
Abstract
Intraoperative ultrasonography (IOUS) is rapidly changing as advancements in technology provide surgeons with more options for the treatment of their patients. Despite the introduction of intraoperative magnetic resonance imaging (MRI) and computed tomography (CT), advancements in IOUS technology and its low cost have kept this a viable modality. The improved image resolution that is available provides neurosurgeons, for example, with the information necessary to adequately resect cancer in the brain, including superficial and deep-set tumors, whether they are primary brain cancers or brain metastases. Strain sonography and contrast-enhanced ultrasonography (CEUS) are advancements being used to help better visualize residual tumor cells after resection. IOUS is the only modality that provides the neurosurgeon with the ability to obtain real-time imaging while a resection is taking place. All of this information helps to make the complete resection of brain cancer with the least amount of neurological damage more likely, significantly enhancing the patient’s chances of a good outcome.
Intraoperative ultrasonography (IOUS) has seen a significant increase in usage because of technologic advancements made to transducers and sonographic machines. These advancements have improved the image quality, allowing for better visualization of organs and pathology. The result of better visualization, combined with real-time imaging, has opened the door to numerous applications of sonography in the operating room that were not possible with previous sonographic systems. The continued improvements in speed of data collection and miniaturization will undoubtedly lead to even more widespread applications. 1 IOUS is being used for procedures such as pancreatic imaging for bile duct obstruction and tumor localization, vascular procedures including endarterectomy and a variety of endovascular interventions, laparoscopy procedures, guidance for intraoperative biopsies, guidance for shunt placements, spinal lesion removal, and resection of brain cancers. The focus of this article is on the applications of IOUS in neurosurgery, specifically surgery of the brain.
Even with the expanding capabilities of IOUS for the guidance in neurosurgery, the technique still is not used to its full potential. One of the reasons for this is that neurosurgeons are more comfortable interpreting magnetic resonance imaging (MRI) and computed tomography (CT) images compared with sonographic imaging. However, considering that intraoperative MRI and CT are not available in all facilities due to costs and other physical constraints, neurosurgeons are likely to become more open to the possibilities that IOUS holds in the resection of brain tumors. These patients often have a very poor or limited prognosis, and the potential exists to provide the patient with an enhanced likelihood of improving their quality of life postoperatively.
History
IOUS has been applied since the first sonographic machines were in use. Although IOUS began to be developed in earnest after the development of gray-scale B-mode ultrasonography, and especially after the development of real-time imaging, early investigators were using more primitive tools as early as the 1960s. 1 One of the very first reports of IOUS was by Schlegel et al 2 in 1961, who used A-mode ultrasonography for the localization of renal calculi (Figure 1).
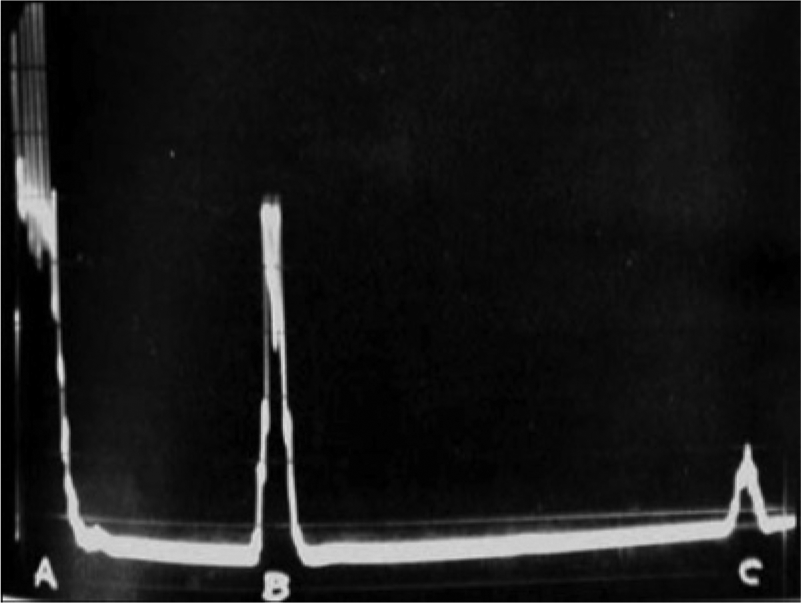
A-mode sonogram of a renal calculus. The initial spike labeled A represents the surface of the kidney, the spike labeled B is a reflection from the calculus, and the small spike labeled C is the posterior margin of the kidney. (Reproduced with permission from Schlegel JU, Diggdon P, Cuellar J. The use of ultrasound for localizing renal calculi. J Urol 1961;86:367–369.)
Additional early A-mode applications included the detection of stones in the bile duct and in the gallbladder. A-mode sonography, however, simply plots points on the screen that chart the depth of the source of the returning echo, providing very limited information to the surgeon. The inability to display tissue texture in A-mode or bistable B-scanning as well as the rather large, bulky size of the equipment limited the more widespread use of IOUS. A small direct-contact ophthalmic B-scanner was developed and proved useful for B-scan ultrasonography during orbital surgery for tumors, as reported by Purnell et al 3 in 1973 (Figure 2), but very little further development was reported until the advent of real-time scanners and smaller, more portable equipment.
