
Abstract
Leriche syndrome, also referred to as aortoiliac occlusive disease, is complete occlusion of the infrarenal aorta and bilateral common iliac arteries. The development of collateral pathways allows reconstitution of arterial blood flow to the lower extremities, preventing limb ischemia. Patients typically present with a triad of symptoms, which include intermittent claudication of the buttocks and thighs, decreased or absent femoral pulses, and impotence in men. Sonography may play a significant role in diagnosing Leriche syndrome, particularly in cases with contraindications to other more invasive tests. Knowledge of the presentation of aortoiliac occlusion along with recognition of developing collateral pathways assists with the diagnosis and management of this disease.
Keywords
Leriche syndrome, or aortoiliac occlusive disease, is complete occlusion of the distal aorta and bilateral common iliac arteries. Described in 1940 by the French surgeon Rene Leriche, this disease is recognized by its triad of symptoms, which include intermittent claudication of the buttocks and thighs, decreased or absent femoral pulses, and impotence in men. More acute or severe symptoms are prevented by the development of a network of collateral pathways that supply blood to the internal and external iliac arteries. Although sonographic evaluation of the distal aorta and iliac arteries for occlusion can be difficult because of their deep location in the body, high-quality imaging and hemodynamic evaluation are becoming more achievable with advanced technology. Increased familiarity with the disease and its clinical and sonographic presentation allow rapid diagnosis and increase the chances of a better outcome after treatment.
Case Report
A woman late in her fifth decade presented to a vascular physician. She complained of cold extremities and intermittent claudication bilaterally of the hips, thighs, and calves. She also had complaints of abdominal, back, and chest pain. One year previously, the patient was diagnosed with chronic abdominal aortic occlusion but had declined treatment at that time. On her current visit, she stated her symptoms were worsening, including the onset of ischemic rest pain. Upon physical examination, both the right and left common femoral arteries were nonpalpable. The patient’s history was significant for heavy tobacco use, hypertension, and diabetes mellitus. An aortoiliac duplex sonogram, ankle brachial index with toe pressure (ABI/TP), and computed tomographic angiogram (CTA) were ordered.
A curvilinear transducer with a center frequency of 5 MHz was used on a Philips iU22 machine (Philips Healthcare, Andover, MA). The study showed the proximal aorta measured 2 × 2.3 cm (anterior-posterior × transverse) with a biphasic waveform and peak systolic velocity of 60 cm/s. The mid aorta measured 2 × 2 cm with a blunted, staccato-like monophasic waveform and a peak systolic velocity of 28 cm/s (Figure 1), which was significantly diminished compared with normal mid-distal aortic values of 60 to 100 cm/s. The distal aorta and both common iliac arteries showed no evidence of blood flow; however, numerous collateral vessels were noted (Figures 2–4). There was monophasic flow seen in the bilateral external and internal iliac arteries. The ABI suggested only moderate peripheral arterial disease, with the right leg measuring 0.71 and the left leg measuring 0.72. Continuous wave Doppler recordings showed a monophasic common femoral artery waveform with a decrease in wave amplitude. The femoral brachial index was not obtained since segmental pressures were not performed. The CTA confirmed the sonographic findings, showing complete occlusion of the distal aorta and bilateral proximal common iliac arteries (Figure 5). The distal common iliac arteries were reconstituted by large paravertebral collateral vessels (Figure 6). The hypogastric arteries and bilateral external iliac arteries were patent. Based on the findings, the patient was diagnosed with Leriche syndrome. Because of complaints of chest pain and other escalating symptoms, the patient was referred on an emergent basis for admittance and management.
