
Abstract
Smartphones are one of the most widely used cell phones in the United States today. They perform multiple functions, and in April 2009, another capability was added to that list. Smartphones are now able to display sonographic images of the human body and organs through use of a smartphone-compatible ultrasound probe. The probe can be plugged into the USB slot of a smartphone and used to allow gray-scale image visualization. This article discusses the function and structure of this new and emerging technology while looking at the impact of this technology on the field of sonography.
Technologic advances over the years have had a significant impact on sonography, for both image-processing systems and ultrasound probes.1,2 Probe technology in particular has seen evolvement from static single-crystal systems to mechanical sector scanners to linear arrays and real-time 3D systems. A recent addition to this technology is an ultrasound probe compatible with a smartphone.3,4 This article discusses this emerging technology considering the physics, development, function, and the potential applications of a smartphone system, along with the limitations and disadvantages of such a system.
The Smartphone Probe
In April 2009, two investigators at Washington University in St Louis announced the development of a smartphone-compatible ultrasound probe (Figure 1). 5 The work represented the culmination of two and a half decades of research and development, reducing the size of the system from a full electronic cabinet to a small 1 × 3–inch circuit board (Figure 2). The size of the device allows physicians and sonographers to use a mobile device small enough to fit easily in the hand (Figure 3a,b and Figure 4). The present system is only compatible with Windows (Microsoft, Redmond, Washington)–based smartphones. The technologic challenges that had to be overcome were primarily the trade-offs associated with battery power consumption and the speed of data transfer. A secondary challenge was creation of the necessary algorithms that allowed the display of the image on the smartphone screen. A device was approved for use by the Food and Drug Administration (FDA) in 2011 after meeting strict regulatory requirements for