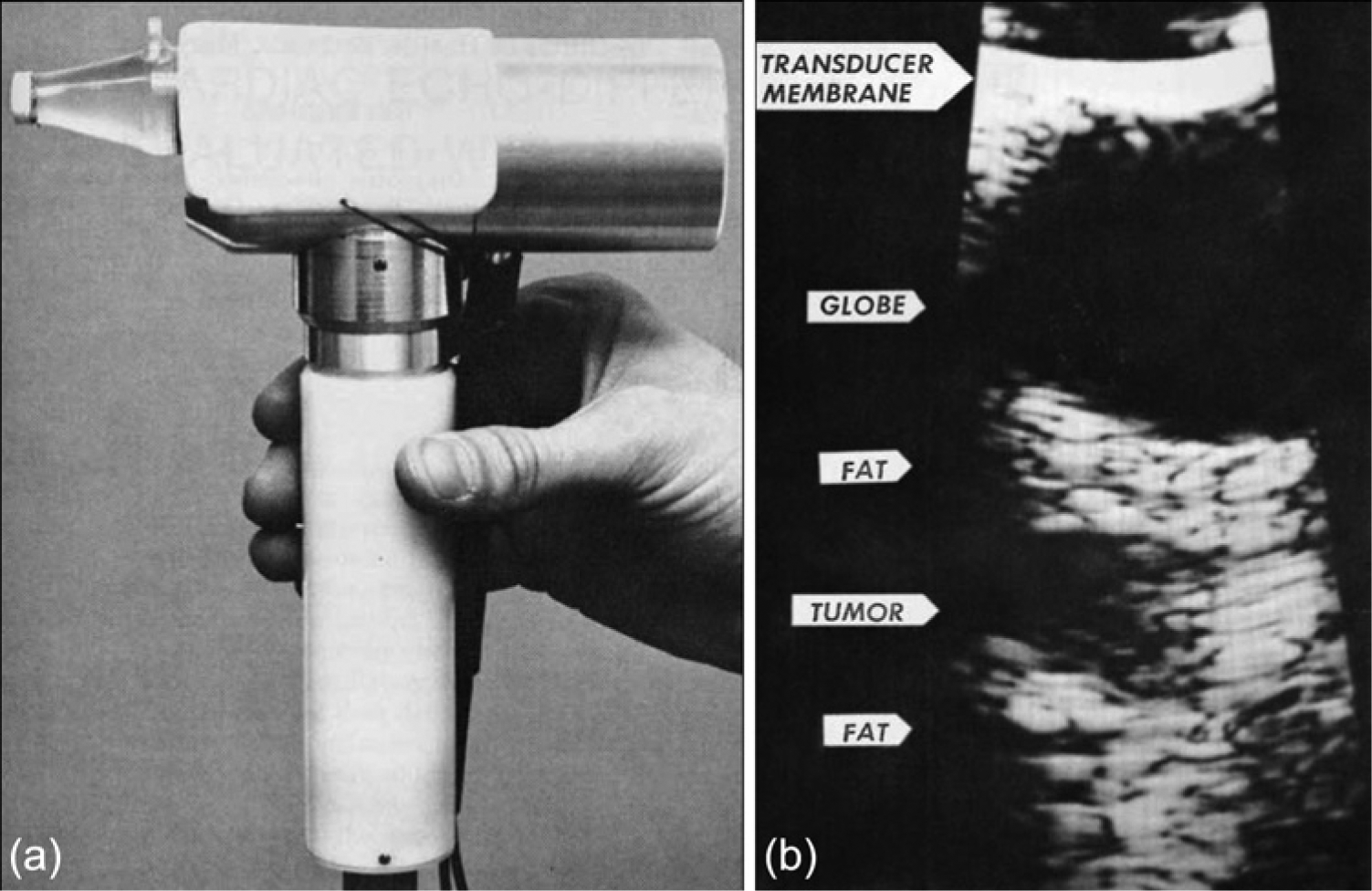
(a) Early contact B-scanner for intraoperative ophthalmic use. (b) Intraoperative B-scan image of a retrobulbar tumor. (Reproduced with permission from Purnell EW, Cappaert WE, Sokollu A: B-scan ultrasonography during orbital surgery. J Clin Ultrasound 1973;1:32–35.)
The development of real-time gray-scale imaging opened up many more opportunities to apply IOUS. This provided the capability to see borders of organs and distinctly outline pathology, and it provided the advantage of real-time sonographic guidance for the placement of biopsy needles (Figure 3). In addition to real-time imaging, the transducers used for IOUS were becoming smaller and more appropriate for the operating room. The combinations of these two facts led to the development of the Berger biopsy guidance system, an ultrasonographically guided stereotactic device that could be used through a minimal craniotomy site just slightly larger than a standard burr hole (Figure 4). 4 This device allowed brain biopsies to be performed with minimal morbidity to these patients.

