
Abstract
Echocardiography has been utilized perioperatively since the 1970s and many studies have been conducted to prove its efficacy. Epicardiac echocardiography (EE) is the modality of choice when transesophageal echocardiography (TEE) is contraindicated or when aortic atherosclerosis is suspected. Perioperative TEE has shown to be an excellent tool in the operating room for assessment, diagnosis, surgical guidance, and outcome evaluation. Pediatric surgery has also shown better surgical outcomes for congenital disease states with the guidance of TEE. The cardiac Sonographer’s role in the operating room is a very important one because it involves operating the ultrasound machine and communicating image interpretations to surgeons in a timely and efficient manner. Cardiac Sonographers eager to progress in their careers can take advantage of this opportunity to enhance their clinical and educational qualifications. Technology is advancing quickly with the breakthrough of 3D and 4D TEE, where images are captured in real time, providing improved diagnoses and prognosis. This article discusses the evolution of echocardiography in the operating room and its future impact on perioperative evaluation, with attention paid to the role of cardiac Sonographers and the future clinical progression in their scope of practice.
Keywords
Introduction
Perioperative echocardiography (POE) has become a reliable tool in guiding surgeons by providing instant diagnostic feedback and immediate assessment of results during cardiac procedures. Whether it is through epicardiac echocardiography (EE) or transesophageal echocardiography (TEE), perioperative echocardiography has shown enormous progress in improving the outcomes of cardiac surgery and ultimately, patient prognosis. Intraoperative echocardiography (IOE) was first introduced in the 1970s when Johnson and coworkers used M-mode echocardiography to evaluate the results of mitral valve operations. 1 IOE evolved further in the 1980s when surgeons began utilizing 2D POE in the operating room to aid in the evaluation of left ventricular function, prosthetic valves, and localization of myxomas and other foreign bodies. 1 Perioperative 2D echo allowed surgeons to examine the left ventricle closely by evaluating its wall motion and calculating ejection fraction during surgery. Spectral Doppler studies also provided essential hemodynamic and diagnostic information regarding pathologies such as valvular stenosis and valvular regurgitation. TEE imaging frequencies (2.5 to 7.5 MHz) are higher than that of transthoracic echocardiography (TTE), further improving spatial resolution and image quality, providing surgeons with exceptional real-time guidance.
Today, more than 90% of cardiovascular technology and interventional training programs in the United States use intraoperative TEE as a diagnostic and monitoring tool. 2 In 2003, the American Society of Echocardiography (ASE), the American Heart Association (AHA), the American Society of Anesthesiologists, and the Society of Cardiovascular Anesthesiologists presented updated guidelines for the use of intraoperative TEE. 3
Sonographers’ Roles in the Operating Room
Experienced Sonographers in busy hospitals perform multiple tasks including adult and pediatric transthoracic echocardiograms, stress echocardiograms, bubble study echocardiograms, and transesophageal echocardiograms. It has been shown that the role of a cardiac Sonographer has further expanded over time to a presence in the cardiac operating room to assist surgeons in acquiring optimal intraoperative diagnostic images. The American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists (SCA) recently published a joint document titled “ASE/SCA Recommendations and Guidelines for Continuous Quality Improvement in Perioperative Echocardiography,” which supports the position paper, “Guidelines for Cardiac Sonographer Education: Recommendations of the American Society of Echocardiography Sonographer Training and Education Committee,” stating that the Sonographer’s role in the performance of TEE is limited to maximizing image quality by the manipulation of the controls on the ultrasound machine.4–6
Cardiologists, cardiac anesthesiologists, and cardiac surgeons have all become involved in producing perioperative echocardiograms and interpreting the results. Cardiac anesthesiologists particularly have demonstrated a great deal of interest and knowledge of TEE. Although echocardiography skills are outside the main training scope of practice for anesthesiology, cardiac anesthesiologists have accepted the challenge and have become closely involved in programs of education, training, and accreditation. 6 As all aspects of sonography examinations are highly operator-dependent, it is necessary to have qualified and experienced cardiac Sonographers in the operating room to manipulate the controls and functions of the ultrasound system for a complete and diagnostic echocardiogram. Additionally, Sonographers typically have an important role in producing a final comprehensive diagnostic report that physicians rely on for patient management.
