
Abstract
The current assessment of HbA1c levels of diabetic patients is performed only by trained personnel at the laboratory prior to their clinical review consultation. Patients are not empowered to do self-testing of HbA1c at the clinic. This study shows that diabetic patients can perform self-testing of HbA1c and would choose this option over conventional methods, if available. A self-service HbA1c facility that provides patients the option to bypass the laboratory before consultation in all outpatient settings will enable patient empowerment, reduce waiting time and improve their patient experience, while increasing the capacity of laboratory services.Summary box
What is known?
What is new?
What is the impact?
Introduction
Glycated hemoglobin (HbA1c) level is the gold-standard test for monitoring glycemic control and is performed for the management of diabetic patients. HbA1c test ranks as the most-ordered laboratory test in primary care clinics, accounting for 17% of total laboratory service. Globally, the prevalence of diabetes is projected to rise by approximately 20% by 2030. 1 In Singapore, 6.9% of residents are diagnosed with diabetes, and the incidence is projected to increase by 26.1%.2,3 More resources are needed for the management of diabetic patients ascribed to initiatives such as “beyond hospital to community”; allowing patients with cross-institution laboratory orders to access phlebotomy services in primary care clinics, and the launch of “Healthier-SG” advocating preventive health.4,5
Increasing the capacity of laboratory services in primary care clinic becomes important to ensure a smooth patients’ journey for timely follow up and treatment for diabetes. The current assessment of HbA1c levels of diabetes mellitus (DM) patients is done through a bench top analyzer in the primary care laboratory prior to their clinical review consultation. This process requires Medical Laboratory Technologists (MLTs) on-site to render the HbA1c test. With limited headcount for MLTs and difficulty in recruiting and retaining candidates, exploring alternative solutions would be required to complement existing model of service over the long term.
HbA1c test has been evolving over the past decade, from laboratory to point-of-care and home testing. A study in Africa concluded that home-use point-of-care HbA1c testing is feasible for use in community setting with slight underestimation of A1c results. 6 Despite the accuracy of home-use HbA1c test, to the best of our knowledge, there are lack of studies on cost evaluation. It is postulated that home testing HbA1c would not be cost-efficient and convenient as it is tested at intervals of 2 to 3 months. 7 Additionally, it relies heavily on the self-management ability of the patient in ensuring proper storage conditions of test cartridges and keeping track of expiry dates.
In recent years, there has been an increasing trend of self-service technology (SST) adoption. Self-service kiosks are already implemented in primary care for patients to register their clinic visits, make payment for services consumed and book future or same-day appointments for clinic services such as consultations. However, there are currently no self-service HbA1c facilities in primary care clinics. A self-service HbA1c testing kiosk that provides diabetic patients with the option to bypass the need to secure a suitable laboratory test appointment slot before their review consultation is a solution that will potentially reduce waiting time and improve patient experience, while increasing the capacity of laboratory services. In the United States of America, it was found that reduced waiting time for HbA1c appointment had the potential to lower patients’ HbA1c level. 8 With the expected increase in demand for HbA1c testing services, the availability of a self-service HbA1c testing kiosk would resolve issues such as limited appointment slots and facilitate better management and care for diabetic patients.
However, to date, there are limited studies exploring the idea of self-testing point-of-care HbA1c in primary care setting. Hence, this pilot study aims to assess patients’ acceptability and ability to perform self-testing of HbA1c levels within the clinic before consultation, as well as the feasibility of the implementation of self-testing by patients in our primary healthcare setting. The results obtained would provide guidance on the implementation of self-testing HbA1c in primary care clinics and help to manage the projected increase in phlebotomy services.
Methods
Study population
This study was conducted in SingHealth Polyclinics, Tampines in February 2022 and patients were eligible if they were aged 21 years old and above, could converse in English language and had been given a lab order form for a single HbA1c test to be performed prior to their consultation.
Sample size
Based on a study by Browne, 9 a minimum of 30 subjects is required to estimate the feasibility and acceptance of a pilot study. A total of 30 participants were recruited for this study.
Patient and public involvement
Self-service HbA1c test station set-up and procedure
A set of Hemocue® HbA1c 501 Analyzer was commissioned and placed near the laboratory. The Hemocue® HbA1c 501 is a point-of-care system that provides a fully automated boronate affinity assay for determination of the Hemoglobin A1c percentage (HbA1c%) in whole blood. The Hemocue® HbA1c 501 Analyzer is certified according to the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) and the National Glycohemoglobin Standardization Program (NGSP) to ensure quality of the HbA1c test. It is a small, portable, and fully automated point-of-care system for all healthcare environment. Its test cartridge pack consists of a cartridge and a reagent pack containing the reagents necessary for the determination of hemoglobin A1c, with a sampling area for blood collection. Each test requires a minimum of 4 μL of capillary blood sample and HbA1c result will be displayed 5 min after the test is started.