Intraoperative sonogram of the liver localizing a small intrahepatic abscess with an ultrasonographically guided needle placed into the abscess cavity for subsequent surgical drainage. The needle tip can be seen indicated by the marker. (Reproduced with permission from Kane R: Intraoperative ultrasonography history, current state of the art, and future directions. J Ultrasound Med 2004;23(11):1407–1420.)
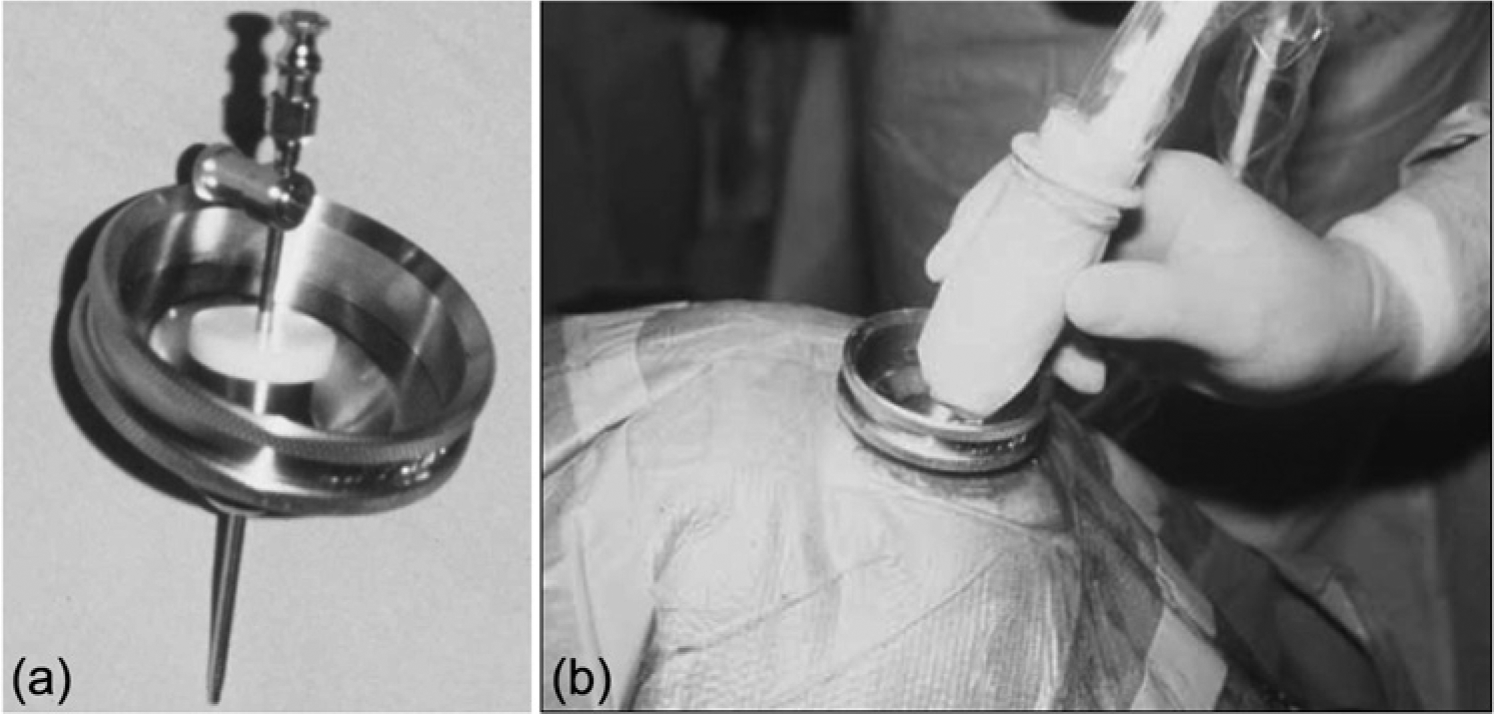
(a) Photograph of the Berger ultrasonographically guided stereotactic device. (b) The Berger device in use in the operating room with the transducer shown in the pivot zone of the device. (Reproduced with permission from Kane R: Intraoperative ultrasonography history, current state of the art, and future directions. J Ultrasound Med 2004;23(11):1407–1420.)
Even with the advancements in technology, IOUS still struggled to gain acceptance among surgeons in the 1980s. However, by the mid-1990s, many surgeons recognized the value of IOUS during surgical procedures. With the availability of various types of IOUS and laparoscopic ultrasound probes, the use of ultrasound has become more widespread during a variety of operations. 5 The many areas that now use IOUS include neurosurgery, endocrine surgery, cardiovascular surgery, hepatobiliary surgery, pancreatic surgery, and other abdominal surgery.