Advanced Sonographers have shown their interest in achieving higher education opportunities in their field of studies, and several universities now offer degrees at the Bachelor of Science and Master of Science level in the field of sonography. The American Society of Echocardiography in 1999 proposed an advanced career path for Sonographers titled “Ultrasound Practitioner,” 7 and the Society of Diagnostic Medical Sonography (SDMS) has presented a suggested curriculum for this graduate-level program; 8 any such programs are still under development by national universities.
In 2009, the ASE also proposed a new career path for cardiac Sonographers titled the “Advanced Cardiovascular Sonographer.” 9 Recently, the Commission on Accreditation of Allied Health Education Programs (CAAHEP) approved the new program, 10 which proposes to train qualified Sonographers on a higher level of practice and a broader perspective that will include responsibilities such as supervision, quality assurance, and quality control. It is only natural that responsibilities such as advanced imaging in the operating room be incorporated into the curriculum of any of the proposed career paths for Sonographers so they can perform at a more effective level with the entire cardiac surgical team.
Perioperative Echocardiography
Perioperative echocardiography plays an important role in cardiac surgery by providing assistance in planning, decision making, intraoperative evaluation, and postoperative management. High-quality diagnostic preoperative echocardiography findings result in better surgical planning. Comprehensive POE may reveal new or more specific findings that have the potential to alter both the type or scope of surgery and the method of surgical approach. Changes in surgical decisions will also be influenced by patient consent, specific choices of surgically implanted devices, and the benefit-risk of morbidity and/or mortality based on the complexity of the procedure. 11
The American College of Cardiology and the American Heart Association have presented their recommendations for the use of POE, in which they provided three categories of guidelines (Classes I, IIa, IIb, and III). 3 It is suggested that IOE is most beneficial for patients in Classes I and IIa, which include but are not limited to valvular repairs and replacements, hypertrophic obstructive cardiomyopathy (HOCM), aortic dissection, congenital heart disease repair, transcatheter aortic valve implantation, aneurysm repair, heart transplant, and ventricular assist device implantation. 8 Classes IIb and III include indications such as surgical repair of uncomplicated secundum atrial septal defect, pericardiectomy, pericardial fluid drainage, and coronary artery bypass graft surgery in patients with preserved left ventricular function. These indications do not have a well-established definitive need for intraoperative echocardiography, and opinions are varied as to whether benefits outweigh the risks. 8
Perioperative Transesophageal Echocardiography
The use of transesophageal echocardiography during surgery was first described in the1980s and was widely utilized in the operating room when high-frequency transducers and color Doppler imaging became available. 12 Besides visualizing cardiac structures, TEE allows visualization and evaluation of the thoracic aorta and identification of pericardial effusions and aortic insufficiency. While TEE efficiently guides the surgical approach, it also provides continuous hemodynamic assessment during surgeries for cardiomyopathy, congenital malformations, valvular repairs, and myocardial ischemia. Perioperative TEE has especially been helpful during surgical mitral valve repairs, coronary heart disease interventions (CHD), and left ventricular assessment post heart transplantation. TEE has additionally been shown to provide effective assistance in evaluating the intracardiac results of minimally invasive cardiac surgical procedures such as robotic mitral valve repair. 12 In these procedures, surgeons are able to perform a peripheral cardiopulmonary bypass (CPB), transthoracic aortic cross-clamp, and ante-grade cardioplegia utilizing a robotic platform such as the da Vinci Surgical System, all under the guidance of TEE.