medical “apps.”6,7 Today a variety of specialized probes have been developed covering a frequency range of 2 to 18 MHz. These probes can be plugged into a USB port not only on smartphones but also tablets, laptops, and desktop computers. The probes can be used for typical applications in imaging such structures as the liver, kidney, bladder, and endocavitary applications, with special-purpose probes designed for applications such as very high-frequency imaging, ultrasound guidance for biopsies, vascular access, and central line placement (Figures 5 and 6).

Photograph of a smartphone probe connected to the USB port of a Windows operating system–based mobile phone. From http://billkosloskymd.typepad.com/wirelessdoc/2009/05/ultrasound-imaging-with-smartphones-using-a-usbbased-probe.html
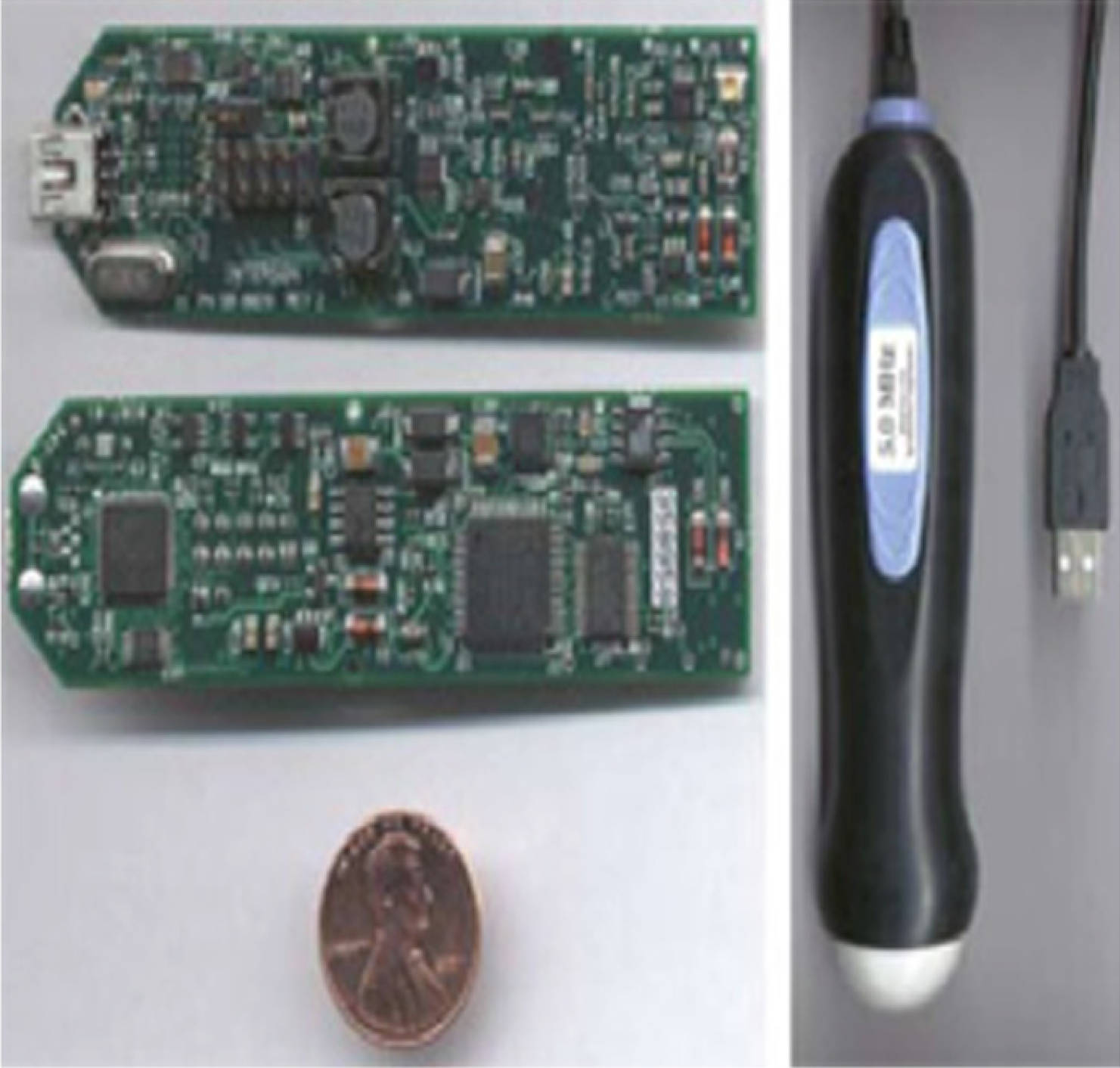
Current size of the printed circuit board (approximately 1 × 3 inches, shown with a penny for comparison) used for the smartphone probe. From www.medgadget.com/2009/04/mobile_clinical_imaging_on_a_smart_phone.html
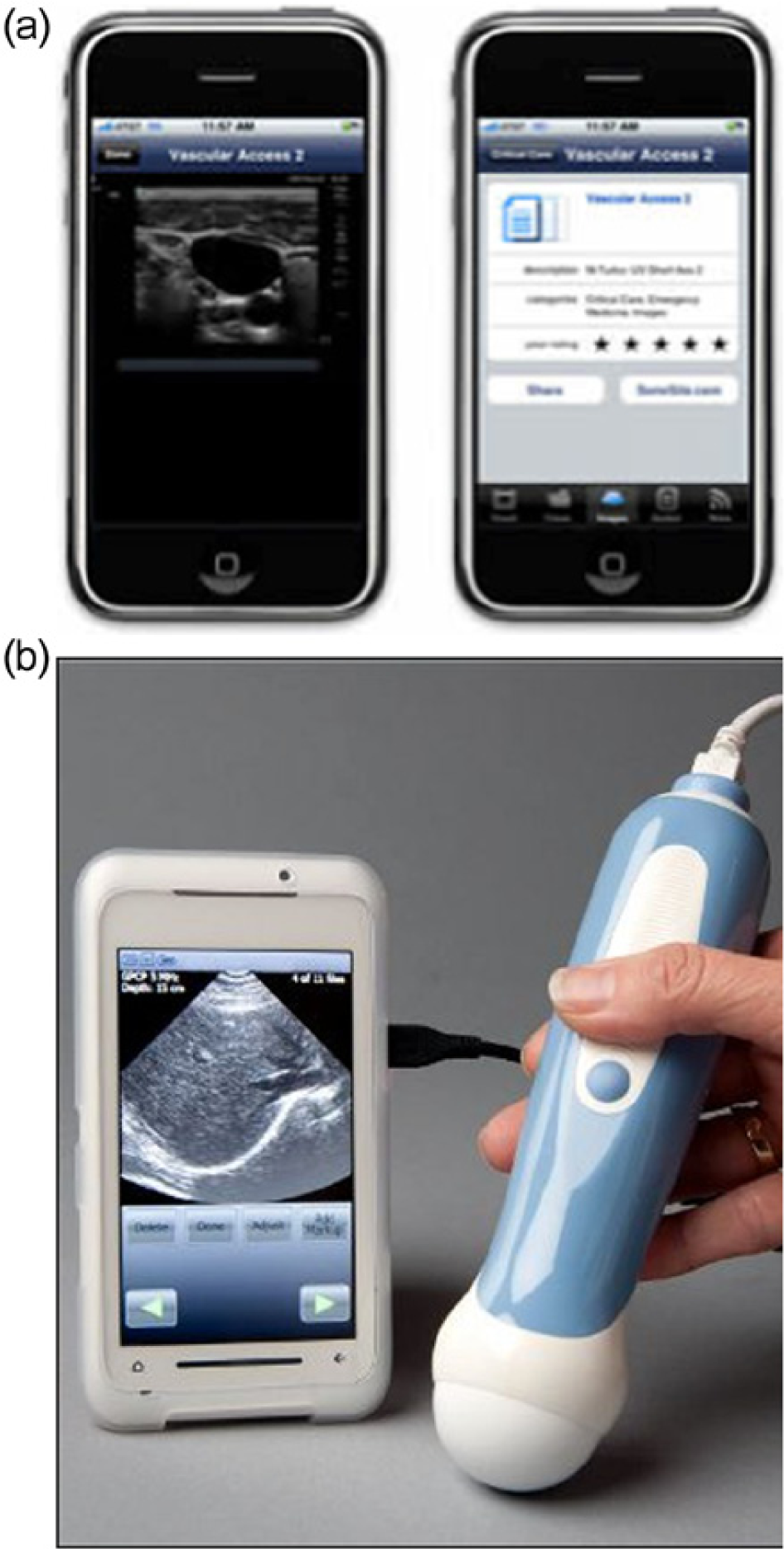
