and cost-effective method used to measure CIMT and evaluate for the presence of atherosclerotic plaque. 8 The purpose of this study was to compare CIMT measurements in patients with chronic kidney disease to a matched cohort of subjects with normal kidney function.
Materials and Methods
The study was performed on 75 clinically stable CKD patients from the nephrology outpatient clinic in the Lagos University Teaching Hospital, Lagos, Nigeria. It included an equal number of age, body mass index (BMI), and gender-matched control subjects. All the patients had CKD stages 3 through 5 and were hypertensive. For the purposes of this study, CKD was defined as an estimated GFR less than 60 ml/min/1.73m2 and hypertension defined as blood pressure of greater or equal to 140 mmHg systolic or 90 mmHg diastolic or the use of antihypertensive medications to control blood pressure. 9
To be eligible for inclusion into the CKD group, individuals had to be aged between 18 and 64 years, have a glomerular filtration rate less than 60 ml/min/1.73m2, and consent to participate in the study. Inclusion criteria for the control group were age between 18 and 64 years and diagnosis of hypertension but no biochemical or radiologic evidence of kidney disease. Individuals were excluded from the study if they had a history of neck trauma, had suffered a cardiovascular accident in the past, were on maintenance hemodialysis, or had previously been documented to have increased wall thickness and/or atherosclerotic plaques in the carotid arteries. The study protocol was approved by the health research and ethics committee of the hospital, and each study participant provided written informed consent before recruitment into the study.
In addition to documenting each subject’s age and gender, their weights and heights were measured in meters and kilograms, respectively, using a simple standiometer and an electronic weighing scale, respectively. BMI was calculated by dividing the weight in kilograms by the square of the height in meters. 10 For each participant, 2 readings of systemic blood pressure were obtained from both arms using a mercury sphygmomanometer (Accoson, Siemens, Malvern, Pennsylvania) with the patient seated and after resting for 5 minutes. The 2 readings were taken 30 minutes apart, and the higher value was recorded as the patient’s blood pressure.
Blood samples were collected from each patient after an 8- to 12-hour overnight fast. The samples obtained were analyzed for glucose, total cholesterol, urea, and creatinine using appropriate laboratory methods. The GFR was estimated from serum creatinine using the 4-variable version of the modification of diet in renal disease (MDRD) equation established by Levey et al, 11 and these results were used to classify the patient’s stage of CKD. 1 The ultrasonography examination of the carotid arteries were carried out on the same day the blood samples were collected as much as possible.
Ultrasound Protocol
All ultrasonography examinations were performed by a single radiologist (AOK) to eliminate interobserver variability. A real-time ultrasound imager (Toshiba Nemio XG; Kyoto, Japan) with a 6 to 11 MHz multivariable linear transducer was used to acquire the images. The technique used in acquiring the images was the standardized approach to B-mode CIMT measurements previously described by Landwehr et al 12 and is detailed in the following.
The patients lay supine with the neck extended and the head turned slightly away from the side being examined. 8 Ultrasound coupling gel was applied along the sternocleidomastoid muscle and the transducer placed on the neck at the supraclavicular level. The common carotid artery was imaged at this level in the longitudinal plane. 13
The sonographic images were adjusted for optimal visualization of the carotid artery, and the carotid intima-media complex was defined as a band of low-level gray scale echoes that did not project into the lumen between the first and second echogenic lines.14,15 In plaque-free arterial segments, the CIMT was measured manually in the longitudinal plane from the far walls of a segment of the common carotid artery 3 cm in length adjacent to the carotid bifurcation (Figure 1). CIMT was measured as the distance between the leading edge of the first (lumen-intima interface) and second (media-adventitia interface) echogenic lines. 15 The 3 points at which CIMT measurements were obtained were 10 mm below the carotid bifurcation, 5 mm below the carotid bifurcation, and in the carotid bulb bilaterally. The mean of these 3 measurements on each side was determined, and the higher mean value was taken as the CIMT.