Instrumentation
The current standard for instrumentation in IOUS today is the use of B-mode sonography. Color or power Doppler imaging frequently complements B-mode imaging to distinguish blood vessels from other structures or to identify small vessels; however, most IOUS examinations can be performed with B-mode ultrasound alone. 5 One of the benefits of IOUS is that it usually requires sound penetration significantly less than 10 cm, because there is less distance for the sound waves to travel before they reach their destination. This means a higher frequency transducer can be used to obtain greater resolution images. For neurosurgical procedures, a craniotomy/craniectomy removes the bony skull from the ultrasound pathway, leaving only brain tissue itself, with its low attenuation, in the acoustic path. During pancreatic surgery, the abdominal wall is incised and pulled back, allowing the opportunity for the transducer to be placed directly on top of the pancreas. Typical IOUS frequencies vary from 7.5 to 10 MHz, but higher frequencies up to 15 MHz are available for use in circumstances where depth of penetration is not a limiting factor. 6 With such high frequencies, even small lesions, such as 1-mm calculi, 2-mm cysts, 1- to 2-mm vascular defects, and 3- to 5-mm tumors, can be readily detected. 5
The types of transducers used for IOUS include those characteristically used for general sonography such as linear array, curvilinear array (convex), and phased array (sector). In addition, transducers have been designed specifically for use in IOUS with certain sizes and shapes conducive to surgical application. Direct exposure in the operative field is often very small, making it essential for the probe to be small enough to be manipulated in this confined space. The two principal shapes of probes used are a flat T- or I-shaped probe and a cylindrical pencil-like probe, with the active elements oriented to allow end viewing or side viewing (Figure 5). 6
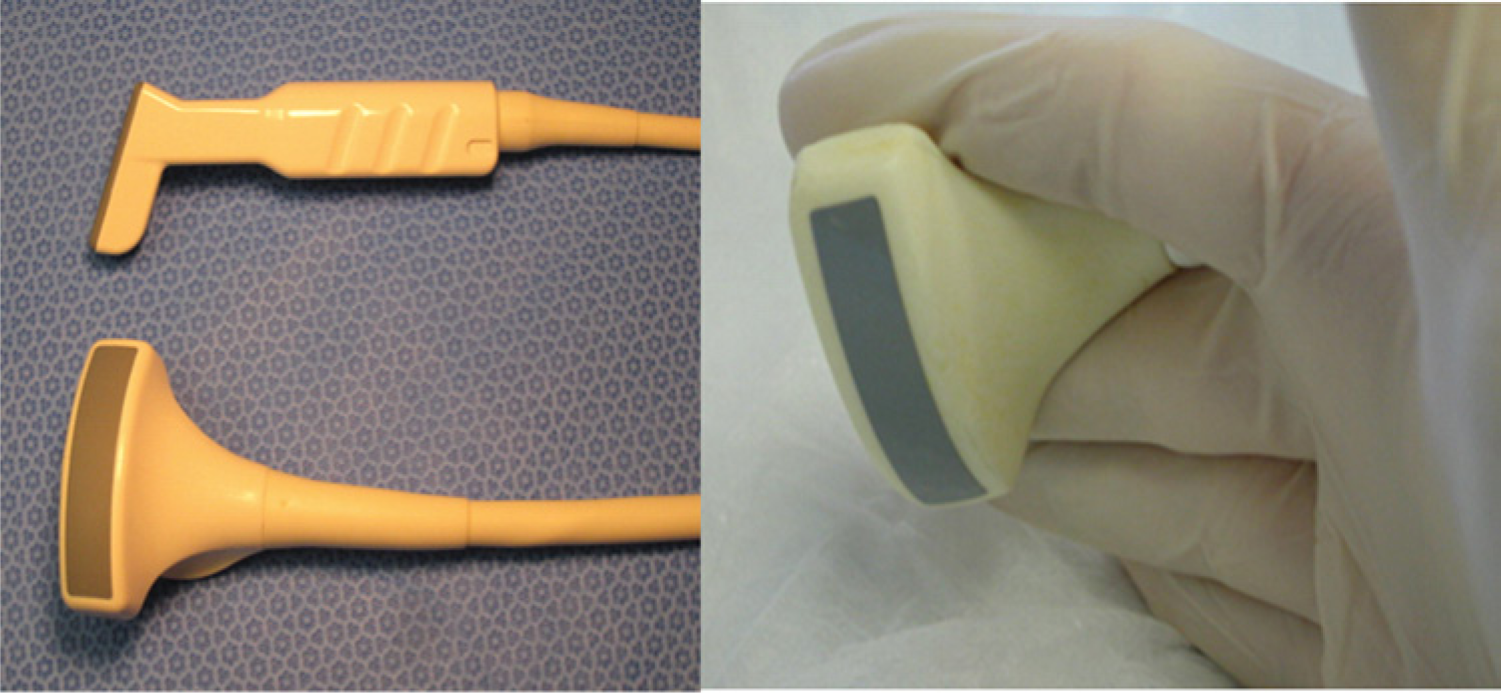
Examples of transducers designed specifically for intraoperative use. (a) A small footprint “hockey stick” probe designed for end viewing and a linear array with the active elements positioned for side viewing. (b) Configuration of many of these transducers allows their insertion into small, confined anatomic spaces, and they can be cradled in the palm of the operator’s hand or between the operator’s fingers. (Reproduced with permission from Sun MRM, Brennan DD, Kruskal JB, Kane RA: Intraoperative ultrasonography of the pancreas. Radiographics 2010;30:1935–1953.)