Implantation of a left ventricular assist device (LVAD) requires preoperative TEE to identify left ventricular thrombus or atheroma; it also requires intraoperative TEE for direction and positioning of the cannulae, monitoring of the aortic valve, detection of atrial septal defects, and de-airing of the pump throughout the weaning process. 13 When TEE is used intraoperatively, it provides multiple advantages over epicardiac echocardiography. Its ability to continuously image the heart pre, during, and post surgery makes it the preferred imaging method. Since the TEE probe does not impact on the sterility of the operation field, there is less potential for contamination and postoperative infection. TEE is also preferred over EE because it induces a lower incidence of cardiac arrhythmias.
Although TEE is considered safe, insertion and manipulation of the TEE probe may cause complications that can be oropharyngeal, esophageal, or gastric related. 14 Esophageal perforations may occur in the abdominal region, followed in frequency of occurrence by perforations of the intrathoracic and cervical portions of the esophagus. Esophageal bleeding and unanticipated lesions such as a neoplasm, diverticulum, or inflammatory mucosal changes may result in possible complications as well. Respiratory and cardiovascular complications may include arrhythmias and blood pressure fluctuations. The American Society of Echocardiography stated that limitations of intraoperative TEE include limited potential for optimal Doppler angle alignment, limited time in the surgical setting to perform a complete study, and suboptimal ambient lighting. 15
The ASE established the council for IOE to address issues related to the use of echocardiography in the operating room. The ASE and the Society of Cardiovascular Anesthesiologists provided guidelines for performing a comprehensive intraoperative multiplane TEE examination based on a series of 20 anatomically referenced cross-section images to promote training in TEE and to improve the assessment and interpretation of TEE studies in the operation room. 16 The ASE and SCA guidelines were established to promote an objective approach to achieve accurate diagnosis and management, assist in decision making, and improve the prognosis of surgery in the operating room. At the upper esophageal window, aortic arch short and long axis views are acquired. At the mid esophageal window the views include four-chamber, two-chamber, mitral commissural, long axis, right ventricular (RV) inflow-outflow, atrio-ventricular (AV) short and long axes, and descending aorta short and long axes. At the transgastric level, views include the basal short axis, mid short axis, two-chamber, long axis, and RV inflow. Finally, at the deep transgastric window, a long axis view is captured to view the left ventricular outflow tract, aortic valve, and ascending aorta (Figure 1). 16
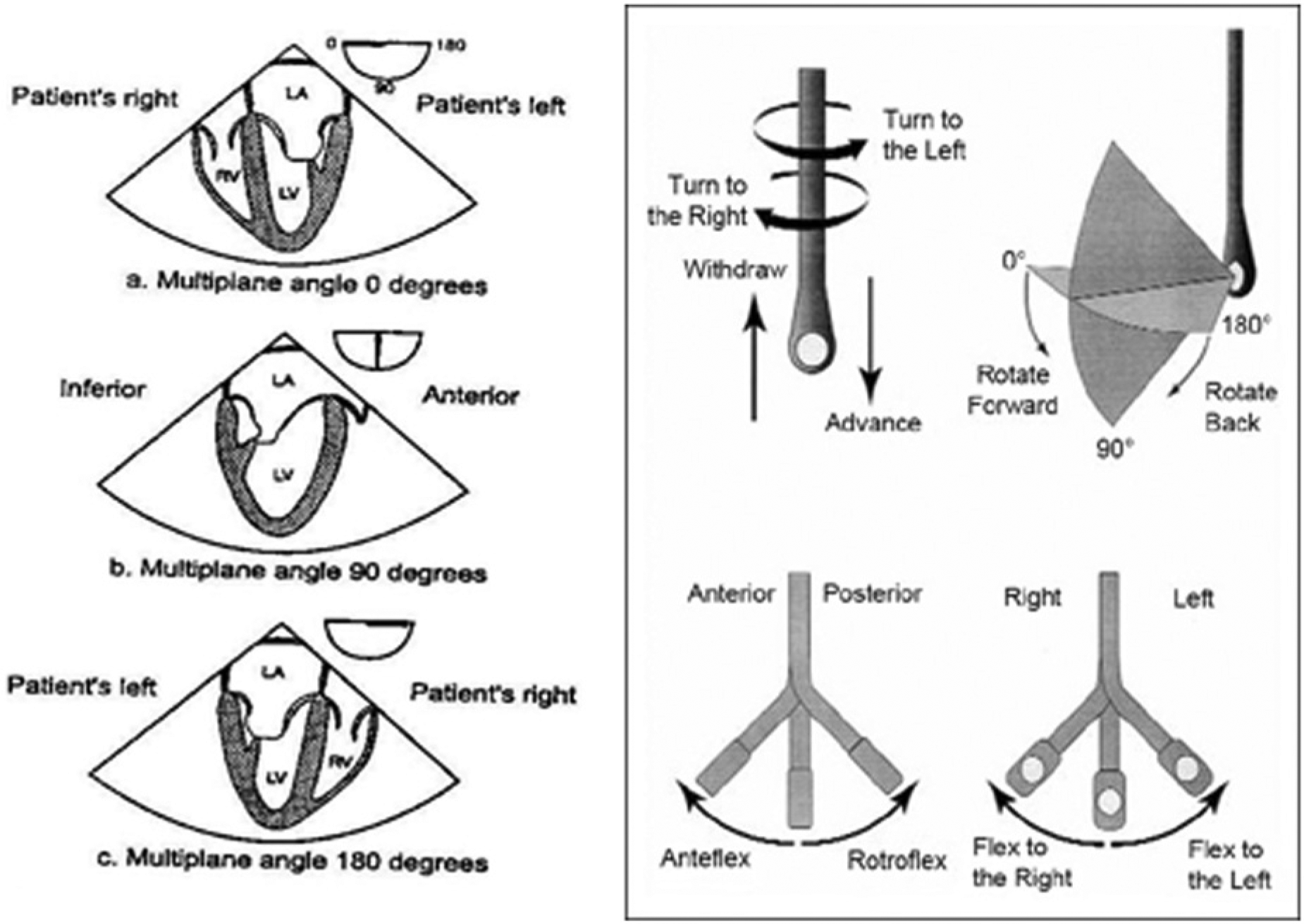