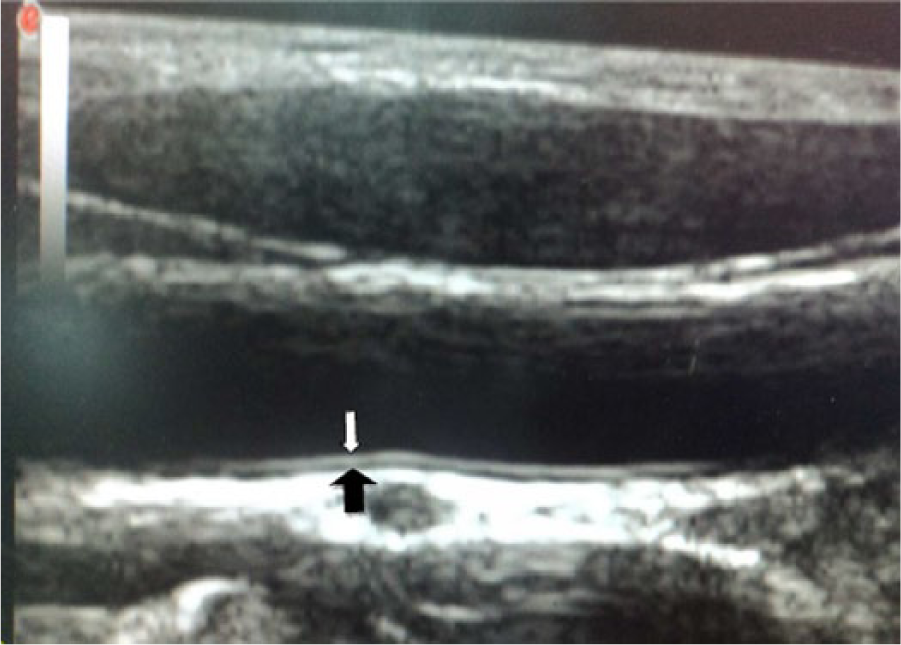
Sagittal image of the distal common carotid artery showing the sites of cursor placement for measurement of the intima-media thickness.
Statistical Methods
The data obtained were analyzed using the Statistical Package for Social Science software for Windows, Version 17.0.1 (SPSS, Chicago, Illinois). Continuous variables are presented as means and standard deviation (SD), while categorical variables are presented as proportions. Comparison between means was done using the Student’s t test and analysis of variance (ANOVA) while comparison between proportions was done using chi-square. In all cases, statistical significance was accepted as P values <.05.
Results
Table 1 shows the clinical and laboratory characteristics of the study population. Compared to the control subjects, patients with CKD had significantly higher mean systolic blood pressure (160.6 ± 3.5 mmHg vs 148.1 ± 22.4 mmHg; P < .01) and higher mean total cholesterol (10.9 ± 3.5 mmol/l vs 8.80 ± 3.95 mmol/l; P < .01). They also had significantly lower mean estimated GFR (32.90 ± 15.90 vs 94.26 ± 30.63 ml/min/1.73m2; P < .01). The distribution of the 75 patients with CKD according to their stage of CKD is shown in Figure 2; the majority of patients (57%) had stage 3 CKD.
Clinical and Laboratory Characteristics of the Study Population.