Test cartridges, disposable lancets, alcohol swabs and plasters were provided at the test station. A demonstration video providing step-by-step instructions to guide patients through the entire test process was stored in a tablet device and placed next to the analyzer. Participant could watch the video and pause it at their own convenience while performing the test. A plaster bandage was provided to participants to stop the bleeding after needle-prick. All used test cartridges, lancets, alcohol swabs were disposed of in the biohazard bin located at the test station. A study team member familiar with the test procedure was on-site to troubleshoot, if required.
Participants proceeded to complete a questionnaire while awaiting the HbA1c results. The questionnaire consists of the System Usability Scale (SUS) and a self-designed section which measured participants’ acceptance, difficulty and understanding on the self-testing procedure and video demonstration. The printout of the HbA1c result was tagged to the patient consent form for verification of results with the test performed in the laboratory.
System usability scale
The SUS consist of 10 items on a five-point Likert scale that assesses the usability of a system. 10 It allows for fast and efficient results to be generated on the usability of the system. Scores for SUS ranges from 0 to 100, consisting of both positively and negatively phrased questions. In its raw form, each item score ranges from 0 to 4. Scores for positively phrased questions 1, 3, 5, 7 and 9 were calculated by subtracting 1 from the raw score. While negatively phrased question 2, 4, 6, 8 and 10 were calculated by subtracting the raw score from 5. Score contribution for all items were then summed up and multiplied by 2.5 to obtain a final score between 0 and 100. A higher score translates to better system usability. Scores above 68 were considered above average and scores below 68 were classified as below average.
Acceptance, difficulty and understanding for self-testing
Participants were asked to rate the 7-step procedure on a five- or six-point Likert Scale to assess their ability and acceptance on self-testing. The 7 steps are: 1. Opening the test cartridge pack by tearing the pouch on the side with the serrated edge and removing the contents from the pack. 2. Inserting the test cartridge into the compartment and ensure proper placement. 3. Gently mixing the reagent pack back and forth 5 to 6 times. 4. Wiping the finger with an alcohol swab and letting it dry, then performing the finger prick using the disposable lancing device to obtain a good drop of blood. 5. Gently touching the blood sample with the tip of the sampling area of the reagent pack and ensuring the sampling area is filled. 6. Inserting the reagent pack in the cartridge and gently pushing into the cartridge compartment of the analyzer. 7. Removing and discarding the cartridge after the test is completed.
The five-point Likert Scale consists of selection from Strongly Agree to Strongly Disagree, while the six-point Likert Scale had an additional option of Not Applicable (NA). Questions answered include ease of performing each step and ability to understand and follow instructions from the video demonstration. The results obtained were tabulated and analyzed to understand the feasibility of implementing such self-service technology and issues participants encountered. The total time taken and number of replays for each step were also recorded.
Statistical analyses
Descriptive statistics were presented in frequencies and percentages for demographics variables and mean and median for SUS. The SUS score of 68 and above was defined to be above average. Chi-Squared test or Fisher’s Exact test were performed to test association between the demographics and SUS score where appropriate. Questions on acceptance and understanding of the self-testing HbA1c system were presented in frequency and percentages. All analyses were carried out using IBM SPSS Version 26.0. A p-value ≤.05 was considered statistically significant.
Results
Demographics and acceptance level of study population (N = 30).

Contribution of individual items to system usability scale score.

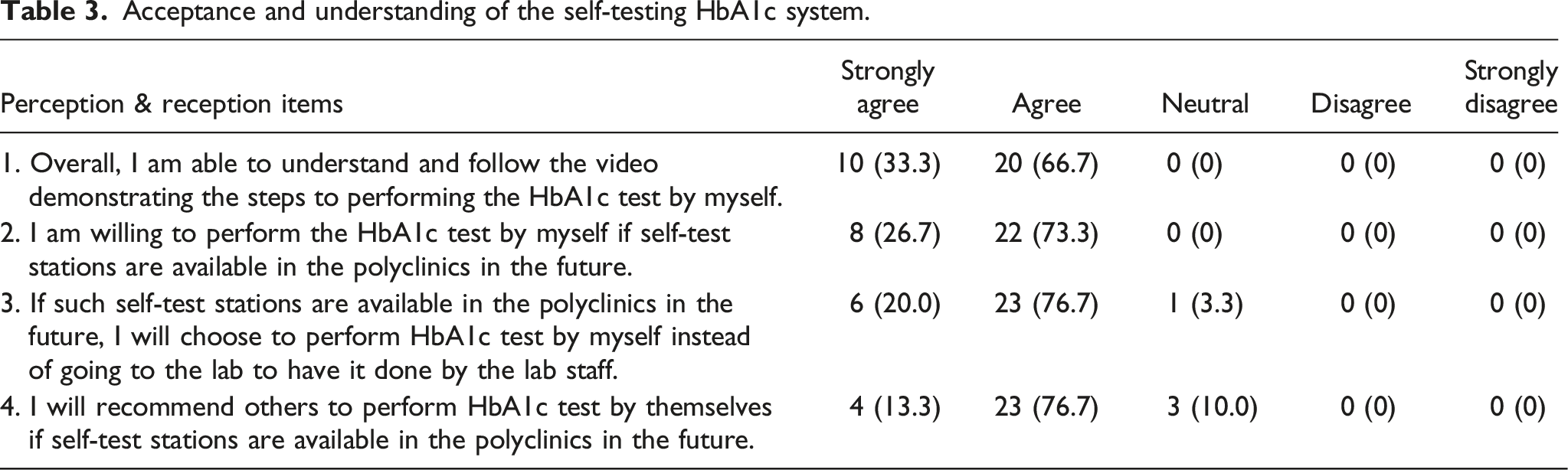
Acceptance and understanding of the self-testing HbA1c system.