Terminology used to describe manipulation of the transesophageal probe and transducer during image acquisition. (Reprinted with permission from Shanewise JS et al. ASE/SCA Guidelines for Performing a Comprehensive Intraoperative Multiplane Transesophageal Echocardiography Examination. J Am Soc Echocardiogr 1999;12:884–900.).
Pediatric Intraoperative Echocardiography
Until the 1990s, large TEE probe size was a factor that limited its use in the intraoperative evaluation of congenital heart surgery in pediatrics. As smaller TEE probes were developed it was shown that TEE could be safely performed in pediatric patients. The first experience with pediatric intraoperative TEE was described by Cyran et al. in 1989 in children as young as 7.5 years of age using an adult-sized probe for the evaluation of surgical repair of congenital heart lesions. 17 The first probe specifically designed for infants weighing as little as 3 kg was designed by Kyo et al. 18 and Omoto et al. 19 This probe, state of the art for its time, had a diameter of approximately 7 mm and was a 26-element single-plane phased array operating at 5 MHz. 20 Today the surgeon, echocardiographer, and anesthesiologist all work together, using TEE to determine whether the surgical repair is anatomically and hemodynamically successful and whether there are any significant and/or potentially treatable complications to manage before disconnection of bypass cannula, sternal closure, and return to the ICU. 15 TEE also assesses cardiac function and presence of intracardiac air and aids in the diagnosis of cardiac rhythm abnormalities in patients with congenital heart disease. Modern indications for intraoperative TEE in pediatric surgery for congenital heart disease include but are not limited to presence of a patent foramen ovale (PFO), aortic dissection, pericardial effusion, intracardiac thrombus evaluation, prosthetic valve evaluation, and evaluation of extracardiac baffles following procedures such as Fontan, Senning, or Mustard. Intraoperative TEE offers significant aid in surgical guidance during placement of an atrial septal defect (ASD) or ventricular septal defect (VSD) occlusion device, a blade or balloon atrial septostomy, and catheter tip placement for valve perforation, as well as real-time guidance during radio frequency ablation procedures. 15
Epicardiac Echocardiography
Epicardiac echocardiography was used long before intraoperative TEE was introduced. EE can be performed intraoperatively and is considered the most practical imaging tool when TEE is contraindicated or cannot be advanced into the esophagus. TEE may be contraindicated because of esophageal disorders or previous complications. EE’s high-frequency probe offers superior resolution for gray-scale imaging, especially for imaging the aorta, pulmonary veins, aortic valve, and pulmonic valve. EE requires a sternotomy and is performed by placing the ultrasound transducer directly on the epicardial surface of the heart (Figure 2) to acquire 2D, color flow, and spectral Doppler images in multiple planes.21,22 The EE operator must wear a sterile gown and gloves and the probe must be placed in a sterilized