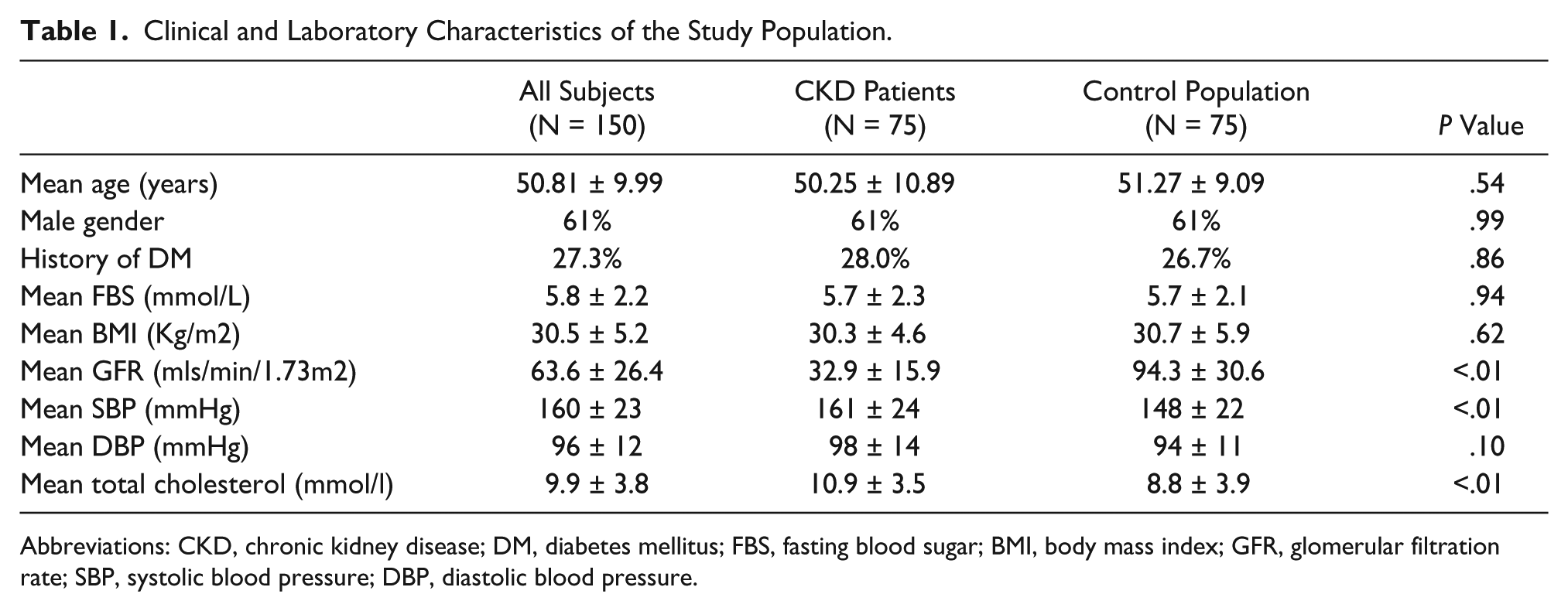
Abbreviations: CKD, chronic kidney disease; DM, diabetes mellitus; FBS, fasting blood sugar; BMI, body mass index; GFR, glomerular filtration rate; SBP, systolic blood pressure; DBP, diastolic blood pressure.
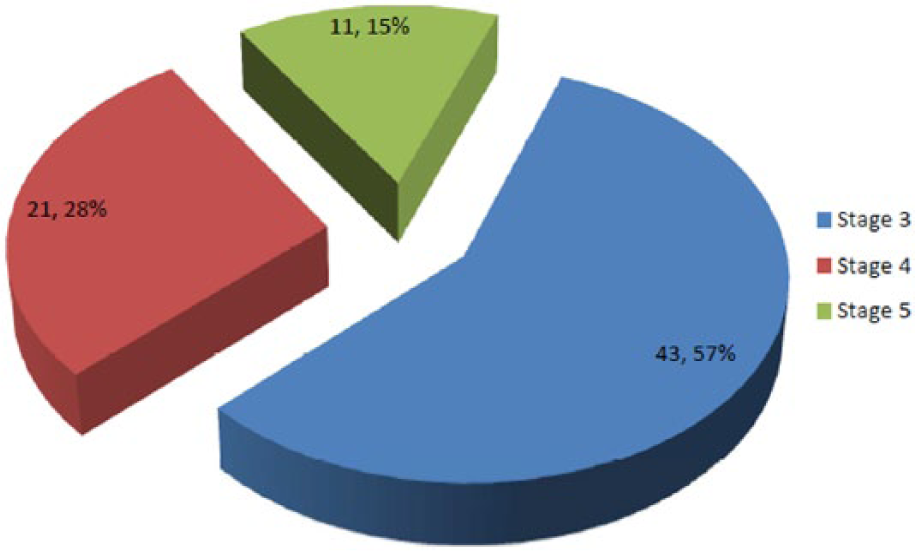
Distribution of the stages of chronic kidney disease (CKD) in the patient group.