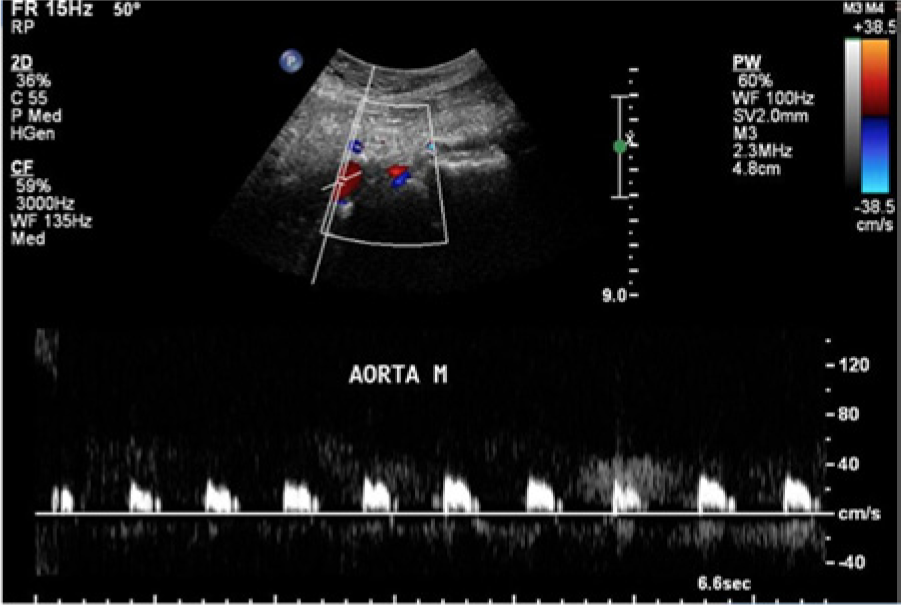
Sagittal color/spectral Doppler image of the mid aorta showing a blunted, staccato-like monophasic waveform characteristic of a more distal occlusion.
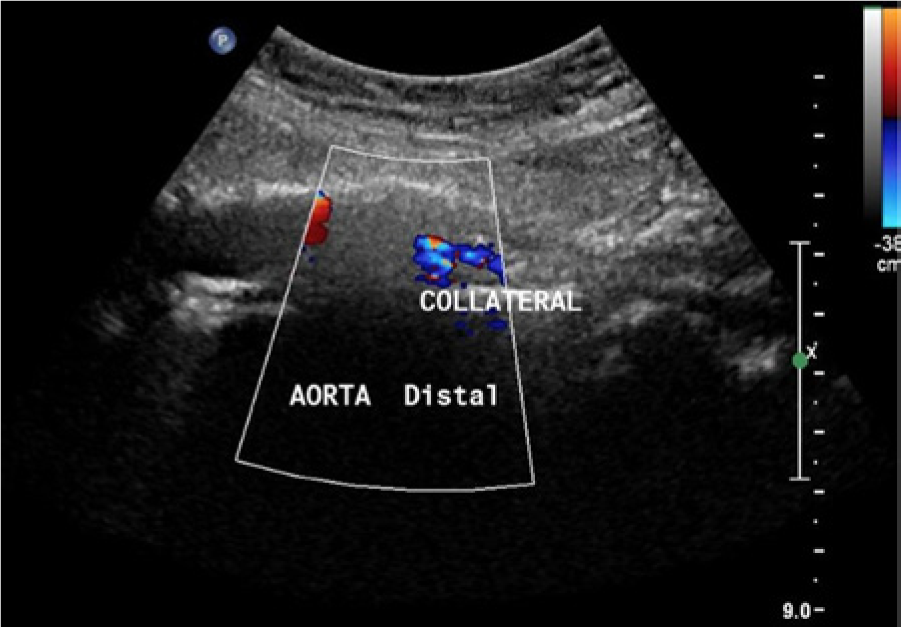
Sagittal color Doppler image of the distal aorta with no detectable evidence of blood flow. Note that evidence of blood flow is seen in a parallel collateral vessel.
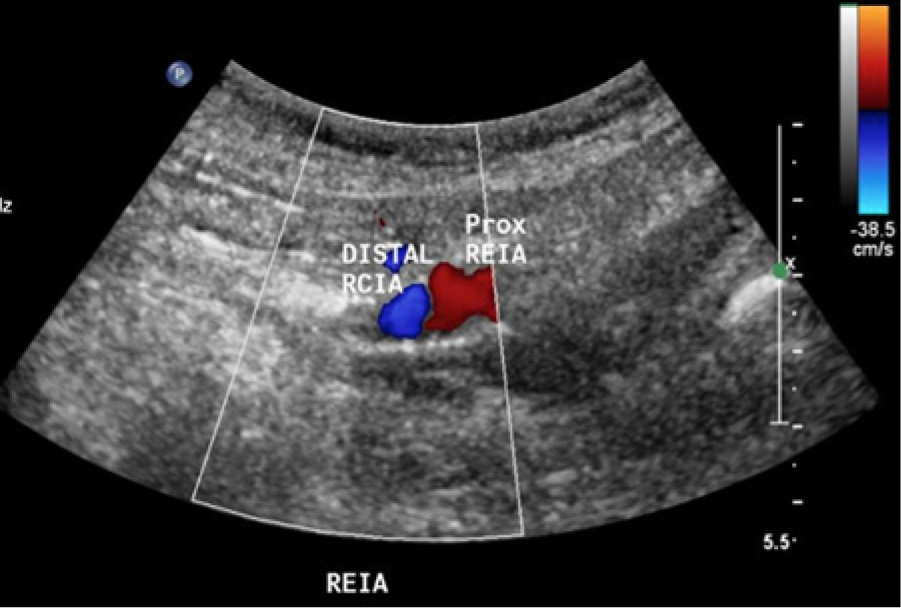
Sagittal color Doppler image showing blood flow detected in the right distal common iliac artery/proximal external iliac artery. Note that the color image shows retrograde flow in these segments, consistent with collateral filling of some more distal portion of the external iliac artery. No flow was seen in the proximal common iliac artery.