User experience on understanding of video and difficulty in performing the entire procedure.

Discussion
This study assessed the acceptability, understanding and feasibility of self-service HbA1c testing for diabetic patients in a primary care setting. In general, 100% of the participants were able to follow, understand the video demonstration and showed willingness to self-test their HbA1c. Although SUS score was marginally below average, participants were confident and had positive reception towards using the system frequently. However, majority of the participants required assistance in one of the steps where some degree of force was needed to insert the test cartridge into the analyzer.
This study has shown that diabetic patients are able to self-test their HbA1c levels without requiring a phlebotomist in primary care setting. All patients were able to follow and understand the video demonstration, with an average completion time of 11.8 min. Considering approximately two third of the study population is aged 60 years and above, it is postulated that the younger diabetic patients would exhibit the capability to perform HbA1c self-testing. However, there is room for improvement to enhance the overall user experience and system usability. Potential avenues for refinement of the video demonstration include incorporating further details such as the recommended angle of insertion and expected force required for insertion and removal of the cartridge into the analyzer. Additionally, it is important to note that the current video demonstration is available solely with English captions and lacks a voice-over component. Consequently, patients are required to focus on both the captions and visual demonstration simultaneously. To enhance accessibility and usability for a wider population, considerations should be given to offer the option of multilingual voice-overs within the video demonstration when implementing self-service HbA1c kiosks. This proactive approach would ensure generalizability of HbA1c self-testing to a more diverse group of diabetic patients.
Acceptance for HbA1c self-testing was high among participants despite some difficulty in inserting the test cartridge into the analyzer. All but one participant will choose to self-test HbA1c in the future instead of opting for the conventional HbA1c testing done by the phlebotomist or MLT. This offers a promising prospect for the integration of self-testing as a viable option for diabetic patients. Notably, the presence of a trained research assistant on-site to provide guidance and support may have provided a sense of assurance to the study participants that in turn accounted for the heightened level of acceptance. The allocation of a trained personnel on-site will be important for effectively addressing prospective challenges during clinical implementation. It is imperative for the personnel to undergo a structured training program that will equip them with the necessary competencies for the role.
In this proof-of-concept study, the results have indicated that HbA1c self-testing within a primary care setting is feasible, with diabetic participants demonstrating a high level of ability and acceptance. Out of the 60 eligible patients who were approached, 30 (50%) were willing to participate in this study and were recruited. The main reason for non-participation was noted to be the fear of performing needle-prick tests on themselves. To attract diabetic patients from the general clinic to utilize the self-service HbA1c testing kiosk, there is a need for targeted efforts to provide information of the kiosk’s benefits. Such issue could be addressed through the distribution of educational pamphlets (either hardcopy fliers or electronic mailers) before booking of subsequent appointments. A further study might need to be done to analyze the take-up rate for such self-test facilities.
As the concept of around-the-clock primary care clinic pods emerges on the horizon, it might be possible to seamlessly incorporate self-testing HbA1c and potentially other point-of care tests within these pods. The integration not only increases the flexibility of booking for clinic appointment slots but also complements well with the increasing demand for telehealth services. This will provide well-controlled diabetic patients who are managed through video consultation the option to take up the service and ensure that appropriate care is delivered. Furthermore, this service could also be adopted by private General Practitioner (GP) clinics to provide routine HbA1c testing in their management of diabetic patients.
Conclusion
Despite encountering issues in the insertion of test cartridges into the analyzer, diabetic patients had high acceptance level for self-testing of HbA1c and are willing to perform it in future if such a service was available. All of them were able to perform the test themselves based on the instructions provided and willing to recommend this option of measuring glycated hemoglobin to others. This study has proven the possibility of having a self-testing HbA1c facility in our primary healthcare setting to cope with increasing demand for phlebotomy services. With reduced reliance on the MLTs to perform their HbA1c tests, diabetic patients will not face the frustration of not being able to book an appropriate lab appointment slot prior to their regular review medical consultation. There will be a potential increase in laboratory capacity too, when the MLTs are freed up to focus on providing phlebotomy services for other tests.
Moreover, the potential to scale up such health service beyond primary care setting to General Practitioner clinics will enable outreach to a wider population and ensure a more convenient and timely process for diabetic management.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SingHealth Polyclinic Centre Grant – IPRAMHO; NMRC/CGAug16C008.