A flat probe designed for IOUS usually has a wider footprint of 3 to 5 cm and is able to provide a wide near-field image, making it more useful for imaging larger organs. 5 A cylindrical, pencil-shaped probe is useful for scanning small target organs or structures, such as the extrahepatic bile ducts, that may be located deep in the operative field. General transducers used in everyday scanning can also be used in surgery when exposure in the operative field permits. A general-purpose 3- to 5-MHz transducer may be used in the operating room for a variety of procedures when a wide field of view would be advantageous, such as sonographic guidance during a dilation and curettage (D&C) procedure or localization of the kidney for stent placement in a pregnant woman in whom the use of radiation is contraindicated. An endocavitary prostate probe can be used with a needle guide for the performance of prostate biopsies in the operating room.
Regardless of the type of transducer used for IOUS, it will be part of the sterile operative field and therefore must be either covered with a sterile probe cover or cold-gas sterilized. The gas sterilization procedure requires aeration, limiting use of a probe treated in this fashion to one procedure a day. In addition, some manufacturers are reluctant to allow gas sterilization of transducers because of the risk of damage caused by the high temperatures required during the sterilization process. 6 General transducers used in everyday scanning must be covered with a sterile probe cover, because they are not designed to withstand gas sterilization without risk of damage to the transducer. During scanning, caution must be taken to avoid tearing the transducer sheath, contaminating the surgical field. Recently, a low-temperature hydrogen peroxide vapor-gas plasma sterilization, which is completed in 60 minutes, has become available, and some IOUS probes are amenable to this method. 5 Glutaraldehyde also may be used to sterilize transducers for which gas plasma sterilization is not recommended; however, glutaraldehyde must be used with caution because adverse reactions have been reported. 6
Universal precautions must be adhered to in the removal of any sterile probe cover, because the probe cover has come in direct contact with the bodily fluids of the patient. Even if a transducer has been covered with a sterile probe cover, it still must be disinfected after each use. This should be accomplished following the manufacturer’s directions appropriate to that specific probe, using the recommended disinfectant just as is applied in the sonography department to disinfectant transducers after each use.
Applications in Neurosurgery
Intraoperative MRI and CT are still the gold standard for the surgical planning and resection of brain tumors; however, they are very costly, require significant investment in supporting infrastructure, and are not available at all health facilities. Preoperatively, they can provide excellent, detailed anatomic maps to plan surgery. Once surgery is under way, there may be some slight shifting of the brain tissue, rendering the preoperative anatomic landmarks misleading and of no use. IOUS provides high-resolution, real-time images that can be used to identify preoperative landmarks and guide surgeons during the procedure even in the event of tissue shifting. This is particularly helpful after the initial resection of tumor when there likely has been significant displacement of tissue from its preoperative location; real-time imaging provides anatomic localization after the brain has shifted to help identify any residual tumor.
A potential limitation of IOUS is the necessity that the operator has the proper knowledge to set up the equipment and interpret the images. Neurosurgeons have noted that sonograms can be difficult to interpret, and the inability to demonstrate precise spatial localization can be confusing during surgery. 7 This can be attributed in part to the surgeons’ lack of adequate training in the use and interpretation of sonography, and often to the use of sonography equipment consigned to the operating room that is older and not able to take advantage of newer technology. Neurosurgeons would have to acquire this type of additional training to be able to get the most benefit out of using IOUS. The alternative is to call a radiologist to the operating room to help with the interpretation of IOUS images, but many hospitals do not have adequate staffing to allow for this practice. Proper procedure in performing IOUS is important in maintaining image quality and obtaining the high-resolution images in orthogonal imaging planes necessary to solve this problem. 7 With proper training, the acquisition of high-quality, real-time sonography images allows neurosurgeons to resect not only superficial tumors but small deep-seated tumors as well.
Brain metastases are more common than primary brain cancer, and there is debate over the best treatment protocol. 8 IOUS provides a means to help neurosurgeons more safely remove these metastatic lesions. Complete removal requires the capability to visualize all of the tumor borders and any residual cells during the surgery. IOUS has shown the ability to identify lesion borders, anatomical relationships, and residual tumor cells with high sensitivity, leading to a more complete and safe tumor removal. 7 Intraoperative MRI may also be used to provide high-quality images; however, it is very expensive and unavailable in many hospitals. Lower cost, more practical utility, the ability to repeat the examination several times, and faster image acquisition are some of the characteristics that make IOUS a more attractive method. IOUS allows the localization of lesions in less than one minute and can indicate where best to open the dura mater, the direction and relationships of each sulcus with the tumor, the optimal point to perform the corticectomy, and the best route to approach the tumor. The use of color or power Doppler can help further to identify important vascular structures.