(a, b) Gray-scale sonographic images displayed on a smartphone. From (a) http://gpsmedical.typepad.com/gps_medical/page/2/ and (b) https://www.engineeringforchange.org/news/2011/06/02/ultrasound_is_now_on_smart_phones.html

Smartphone probe being used to evaluate the carotid artery. From http://www.gizmag.com/ultrasound-images-a-snap-with-a-smartphone/11556/
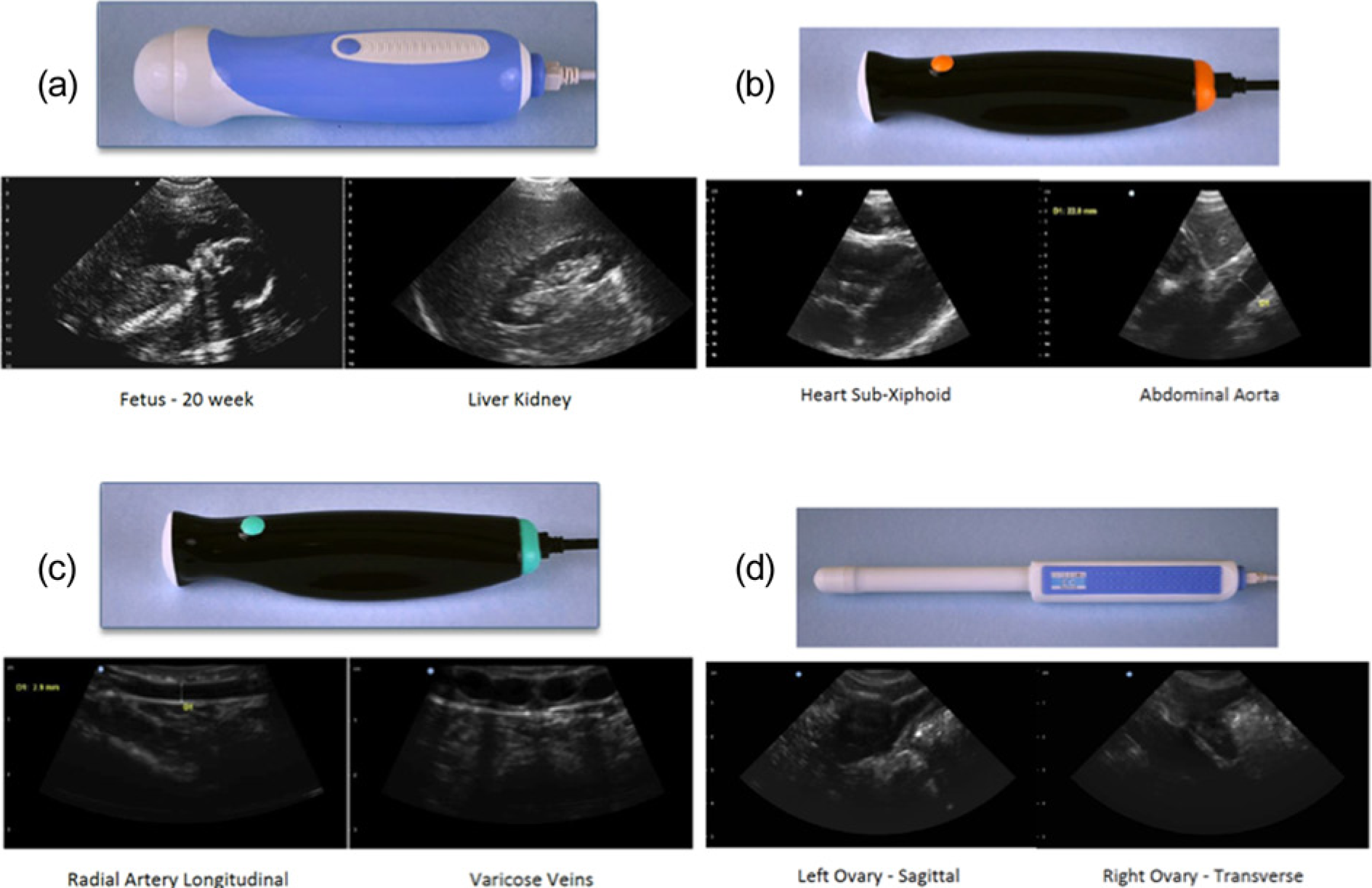
A wide variety of probe types that plug into a USB port are currently available. (a) Abdominal probe, frequency range 3.5 to 5 MHz; (b) general-purpose probe, frequency range 3.5 to 5 MHz; (c) vascular probe, frequency range 8 to 24 MHz; (d) endocavitary probe, frequency range 7.5 to 24 MHz. From http://www.interson.com/products/seemore-153-usb-probes
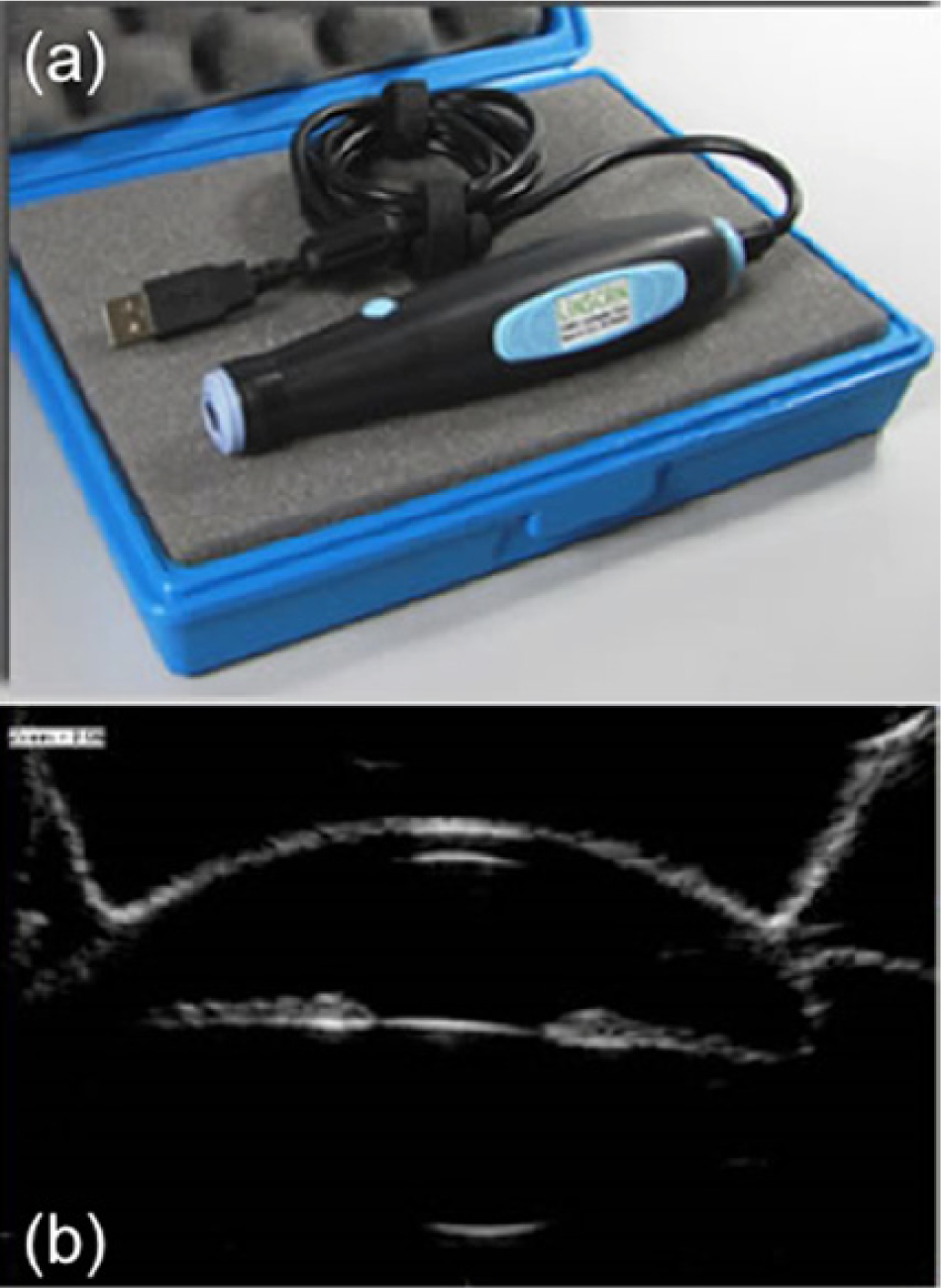
(a) An ophthalmic ultrasound probe operating at a 24-MHz frequency with a USB port interface. (b) An image using that probe of the anterior compartment of the eye. From http://www.ocuscience.us/id78.html
Clinical Applications
The primary use for a handheld smartphone-based ultrasound system is the wide variety of point-of-care (POC) applications: office or bedside examinations in primary care, emergency care, critical care, obstetrics, and ultrasound-guided procedures. It has not been the intent of the developers of these systems to provide comprehensive diagnostic sonographic studies but to quickly answer a specific clinical question. For example, in the emergency care setting, a FAST examination (focused assessment with sonography for trauma, evaluating the perihepatic space or Morison’s pouch, the perisplenic space, the pericardium, and the pelvis) or the extended FAST examination (eFAST, which includes an evaluation for pneumothorax) can be carried out quickly with such a handheld device with very good sensitivity and specificity.8–10
An additional area of application for such devices would be extremely remote areas such as rural regions of developing countries or military battlefields where accessibility, including access to electricity, may be a significant issue. A battery-powered, rechargeable handheld device would provide rapid sonographic imaging to many more potential patients than could be done using conventional high-end ultrasound systems.