As shown in Figure 3, patients with CKD had a significantly higher mean CIMT compared to those with normal renal function (0.86 ± 0.42 mm vs 0.69 ± 0.21 mm; P < .01). However, mean CIMT values did not differ significantly between patients with different stages of CKD (stage 3: 0.88 ± 0.14 mm; stage 4: 0.89 ± 0.18 mm; and stage 5: 0.87 ± 0.14 mm, P = .94) (Figure 4).
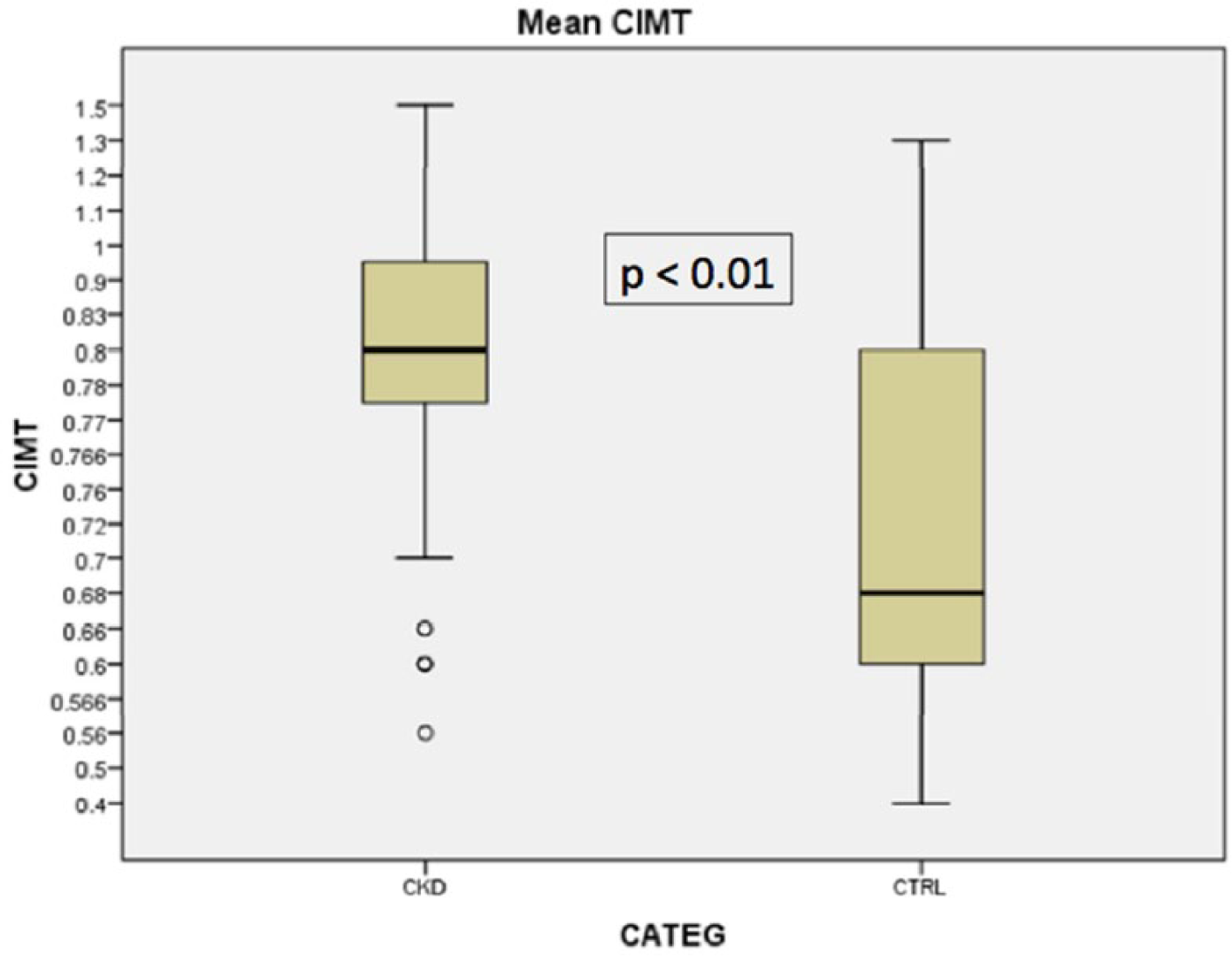
Comparison of the mean carotid intima-media thickness (CIMT) between the patients with chronic kidney disease (CKD; 0.86 ± 0.42 mm) and the control group with normal renal function (CTRL; 0.69 ± 0.21 mm, P < .01).