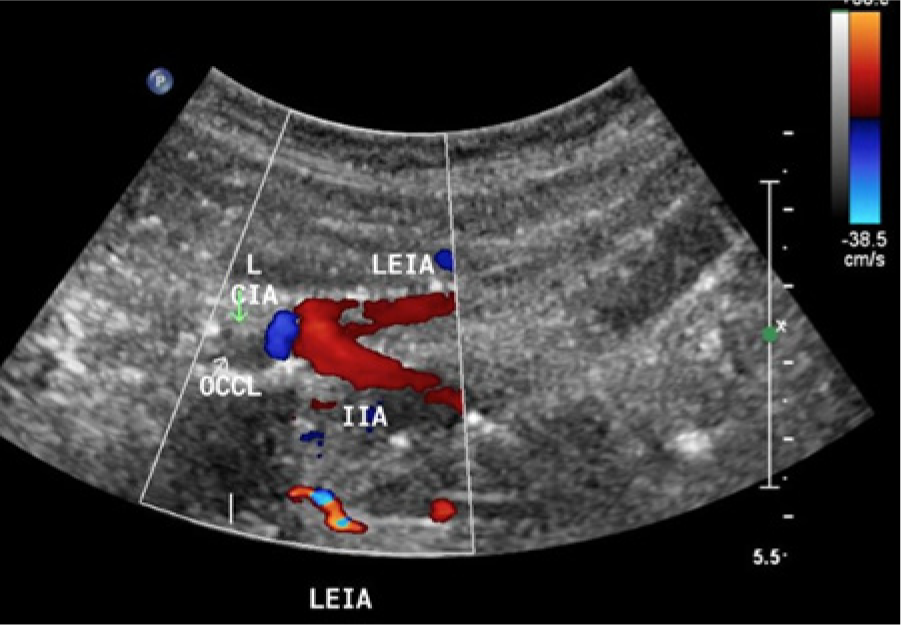
Sagittal color Doppler image of the left iliac artery system showing a complete occlusion of the common iliac artery with reconstitution of the internal and external iliac arteries. Color Doppler imaging shows retrograde flow in the left internal iliac artery consistent with more distal collateral filling, with subsequent antegrade flow into the external iliac artery.

Computed tomographic arteriogram showing complete occlusion of the distal aorta and bilateral common iliac arteries. Note the large collateral vessel (arrow).