sheath to avoid contamination. Warm sterile saline is typically poured into the mediastinal cavity to facilitate imaging. EE is sometimes preferred over intraoperative TEE because the latter does not visualize the distal portion of the ascending aorta and the proximal aortic arch, due to the air-filled bronchi between the esophagus and the aorta. In this case, EE can provide detailed, high-resolution images of the aorta, assisting with the diagnosis of aortic atherosclerosis to assess cross-clamp and balloon insertion risks. Seven views are recommended and should be appropriate for a complete comprehensive 2D and Doppler echocardiographic evaluation in the vast majority of cardiac surgical cases: aortic valve short axis view, aortic valve long axis view, left ventricular basal short axis view, left ventricular mid short axis view, left ventricular long axis view, two-chamber view, and right ventricular outflow tract view.21–23 EE provides very good definition of valvular anatomy and also is effective for the evaluation of valvular stenosis or regurgitation, congenital valvular abnormalities, vegetations, and other lesions. EE is optimal in examining the aorta and locating dissection or intimal tears, lesions, and aneurysms. Hypertrophic obstructive cardiomyopathy (HOCM) is a cardiac disease that involves thickening of the left ventricle, which can obstruct the left ventricular outflow tract (LVOT) over time. Surgical myectomy, removal of thickened cardiac muscle to improve cardiac function in patients with HOCM, is typically done using real-time EE guidance to prevent surgical damage to other areas of the heart. Complications of EE may include contamination, which can be decreased or avoided by following the recommended guidelines of the ASE. Hemorrhage and bleeding are possible complications of open heart surgery, which potentially can limit the use of EE imaging. One limitation of EE is the presence of the probe itself; images and views are obtained by manipulation of the probe and continuous imaging is not possible when the probe is not in contact with the heart tissue. Since EE invades the surgical field, pausing or retracting from imaging is inevitable at times during surgery. Using intraoperative EE effectively requires a diagnosing physician or a cardiac surgeon with advanced perioperative echocardiography training. A more advanced cardiac Sonographer may also be present, depending on the clinical facility, to help acquire the images necessary to provide surgical guidance.
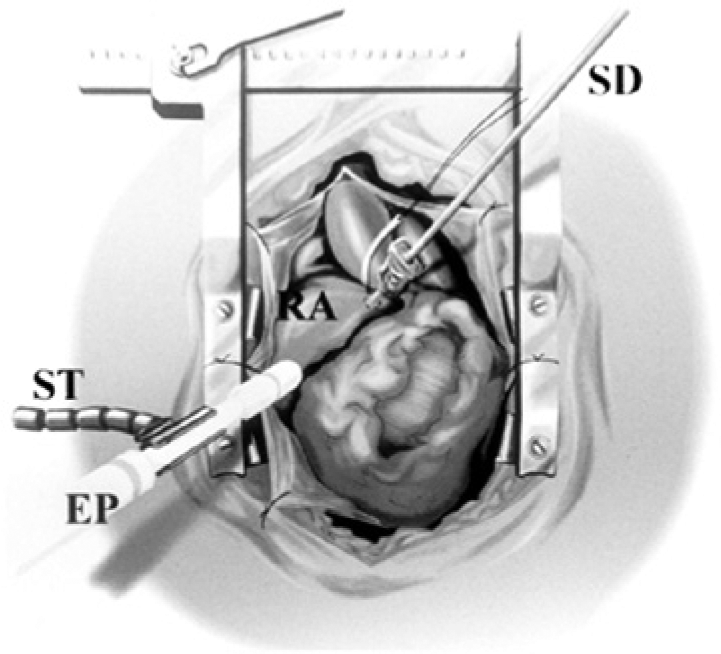
Illustration of an intraoperative view during ep-cardiac echocardiography (EE). The probe is fixed with a stabilizer and directly applied to the surface of the right atrium. EP, echo probe; SD, prototype semiautomatic suture device; RA, right atrium; ST, echo probe stabilizer. (Reprinted with permission from Suematsu Y et al. Beating Atrial Septal Defect Closure Monitored by Epicardial Real-Time Three-Dimensional Echocardiography Without Cardiopulmonary Bypass. Circulation 2003;107:785–790).