Primary brain cancer is not as common as brain metastases, but lesions such as glioblastomas and low-grade gliomas are very aggressive tumors. The best opportunity to increase survival for the patient is the complete removal of the primary tumor and all branching tentacles associated with this tumor. Optimal results may be obtained when maximal surgical resection is achieved with minimal disturbance of neurological function. 7 To achieve this goal, accurate and precise delineation of the tumor and its margins is required. Preoperatively, this is effectively accomplished using MRI or CT. IOUS provides this same type of information in the operating room for a more complete, effective tumor resection.
One of the new technologies being implemented to help guide the resection of brain tumors is strain sonography.9,10 Neurosurgeons often palpate the brain to feel for the stiffer tissue consistency of brain tumors relative to the surrounding normal brain tissue, allowing palpation of residual tumor that may not be visualized using the operating microscope. Tissue strain can be thought of as the amount of tissue displacement when a pressure force is applied. Strain sonography imaging allows a noninvasive method to assess tissue hardness (stiffness) in the brain. With a uniform stress applied to the brain tissue, the displayed strain values will be proportional to the modulus of elasticity (Young’s modulus, the inverse of stiffness) of the tissues; the stiffer the tissue, the less the strain or displacement. The ultrasound strain magnitude images possess a higher contrast between tumor and normal brain tissue, particularly in the peripheral parts of the tumor, than the conventional B-mode images (Figure 6). 10
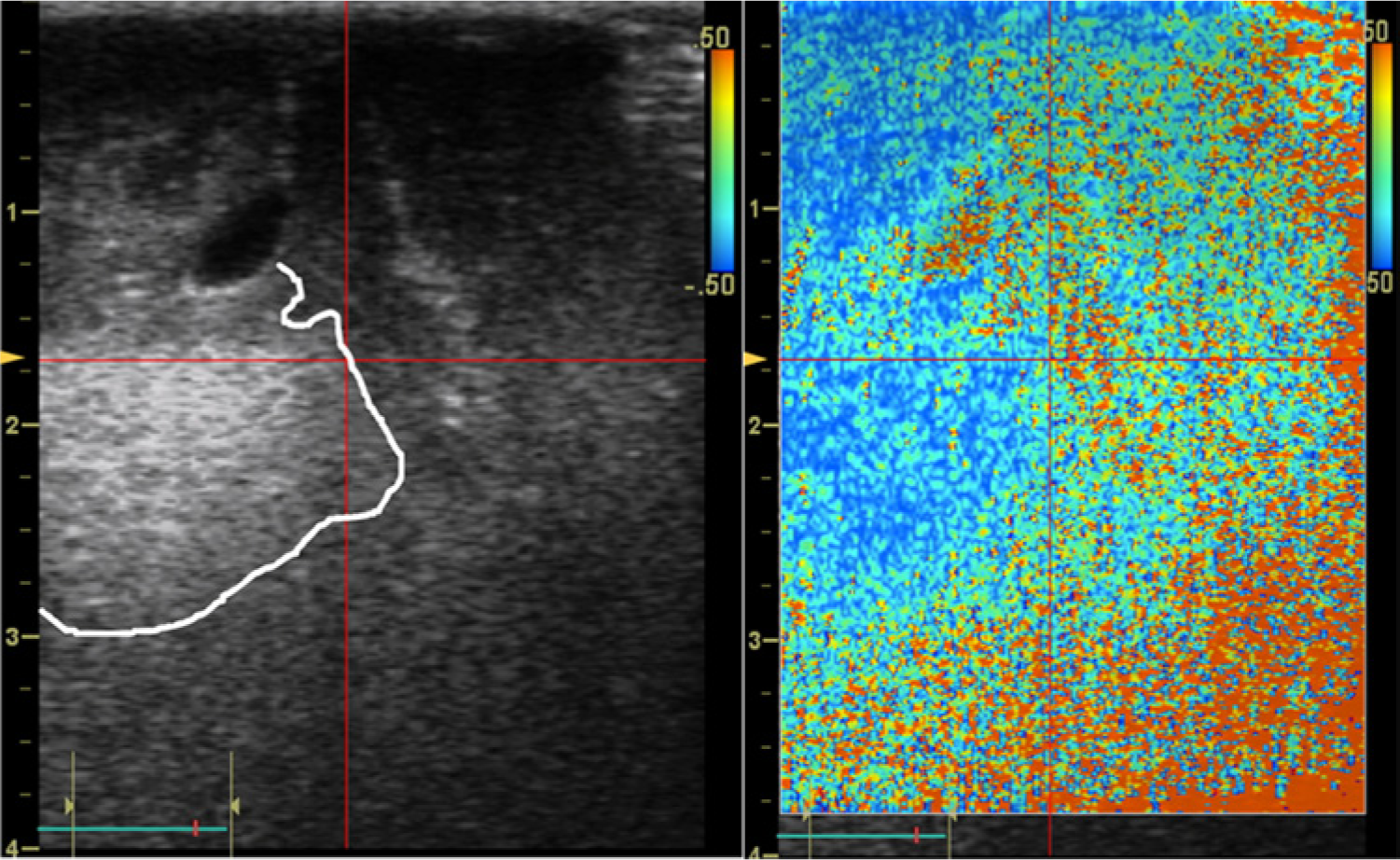
Side-by-side images of a glioblastoma (grade IV) showing the traditional B-mode gray-scale image on the left and the corresponding strain magnitude image on the right. (The delineation of the solid tumor close to the location of the measurements has been marked with a bright line in the B-mode image.) (Reproduced with permission from Selbekk T, Brekken R, Solheim O, Lydersen S, Hernes TA, Unsgaard G: Tissue motion and strain in the human brain assessed by intraoperative ultrasound in glioma patients. Ultrasound Med Biol 2010;36(1):2–10.)