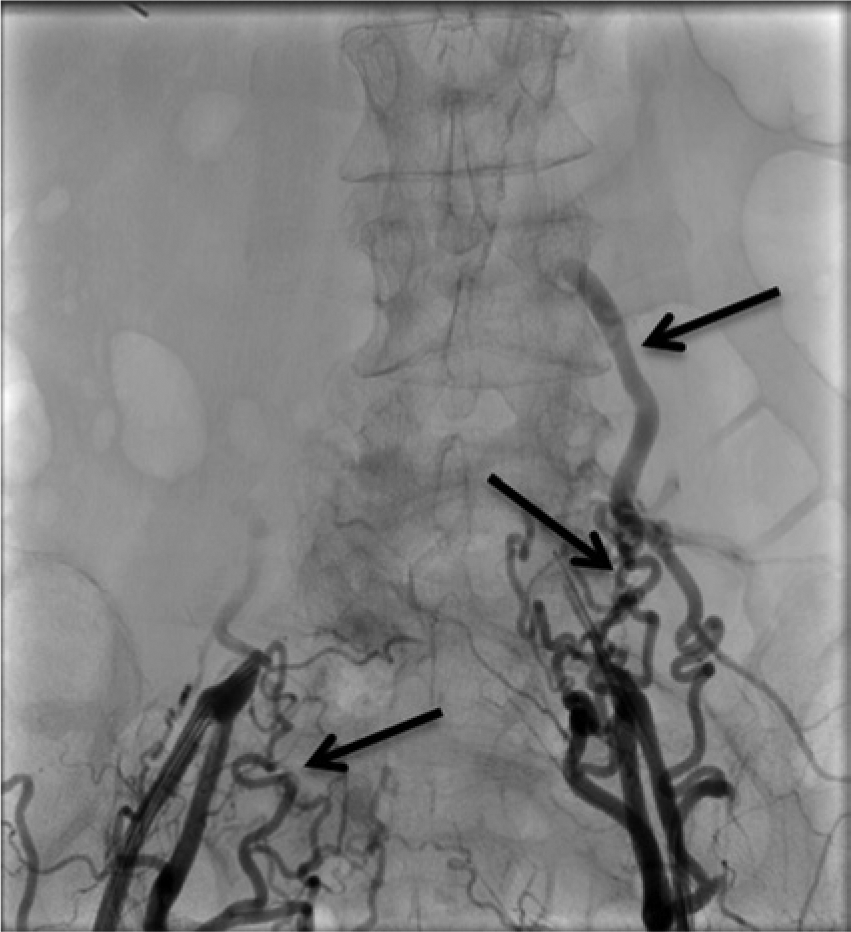
Preoperative angiography showing complete occlusion of the distal aorta and bilateral common iliac arteries with large collateral vessels (arrows) reconstituting the internal and external iliac arteries.
Although the patient’s aorta and common iliac arteries were completely occluded, the surgeon was able to place an endovascular aortic stent guided by preoperative angiography (Figure 6). A few days after surgery, the postoperative angiogram showed a widely patent distal aorta and common iliac arteries, with absent collateral pathways (Figure 7). An ABI was performed a few weeks after the surgery at a routine follow-up visit and showed a normal study, with the right leg measuring 1.00 and the left leg measuring 1.02.

Postoperative angiography showing a widely patent aorta (black arrow) and iliac arteries (white arrows). Note that the previously seen large collateral vessels are no longer visualized.
Discussion
Leriche syndrome is most frequently associated with a chronic condition of atherosclerotic plaque at the level of the aortic bifurcation that eventually occludes the infrarenal abdominal aorta and one or both common iliac arteries. The occlusion usually begins in one iliac artery, extends toward the bifurcation, and then invades both the aorta and the opposite common iliac artery. 1 Atherosclerotic occlusions of the aorta account for 8% to 28% of all arterial occlusions. 2 Leriche syndrome has an atypical distribution, affecting the large central arteries of the abdomen and pelvis, while smaller arteries are usually unaffected. 3 Proximal propagation of the occlusion to the visceral arteries can occur, although this is rare.4–6 Aortic occlusions can be caused by other entities, such as an embolus, vasculitis, or trauma, although these are less common than atherosclerosis. 7 Risk factors include smoking, dyslipidemia, hypertension, diabetes mellitus, male gender, advanced age, and a high genetic risk. 8
Patients usually present with a triad of symptoms which include intermittent claudication of the buttocks and thighs, absent or decreased femoral pulses, and impotence in men. 3 Upon physical examination, an absent or diminished femoral pulse is usually discovered. In some patients, pulses could be palpable but disappear with ambulation and the onset of claudication. 8 Other clinical symptoms may occur depending on the severity of the disease, such as limb ischemia and muscle atrophy; however, most patients are relatively asymptomatic because of the development of large, extensive collateral vessels between abdominal, pelvic, and infrainguinal arteries. 9
The development of collateral pathways for arterial blood flow is a hallmark sign of chronic obstruction seen with Leriche syndrome. Contributions from different collaterals depend on the level of aortic occlusion, the severity of the obstructive process, and the patency of other possible collaterals. 10 Two common collateral pathways that develop are designated systemic-systemic and viscero-systemic pathways. The systemic-systemic collateral pathways derive from the embryologic segments of the dorsal aorta and include the intercostal, lumbar, internal mammary, deep circumflex iliac, and inferior epigastric arteries.9,11 Distal abdominal aorta occlusion, which is seen in Leriche syndrome, tends to collateralize through systemic-systemic pathways. 9 The viscero-systemic collateral pathway consists of a single vessel that is continuous from the superior mesenteric artery (SMA) to the internal iliac arteries. 11 The middle colic branch of the SMA joins the left colic branch of the inferior mesenteric artery and continues into the pelvis as the superior hemorrhoidal artery. 11 This communicates with the middle hemorrhoidal branches of the internal iliac artery. This pathway is more prevalent if the aortic occlusive disease extends cephalad along the aorta, approaching the renal arteries. 9 These collaterals bypass the occluded portion of the aorta and provide necessary blood flow to the lower extremities, thus preventing significant limb ischemia.