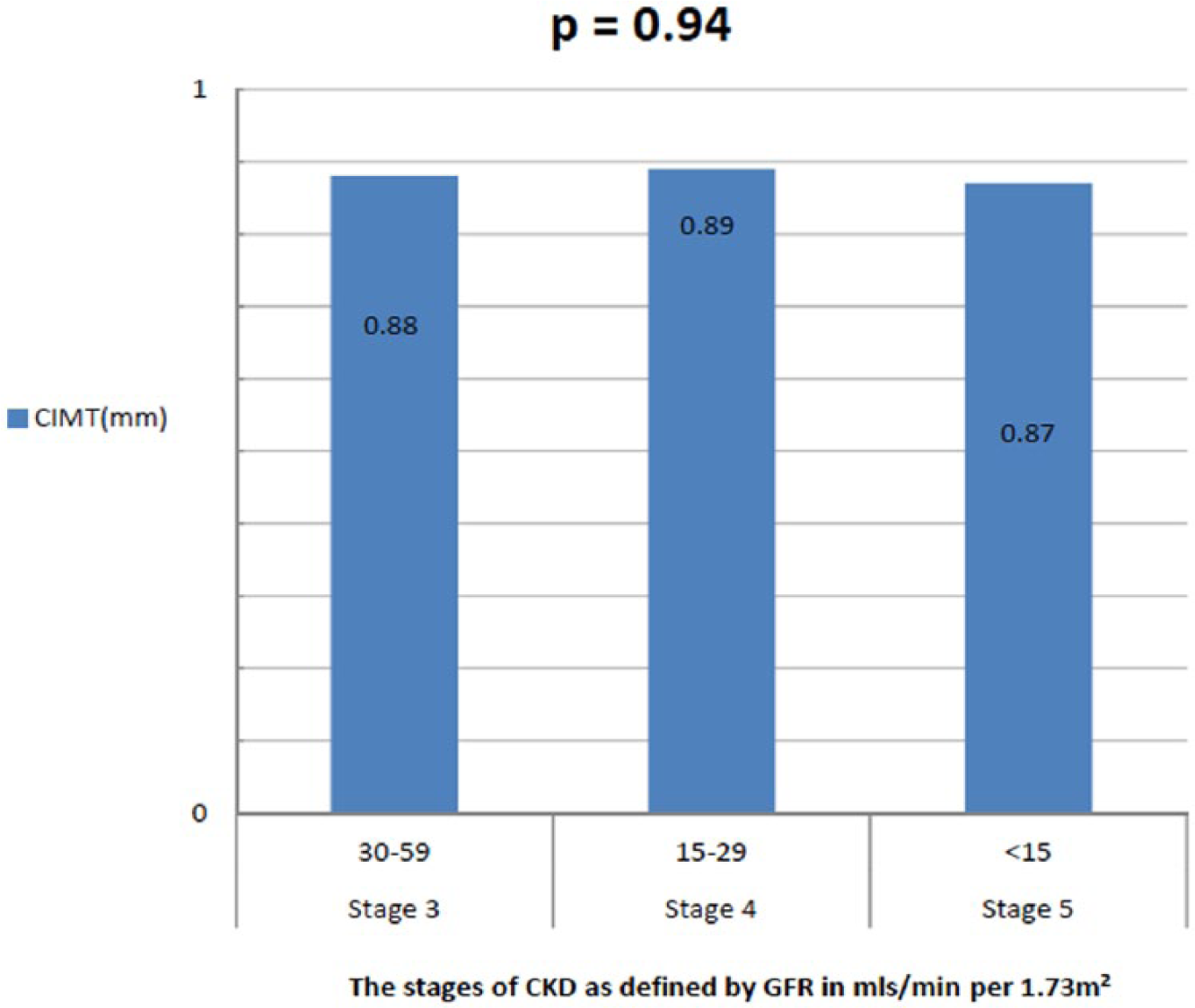
Comparison of the mean carotid intima-media thickness (CIMT) between subjects in the patient group as a function of their stage of chronic kidney disease (CKD).