Epiaortic Ultrasonography
Epiaortic ultrasonography (EU) is considered to be superior to transesophageal echocardiography when evaluating the aortic arch, ascending aortic atherosclerotic disease, cannulation, and cross-clamp sites. Rosenberger et al. 24 showed that EU influenced surgical decision making in 4.1% of the study population and resulted in a lower overall stroke rate, suggesting the potential for improved perioperative neurologic outcome. In a similar study by Bolotin and colleagues 25 it was shown that EU influenced a change in the surgical procedure in 28% of 105 patients undergoing only coronary artery bypass grafting (CABG) procedures, predominantly a shift from on-pump CABG to off-pump CABG because of significant ascending aortic atherosclerotic disease detected during EU.
Patients undergoing cardiac surgery are at increased risk of perioperative stroke; therefore, EU is essential in evaluating the aorta for atherosclerosis disease. The incidence of stroke varies widely depending on the surgical procedure: 1.9% for off-pump coronary artery bypass graft surgery, 3.8% for on-pump CABG, 4.8% for aortic valve surgery, 8.8% for mitral valve surgery, and 7.4% for combined CABG and valve surgery. 26 IOE has become an important tool in decreasing the surgical risks and complications; studies utilizing EU for aortic screening have suggested improvements in outcome as a result of intraoperative modifications of the surgical plan. 27
Findings and Reports of Intraoperative TEE
Performing TEE in the operation room is different than performing a TEE in the cardiology department for several reasons. A TEE performed in the cardiology department is done for diagnostic and prospective management plan purposes. It generally results in a thorough, well-detailed report that includes diagnostic information that was not seen by TTE. An intraoperative TEE report typically is comprised of a verbal and a written component. The written report should clearly deliver essential information to other medical professionals of all specialties. Where the intraoperative TEE findings have led to a change in the operative surgical procedure or in prognosis, it is essential that this information be unambiguous and available as soon as possible after surgery. 28 The verbal component is given during the procedure with the echocardiographer providing vital information to the surgical team. For example, during mitral valve repair surgery, the surgeon needs to be informed of the nature of the mitral lesion clearly and concisely at the start of the procedure and also needs a clear description of the effectiveness of the surgery at the end of cardiopulmonary bypass. 28 Additionally, the surgeon needs to be acutely aware of any changes to the left ventricle and its overall function during surgery in order to avoid serious complications. This clinical setting emphasizes the need for cardiovascular Sonographers to engage and collaborate with surgeons and anesthesiologists at a higher level in the operating room than in the setting of the typical echocardiography laboratory.
Contrast and 3D TEE
Ultrasound contrast is well known to improve echocardiographic visualization to provide effective assessment of ventricular function. Agitated saline contrast aids in detecting right to left cardiac shunts. Perioperatively, contrast opacifies the left ventricular cavity and enhances the endocardial border for better visualization. Signal processing technologies have been developed that can be used to further enhance contrast visualization. These technologies typically utilize fundamental frequencies and higher order harmonics, allowing imaging frequencies of greater than 12 MHz, to construct real-time perfusion images with high contrast agent-to-tissue specificity and spatial resolution. 29 Second-generation microbubble contrast agents have also been developed to improve contrast ultrasound imaging. These agents are effective during POE to identify intracardiac shunts, enhance the Doppler signal, clarify endocardial borders, and for accurate assessment of cardiac perfusion.
