
Abstract
Joint replacement is becoming a more common surgical procedure, and it may have unusual or unexpected postoperative complications. This case report discusses the evaluation of a large pelvic mass first noted on physical examination and ultimately diagnosed by sonography and computed tomography as a chronic hematoma resulting from a failed total left hip arthroplasty.
More than five decades have elapsed since the widespread adoption of total hip arthroplasty for the treatment of arthritic disorders of the hip joint.1,2 The treatment has proved to be one of the most important surgical developments of the 20th century, providing substantial pain relief and improved quality of life for chronic arthritic conditions in elderly patients. As life spans are increasing, however, prostheses designed to last 15 to 20 years may require revision surgery to replace aging or failing hardware. With these additional surgeries come added risks and possible complications.
Case Report
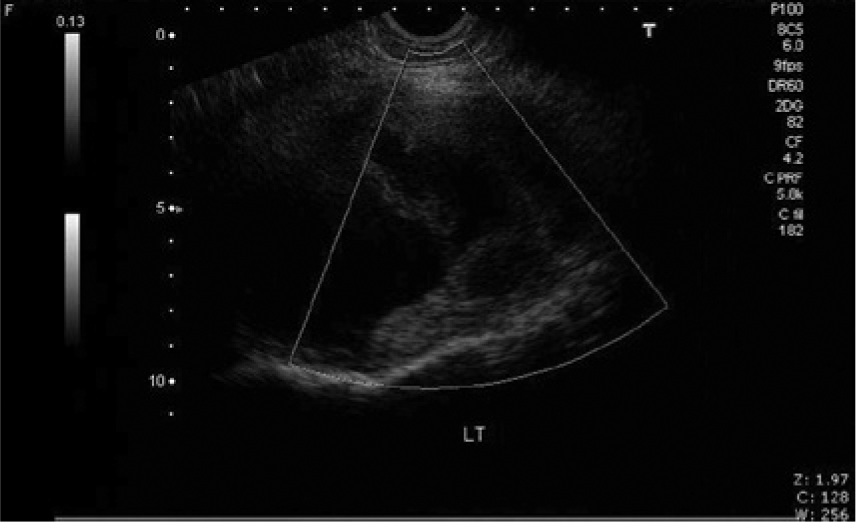
A woman in her early 50s presented to her primary care physician complaining of increasing sciatic-like pain originating in her lower left back and extending down her left leg. The pain had become progressively debilitating and caused significant difficulty with walking. Physical examination by her nurse practitioner revealed a large, firm, fixed mass in the left pelvis. The mass was not painful to palpation. The patient’s medical history was significant for bilateral total hip replacements. The left hip had been replaced in 1991 and had required at least one revision over the following 11 years. The patient was referred to our imaging center for a pelvic sonogram to evaluate the pelvic mass as well as for left hip radiographs. The sonographic examination was performed on a Toshiba Nemio (Tustin, California) ultrasound system. The initial transabdominal examination used a standard 6.0-MHz curved-array transducer. The urinary bladder, uterus, and ovaries appeared normal. In the lateral left pelvis, adjacent to the iliac bone, there was a large 11.6 × 12.5–cm complex mass (Figures 1 and 2). Power and color Doppler evaluation demonstrated no internal or peripheral vascular flow (Figure 3). Transvaginal examination using a 6-MHz endovaginal transducer confirmed a normal uterus and ovaries. Because of its very lateral location, the mass was difficult to image with the endovaginal probe, but it appeared clearly separate from the left ovary.

Sagittal sonographic image showing complex echogenicity within the large 11.6-cm left pelvic mass.

Transverse sonographic image showing similar complex echogenicity within the large left pelvic mass.
Power Doppler image of the pelvic mass showing absence of any vascularity within the mass.
On the anteroposterior (AP) pelvis radiograph, there were multiple calcifications associated with a soft tissue mass in the left pelvis (Figure 4). The acetabular component of the left hip prosthesis appeared to extend beyond the boney margins of the ilium and appeared associated with the calcified mass. Computed tomography (CT) examination was recommended for further evaluation. The CT was performed at another facility using a multidetector scanner. The examination showed what appeared to be a predominantly homogeneous cystic mass along the left side of the pelvis. (Sonography had more clearly defined an echogenically complex nature of the mass, as seen in Figures 1 and 2.) By CT, the mass measured approximately 10 × 9 × 14 cm. There were some radiopaque foci identified inferiorly in the mass representing either calcifications or heterotopic bone formation, although the coronal CT views were somewhat obscured in this region by metallic artifacts associated with the prostheses. The medial wall of the left acetabulum was poorly marginated, and the tip of one of the surgical screws was seen to extend into the lateral portion of the cystic mass (Figures 5–7). The consulting orthopedist believed that the mass was likely the consequence of a failed hip prosthesis and that it likely was a complex chronic hematoma.

Anteroposterior pelvic radiograph showing diffuse calcifications within the left pelvic mass.

Coronal computed tomographic image showing a large left pelvic mass with the appearance of a homogeneous texture.