Discussion
The major finding of this study was that mean CIMT was significantly higher in patients with CKD than in the control group (0.86 ± 0.42 mm vs 0.69 ± 0.21 mm). This finding is similar to those previously reported in the literature.15,16 Since CIMT has been consistently shown to be a marker of the early stages and presence of atherosclerosis and by necessary implication a pointer to increased cardiovascular risk, 8 this finding is in keeping with what is known about cardiovascular risk in patients with CKD being significantly higher than in individuals without CKD. The patients with CKD in this study were compared with age- and gender-matched controls who all had hypertension and had similar rates of diabetes and blood sugar control. This is in contrast to many of the earlier studies that used otherwise healthy individuals as controls.8,15,17 The finding of higher CIMT values in patients with CKD compared to the control group in this study suggest that CKD may increase cardiovascular risk independent of the presence of traditional cardiovascular disease risk factors.2,18
There was no significant difference in the mean CIMT values between patients with different stages of CKD in this study. This is similar to the findings reported by Chhajed et al. 17 This finding suggests that in adult Nigerians with CKD, the mere presence of significantly impaired kidney function, rather than the degree of impairment of renal function, was responsible for the increases in CIMT. Although not shown here, this was further buttressed by the fact that apart from the mean total cholesterol values, there was no significant difference in most of the traditional risk factors for cardiovascular disease between patients in the different stages of CKD. Uremia-related risk factors that are prevalent among CKD patients such as anemia, altered calcium/phosphate homeostasis, vascular inflammation, and oxidant stress are known to contribute to the accelerated atherosclerosis and abnormal vascular remodeling among patients with CKD. 19
The absolute values of mean CIMT (0.86 ± 0.42 mm vs 0.69 ± 0.21 mm) in this study were comparable to those reported by Shoji et al 16 and Broszko et al 15 but lower than those reported by Benedetto et al 20 (1.02 ± 0.22 mm). A possible explanation for this difference from the latter study is the cohort of patients studied by Benedetto et al were on long-term dialysis, whereas the patients in this study had mostly stages 3 and 4 CKD. Patients on maintenance hemodialysis have been shown to have more advanced cardiovascular disease than other patients with CKD who are not on dialysis, and they may therefore be expected to have greater thickening of their carotid intima-media complex. 21 Interestingly, the mean CIMT values in our study (0.86 ± 0.17 mm and 0.69 ± 0.21 mm) are also significantly lower than those reported even in otherwise healthy Nigerians by Okeahialam et al, 22 who compared 3 cohorts of adult Nigerians living in Jos (healthy individuals, diabetics, and hypertensives). The reason for this difference is not immediately clear; however, it suggests that CIMT values may vary based on locality, even within the same country, and this reinforces the need for the establishment of normative values for each region before implementing the widespread use of CIMT in evaluating risk of cardiovascular diseases.
Conclusion
CIMT is significantly higher in patients with CKD compared with controls and as such, may be an important noninvasive and inexpensive and readily available mean of assessing cardiovascular risk in CKD patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.