Three-dimensional echocardiography has also been used in the operating room and has been shown to be helpful in a variety of cardiac interventions, such as surgical septal myectomy in the presence of hypertrophic obstructive cardiomyopathy disease. Intraoperative 3D TEE presents improved imaging because it is able to display helpful diagnostic information in anatomic planes not usually seen by 2D imaging. With the aid of perioperative 3D TEE during septal myectomy (Figure 3), the left ventricular outflow tract is better visualized and the systolic anterior motion of the anterior mitral valve (MV) leaflet is better analyzed, leading to a more efficient surgical outcome. 30 Three-dimensional TEE is superior in evaluating the anatomy of mitral valve prolapse and mitral valve stenosis, such as localization of the prolapsed scallops and examination of the deformed mitral valve annulus.31,32 Three-dimensional perioperative TEE has also been valuable in evaluating atrio-ventricular valves, especially after surgical repair of atrial or ventricular septal defects. 33 Intraoperative epicardiac echocardiography has also used the technology of 3D imaging. Using 3D in EE imaging is helpful in providing more accurate diagnostic information for septal thickness, mitral valve systolic anterior motion, and left ventricular outflow tract patency. 34 Although 3D TEE provides diagnostic morphological information to cardiac surgeons, at present it can be time-consuming to perform and involves a delay between capturing full sector volumes and rendering 3D images. Logistically it has been suggested that it is more efficient to engage cardiovascular Sonographers in this imaging process along with the surgical team to obtain the most rapid image turn-around time and the highest image quality possible. 35
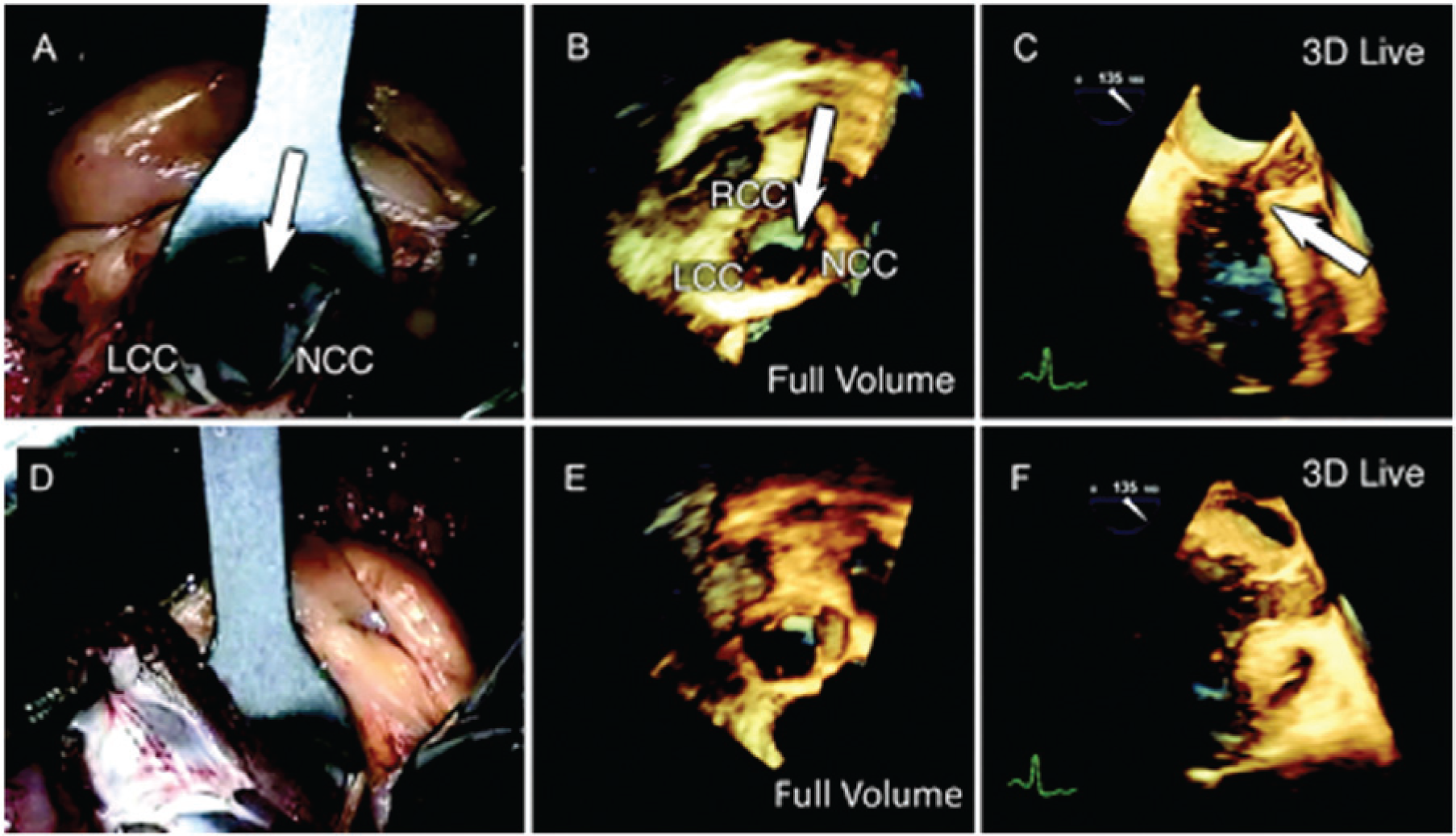
Surgical septal myectomy in a patient with hypertrophic obstructive cardiomyopathy. (A): Thickened interventricular septum (IVS, arrow) through aortic valve at the time of surgery. (B): 3D full volume of aortic root. (C): Thickened IVS (arrow) with 3D of systolic anterior motion. (D): Surgical myectomy performed. (E) Postsurgery aortic root. (F) Postsurgery during systole. LCC, left coronary cusp; NCC, non-coronary cusp; RCC, right coronary cusp. (Reprinted with permission from Vegas A, Meineri M. Three-Dimensional Transesophageal Echocardiography Is a Major Advance for Intraoperative Clinical Management of Patients Undergoing Cardiac Surgery: A Core Review. Anesth Analg 2010;110:1548–1573).