A smartphone-based ultrasound system has the potential to become the stethoscope of the future if appropriate training of medical students and residents not in formal radiology programs can be implemented.11,12 A number of medical schools—such as the University of South Carolina; the University of California, Irvine; Harvard Medical School; and the Icahn School of Medicine at Mt Sinai—have introduced ultrasound training early in their programs. Emergency medicine residency programs now are required to include basic training in abdominal, cardiac, and obstetric ultrasound as well as ultrasound guidance of procedures. Studies have shown the enhanced diagnostic capabilities of medical students when they use a POC ultrasound device compared with the physical examination.11,13 Despite these advancements it is likely to take a full generation for the medical community as a whole to incorporate this technology throughout physician training and practice.
There are advantages as well as limitations associated with this emerging technology. The advantages of its compact size and thus its inherent mobility allow sonographic studies to be performed in virtually any setting no matter how remote or cramped for space. By linking the probe to a smartphone device, it takes advantage of the ubiquitous nature of such devices. There are other compact handheld ultrasound systems available, but these are not physically linked to a smartphone. Systems such as the VScan (GE Healthcare Ultrasound, Milwaukee, Wisconsin), the Acuson P10 (Siemens Healthcare Ultrasound, Malvern, Pennsylvania), or the Signos (Signostics, Adelaide, Australia) have the probe hard-wired to a dedicated image viewing system and at present do not offer plug-in capabilities. Using a USB port to connect the probe to the smartphone allows some degree of future flexibility for probe selection and the potential for expanding the areas of application to all systems of the body. (Of note, however, the manufacturer of the current FDA-approved device [MobiSante, Redmond, WA] sells the probe, with two different frequency ranges available [3.5–5 MHz and 7.5–12 MHz], and a specific smartphone with USB capabilities as a coupled unit, so the potential for fully expanded applications remains in the future.) When smartphone manufacturers in the United States fully implement USB features on their devices, this will open up a vast network of possible users and will be a factor in driving the price down. The present system is able to take advantage of smartphones’ cellular and Wi-Fi capabilities to transmit stored images to other sites and/or a picture archiving and communication system, creating the possibility of not only imaging in remote regions but remote interpretation as well.
There are drawbacks and limitations to this new technology. The cost of a system is in the range of $5000 to $10,000, which is too high to be able to place them in all the areas of need. Most smartphones in the United States are not set up with USB 2.0 support, which significantly limits widespread applicability of the technology. As with all of sonography, the results of an examination depend not only on the technology but also on the skill level of the operator. A great deal of research and work remains to be done to determine the necessary amount of education and training required to make the technology useful at the level of the stethoscope. 14 A significant potential drawback to the technology is once most smartphones have the capability to add an ultrasound probe at a low cost, the technology will be available to a wide lay audience with no training whatsoever. It does not take much imagination to see that abuse of this development would drive the public image of ultrasound from one of diagnostic medicine to a means of producing unique entertainment images and video.
Overall, the possible impact of this technology is significant. Mobile, POC sonography is likely to change the way medicine is practiced in many areas and certainly will affect the role of the sonographer. The future remains uncertain whether sonographers will be called on more and more to do focused, rapid screening types of examinations rather than full diagnostic examinations. The advantage of using very small compact systems is the likelihood of decreasing the risk of developing musculoskeletal problems related to poor ergonomics and large high-end ultrasound systems. Will trained sonographers become more of a teacher to groups needing to develop the scanning skills needed for POC sonography rather than acquiring the images themselves? Who ultimately will interpret the images acquired? Ideally, and the potential strength of POC sonography, is for interpretation to be done at the time of image acquisition, but will POC users be adequately trained for this role? These questions, the ethical questions of placing sonography in the hands of untrained laypersons, and others remain to be answered. It is certain that this technology and the trend to “miniaturization” will continue; what is uncertain is how the technology will be integrated into medicine and good patient care.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.