Axial computed tomographic image showing the large mass, again with the appearance of a more homogeneous texture.
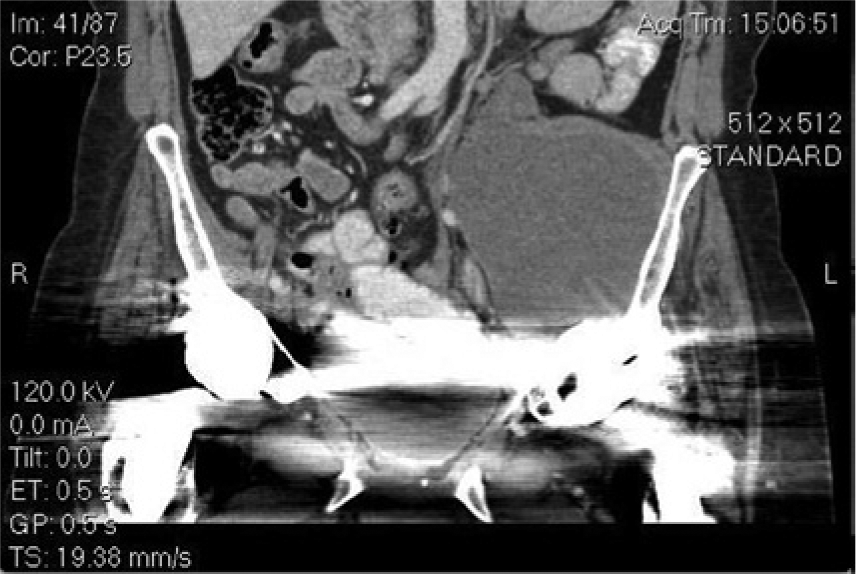
Coronal computed tomographic image showing a surgical screw extending into the pelvic mass; inferior edge calcifications/heterotopic bone formation are somewhat obscured by the metallic artifacts associated with the prosthesis.
The patient was scheduled for a left hip arthroplasty and revision. Using a direct anterior approach as in previous surgeries, the musculature and fascia were incised and mobilized, exposing the left hip. After removing the metallic femoral head, it was noted that the acetabular component of the prosthesis had shifted to a more retroverted position. After meticulous removal of the metal prosthetic cup and screws, a large retroacetabular hematoma was identified internally to an area of eroded bone within the ilium. Using suction, the majority of the hematoma, which measured approximately 2000 mL, was evacuated. Numerous other soft tissue components associated with the hematoma were removed as well. Revision of the hip joint was completed with bone grafting and replacement of the old prosthetic hardware. Upon successful completion of the repair, the patient was sent to recovery in good condition.
Pathologic evaluation of the removed operative tissues revealed fibrous tissue with focal areas of necrosis, scattered dystrophic calcifications, focal foreign body giant cell reaction, areas of myxoid change, and mild chronic inflammatory changes with focal new bone formation.
The patient’s postoperative course was uneventful, and currently she enjoys significant pain relief and is ambulating well. No further imaging studies have been performed.
Discussion
The earliest recorded attempts at hip replacement were carried out in Germany in the 1930s, using ivory to replace the femoral head. 1 While the use of artificial hips became more widespread in the 1950s, the modern artificial joint owes much to the work of John Charnley at the Manchester Royal Infirmary. 2 His work resulted in a design that completely replaced the other designs by the 1970s. Charnley’s design consisted of three parts: (1) a metal femoral component, (2) a polyethylene acetabular component, and (3) special bone cement. The replacement joint, which was known as the low-friction arthroplasty, was lubricated with synovial fluid. In the past few decades, several evolutionary improvements have been made in the total hip replacement procedure and prosthesis. Many hip implants are made of a ceramic material rather than polyethylene, which some research indicates dramatically reduces joint wear. 3 Metal-on-metal implants are also gaining popularity. 4 Currently, over 400,000 hip replacements are performed in the United States annually. 5 Although this surgery has a high success rate, approximately 10% of implants will fail and require revision. In addition, as life spans are increasing, prostheses designed to last 15 to 20 years may require revision surgery to replace aging or failing hardware. 5
Implants may fail for any of several physiologic reasons: loosening, infection, dislocation, or other patient-related factors.6–8 Common to all joint revisions is an assessment of existing bone quality, removal of the failed components, reconstruction of remaining bone and soft-tissue structures, and successfully fixing the new components to the bone. A revision of a hip replacement is generally more challenging than the initial operation, and the results of surgery and the durability of the revised hip replacement are less predictable than those of the primary operation. With every revision surgery, there is some loss of muscular mass, bone, or both. The duration of surgery is generally longer and the likelihood of complications higher than during the primary surgery.9–13
As human life expectancy continues to increase, revision arthroplasty is becoming more common. At the same time, musculoskeletal ultrasound (MSK) is becoming increasingly popular as a diagnostic tool to evaluate damaged or diseased joints prior to and after surgical intervention. 14 With regard to the hip, MSK sonography is remarkably good in the investigation of joint and bursal effusion, tears of the peripheral margins of the labrum, hip dysplasia, and arthritic changes of the femoral head. 15 MSK sonographic evaluation of postarthroplasty hips includes identification of joint effusion for possible sepsis, muscular hematoma, pseudo-tumor formation, and mechanical dislocations.16–18 Advances in sonographic resolution and overall image quality will no doubt increase its diagnostic capabilities.
Conclusion
This patient’s multiple hip revisions with accompanying loss of acetabular bone and a protruding surgical screw tip likely led to the formation of the pelvic hematoma. While hematomas are typically a more immediate postoperative consequence of primary or revision hip surgery, a review of the literature could find no past reports describing such a chronic and large intrapelvic hematoma mimicking a pelvic mass.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.