A current limitation of strain imaging is the presence of noise in the image; to overcome this, strain imaging should be used in conjunction with conventional B-mode sonography. Such image noise is typically seen in regions in the B-mode image that appear hypoechoic compared with other brain tissue, for example, when imaging homogeneous tissue like the brain stem and deeper white brain matter. Strain sonography also remains very operator dependent in applying uniform stress, and it is not difficult to obtain false-positive or false-negative images with strain sonography without a skilled operator. Even with the learning curve required for the implementation of this modality, however, strain sonography holds the possibility of providing neurosurgeons with another technique for more complete resection of brain tumors. Strain imaging may be of particular value compared with conventional sonography alone in the detection of any residual tumor after initial resection. 10
A second new technology available for IOUS is the use contrast-enhanced ultrasound (CEUS). After a baseline IOUS scan, the ultrasound contrast media can be injected into a cubital vein. After allowing 30 to 60 seconds for the contrast media to circulate freely in the blood pool, the region of the tumor is scanned with B-mode and color Doppler imaging for two to five minutes to observe the enhancement of the tumor. 11 Comparisons can then be made of the image that was acquired before injection of the contrast media and the images obtained after the injection of the contrast media.
The increased echogenicity provided by the contrast allows identification of the borders of vascularized tumors and also helps distinguish residual tumor from other surrounding tissues (Figure 7). Complete resection can then be done while minimizing the significant risk of damage to healthy brain tissue and associated postoperative deficits. In the United States, this use of CEUS is not approved by the Food and Drug Administration (FDA), but the contrast media are widely available in health facilities that perform echocardiography (for which ultrasound contrast is FDA approved), and it can be used off-label by following appropriate guidelines for such use.
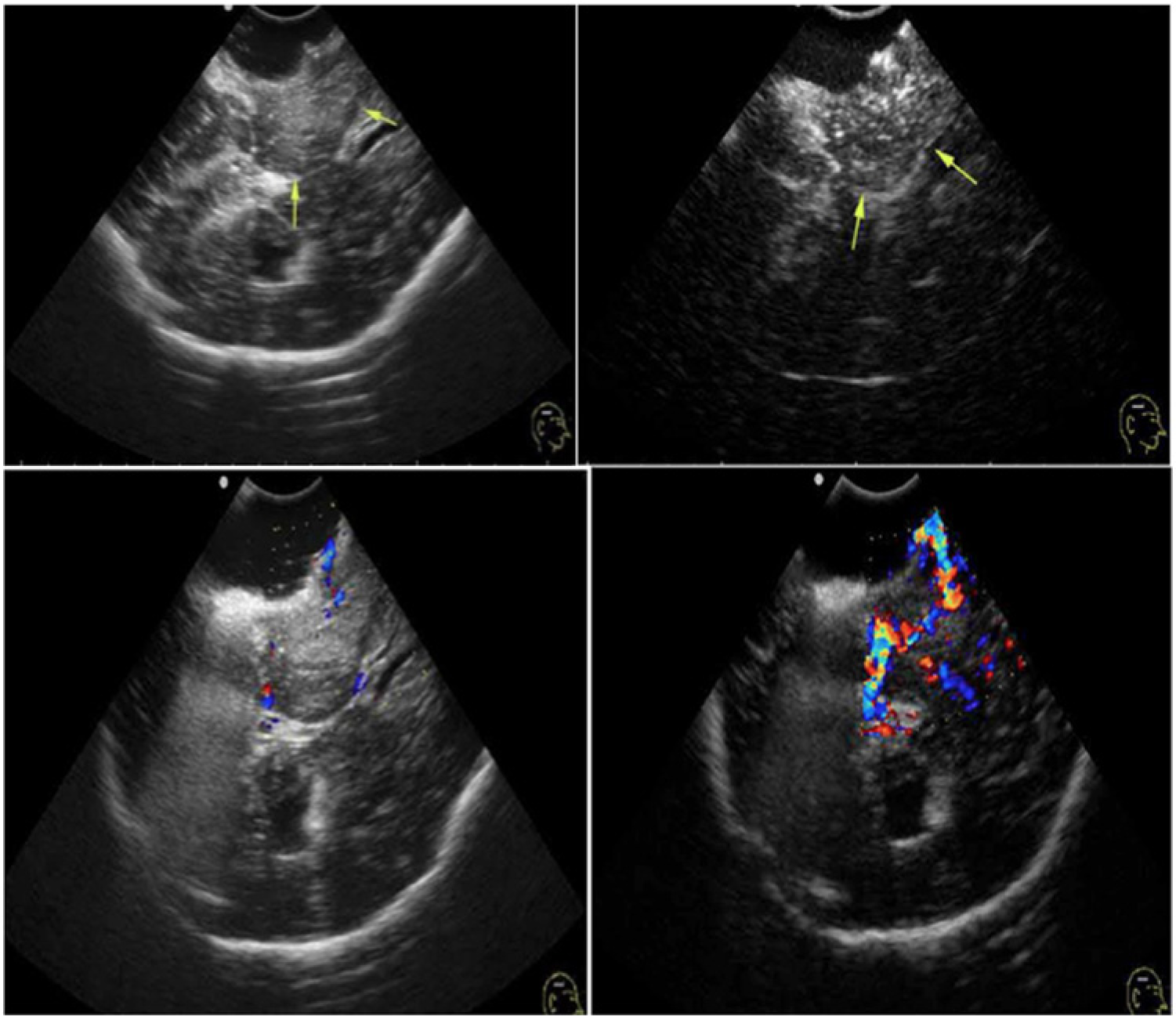
Residual tumor tissue was not identified on conventional gray-scale image (top left) but was visualized on a contrast-enhanced ultrasonographic (CEUS) image (top right). Residual tumor tissue had minimal vascularity on conventional color Doppler imaging (bottom left) but showed hypervascularity on CEUS color Doppler imaging (bottom right). (Reproduced with permission from He W, Jiang X, Wang S, et al: Intraoperative contrast-enhanced ultrasound for brain tumors. Clin Imaging 2008;32(6):419–424.)