Conclusion
Perioperative echocardiography has been shown to be effective in the evaluation and monitoring of cardiac anatomy and physiology during cardiac surgical interventions, providing in most cases real-time guidance for procedures. Epicardiac echocardiography and transesophageal echocardiography are both used perioperatively to give surgeons the necessary information to optimize interventions and thereby improve outcomes, and each modality has shown unique contributions to the surgical team. For patients with likely or possible aortic disease, EE is often chosen because it is better able to visualize the ascending aortic arch, a limitation of TEE due to the presence of air in the intervening bronchi. TEE is commonly used in the operating room for its superior images and reduced artifacts in visualizing native and mechanical valves. TEE is also preferred because it does not disturb the surgical field, and it allows continuous imaging before, during, and after surgery. Pediatric surgery has also benefited from the use of intraoperative echocardiography, particularly in the repair of congenital heart defects. In the operating room, the surgeons and/or anesthesiologists usually are in charge of manipulating the probe; well-trained and experienced Sonographers are needed to operate the ultrasound machine to take full advantage of its capabilities, determine objective measurements, assist in locating lesions and cardiac dysfunctions, and relate the data and other imaging facts to the surgical team. Perioperative real-time 3D imaging will continue to advance as well and offer its advantages to the surgical team. Echocardiography technology is advancing rapidly, and this will create the ability to serve even more patients with higher quality care. All of this creates more career opportunities and advancement options that can be taken advantage of by cardiac Sonographers, provided they take the initiative to enhance their educational fund of knowledge and sonographic skill set.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.