Noninvasive laboratory testing helps confirm the diagnosis, establishes a baseline for follow up, and assesses therapeutic outcomes. ABIs, segmental pressure measurements, and pulse volume recordings are the 3 most commonly used noninvasive modalities. 8 Leriche syndrome typically presents as an inflow problem, with a decrease in the thigh brachial index and pulse wave amplitude. A difference of at least 20 mm Hg between the brachial pressure and the decreased proximal thigh pressure reflects a significant stenosis in the aorta and/or iliac arteries. 8 Initially, the ABI may even be normal in patients with aortoiliac disease, but there is a notable reduction after the patient exercises. CTA, magnetic resonance angiography, and digital subtraction angiography also are commonly used modalities for diagnosis of peripheral arterial occlusive disease, but all have many contraindications. 8 Because of these limitations and the continuous advancement in technology and improvement in the skill and training of sonographers, sonography plays a significant role in the diagnosis and management of patients with aortic disease. Arterial occlusion is diagnosed on the basis of absent blood flow and damped arterial Doppler waveforms distal to the occluded segment. 12 When using color Doppler imaging, it is very important during the examination to decrease the color scale and increase the gain to be able to detect low-velocity flow so as not to miss a trickle of flow in a highly stenosed, nearly occluded vessel. Use of power Doppler will aid in the diagnosis, and spectral Doppler will provide confirmation of an occlusion. Spectral Doppler measurement of peak systolic velocity (PSV) and spectral waveform analysis in the common femoral artery (CFA) can be used additionally as a reliable diagnostic tool to indirectly predict aortoiliac occlusion. 13 A monophasic waveform with no reverse diastiolic flow, combined with a PSV of <45 cm/s in the CFA, is highly predictive of iliac occlusion.13,14 Compared with the normal triphasic waveform, a monophasic waveform indicates severe proximal obstruction and low resistance of the distal vascularity resulting from vasodilation and possible inflammation in response to the ischemic change. 13 When there is presence of visceral collateral circulation, the upstroke of the systolic portion of the spectral waveform is not as rapid because of the relatively slow flow in the collateral arteries. 13 Recognizing that a large, dilated collateral vessel is not a patent aorta or iliac artery is also imperative. This identification is aided by knowledge of anatomy and by paying close attention to the waveform, velocity, and pathway of each vessel.
Surgical intervention is indicated in patients with disabling claudication and/or ischemia at rest manifested by rest pain in the foot, ischemic ulceration, or pregangrenous skin changes. 15 The combination of angioplasty and stenting has become first-line therapy for most patients with Leriche syndrome.8,16 Open surgery with a bypass graft is typically used for patients who have had unsuccessful endovascular treatments or patients with more extensive disease.8,16 It is important that notable collateral pathways are reported because they can change surgical management. 17 This is usually done with CTA or conventional angiography so that the exact location of the collateral is clear. Disturbing these collaterals during surgical intervention could destroy the blood supply to the lower extremities.8,17,18 In some cases, interruption of critical collaterals cannot be avoided, so limb viability should be monitored closely after operation. 17
Conclusion
Leriche syndrome is complete occlusion of the infrarenal aorta and bilateral common iliac arteries that usually results in intermittent claudication of the buttocks and thighs but may present with more severe symptoms such as ischemic rest pain. Sonography is a useful tool in detecting absent blood flow in the aorta and iliac arteries, evaluating for arterial collateralization seen with chronic obstructive disease and assessing distal vascularization. By correlating the clinical signs and symptoms with the sonographic findings, sonography is able to play a major role in the diagnosis of Leriche syndrome.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.