IOUS also has been used recently in conjunction with awake anesthesia and intraoperative direct electrical stimulation in the removal of brain tumors located in or adjacent to particularly sensitive regions of the brain. 11 Such regions, for example, are those in control of motor, sense, language, memory, and other cognitive functions. Without detailed intraoperative guidance, surgery for cerebral tumors in these regions frequently results in a poor extent of resection, permanent postoperative deficits, or both and remains a difficult problem. After preoperative mapping of the brain tumor with MRI, IOUS provides guidance for the neurosurgeon in the dissection of the brain tumor. Under awake anesthesia, the patient receives direct electrical stimulation while asleep to monitor any changes in the responses of the area of the tumor. Rapid anesthesia reversal is also possible in order to wake up the patient enough to monitor cognitive function in the area of operation, without causing the patient pain. Even with brain shifting, as discussed above, IOUS is able to provide the anatomic information necessary to carry out a complete resection with no or minimal residual tumor and without damage to surrounding normal brain tissue.
The most significant limitation to IOUS is, as with all sonography, that the information obtained with this modality is very operator dependent. The neurosurgeon must be comfortable with interpreting sonographic images and knowledgeable on how to obtain the best image possible, particularly in those institutions where staffing conditions may not allow a radiologist or a credentialed sonographer to be a part of the operative team. A second limitation in some cases is the difficulty in precisely judging the presence and extent of any residual tumor after resection of the primary mass, because the surgical cavity may now contain microbubbles in the sterile water used for acoustic coupling, edema at the resection margins, or hemostatic material applied during the resection. All of these may cause strong echoes, which may obscure the important information regarding residual tumor. 12 Despite the training and experience required to obtain diagnostic images and these limitations of IOUS, it remains a viable option for neurosurgeons in the resection of brain tumors located in or adjacent to the sensitive areas of the brain.
Conclusion
The advancements in sonographic machine and transducer technology have expanded the potential applications of sonography in the operating room. New technology allows surgeons to obtain more precise, detailed images in real time of organs and pathology than was available prior to these advancements. The primary limitation of IOUS is that the acquisition of high-quality images is very operator dependent. When used appropriately, IOUS has been shown to be an effective tool for the removal of metastatic lesions of the brain as well as primary brain tumors, both deep and superficial, including tumors associated around or in the sensitive areas of the brain. Developing technologies such as strain sonography and contrast-enhanced ultrasonography are also proving useful in the identification of residual disease following resection of the primary mass.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.