
Abstract
Carpal tunnel syndrome (CTS) is a form of median mononeuropathy (MMN) of the wrist that has become the most common nerve entrapment syndrome of the upper limbs. During the acute phase of CTS, the median nerve becomes hyperemic and enlarged as it begins to be compressed by the transverse carpal ligament; however, continual compression ultimately leads to median nerve ischemia. The objective of this study was to longitudinally quantify the amount of perfusion of the median nerve using spectral Doppler in a working animal model, as the cohort prospectively increased their risk of MMN through a repetitive pinching task. The results of the study provided low-level evidence that the use of spectral Doppler to accurately detect longitudinal changes in vascularity within the median nerve may be diagnostically inadequate. As the subjects in the study moved through the working and nonworking stages of study, spectral Doppler alone proved to lack the level of sensitivity needed to detect physiologic changes within the nerve. This outcome, although inconclusive when it comes to detecting changes in median nerve vascularity, does suggest the need for this method to be analyzed in conjunction with other sonographic features and provocative testing.
Introduction
Carpal tunnel syndrome (CTS) is a form of median mononeuropathy (MMN) of the wrist that has become the most common nerve entrapment syndrome of the upper limbs. Carpal tunnel syndrome affects slightly less than 5 million people in the working population of the United States, with approximately 849 000 new cases reported each year in this country alone.1 -3 This musculoskeletal (MSK) disorder is characterized by compression of the median nerve as it passes through the carpal tunnel in the distal forearm. The carpal tunnel, defined by the area surrounded by the anatomical boundaries of the transverse carpal ligament superiorly and the first row of carpal bones inferiorly, provides space for the median nerve to travel distally for innervation of parts of the hand and digits. 4 However, the most common risk factors for CTS are exposure to vibrations, direct compression, and highly repetitive and forceful hand-wrist motions which will ultimately cause this space to in the carpal tunnel to diminish. 5 Individuals suffering from other pathologies such as rheumatoid arthritis, hyperthyroidism, acromegaly, and diabetes mellitus are also at an increased risk for developing this entrapment disorder. 6
During the acute phase of CTS, the median nerve become hyperemic, is accompanied by intraneural edema, and becomes enlarged as it begins to be compressed by the transverse ligament. 3 However, these acute physiologic changes are often subtle and go unnoticed by the afflicted individual, as they most often occur at night.4,7 As the compression becomes chronic and CTS symptoms become evident, microtrauma consisting of demyelination of the nerve sheath occurs from the repetitive excursion of the median nerve through the constricted carpal tunnel space.4,8 This continual compression ultimately leads to median nerve ischemia at the site of compression. 9 Concentrating on the arterial perfusion aspect of the pathophysiologic response within the median nerve, it is plausible to attempt to observe changes in the arterial blood flow in and around the nerve throughout the progression of this disorder. Previous studies have been carried out to determine the vascularity of the median nerve and its contribution to the disorder; however, few have used spectral Doppler to obtain a quantitative value for the perfusion of the median nerve.
A systematic literature review was conducted to determine the current level of evidence that has been published with regard to the spectral Doppler detection of blood perfusion within the median nerve. The utility of MSK sonography was verified in a study that successfully demonstrated the capability of MSK sonography in detecting and quantifying arterial blood flow within the median nerve in a population of diagnostic medical sonographers. 10 Five neonatal sonographers were followed longitudinally and for 10 weeks received MSK sonograms of the wrist to evaluate median nerve perfusion. These examinations were completed before and after each sonographer conducted a neonatal head sonogram. Peak systolic and end diastolic velocity measurements throughout the median nerve were recorded, and although these quantitative variables did not show statistically significant variation, the study was successful in demonstrating the feasibility of using spectral Doppler as a method of interrogating median nerve perfusion.
In a retrospective analysis conducted by Evans et al, spectral Doppler tracings of patients who were symptomatic and asymptomatic for CTS were analyzed. 4 One hundred sixty-six wrists were analyzed in 47 symptomatic and 44 asymptomatic patients who were to have nerve conduction studies done. The study analyzed a total of 435 spectral tracings that was then reduced to 245 waveforms after a set of exclusion criteria was applied. Examination of the peak systolic velocities (PSVs) showed no appreciable difference between the symptomatic and asymptomatic recruitment groups. This study also evaluated the possible correlation between spectral Doppler tracings and provocative testing, but due to limited sample sizes, no statistically significant data could be recovered. These same 245 spectral Doppler waveforms were then compared with electrodiagnostic testing results obtained on the same patients. Peak systolic velocities were correlated with nerve conduction velocity (NCV) results, which determined that there may be an inverse relationship between them in patients with symptoms consistent with CTS. 8
A more detailed retrospective analysis was carried out in a population of subjects that divided the hands in the study into the categories of highly likely CTS patients and indeterminate CTS patients, based on nerve conduction studies. Nerve conduction data were analyzed along with cross-sectional area (CSA) measurements of the median nerve and intraneural spectral Doppler tracings. In the wrists evaluated, which contained elevated intraneural PSV, there was a sensitivity of 83% in differentiating patients with CTS from the highly likely CTS group. When the use of spectral Doppler was combined with an increase in median nerve CSA, the sensitivity increased to 90% in differentiating patients with CTS from the highly likely CTS group. 9
Those few studies that evaluated spectral Doppler waveforms as a part of the research design were limited to evaluating the median nerve of symptomatic individuals with CTS and of asymptomatic patients based on the single time point of their appointment. Based on the different pathophysiologic changes that occur throughout progression of CTS, the median nerve should be evaluated longitudinally at different stages of the disorder. The objective of this study was to longitudinally quantify the amount of perfusion of the median nerve using spectral Doppler in a working animal model, as the cohort prospectively increases their risk of MMN through a repetitive pinching task. These data could in turn answer the research question as to the utility of spectral Doppler tracings gathered during a MSK sonogram and examine the potential to detect changes in the microvasculature within the median nerve in patients.
Materials and Methods
Data Collection
The study was approved by the Institutional Animal Care and Use Committee board of review prior to initiation. The study was completed using 14 macaca fascicularis monkeys as participants in MMN research. During a 20-week working phase, the 14 macaca fascicularis performed a repetitive squeezing task involving the left wrist, placing them at risk for developing MMN. 11 Figure 1 shows an illustration of the apparatus used to perform the squeezing task during the working phase. This apparatus was monitored by a LabView system (National Instruments, Austin, Texas) that recorded performance via a pulley circuit, which included a potentiometer that provided an analog record of the degree of tong closure, to ensure that the repetitive squeezing task was being completed. Two sonograms were completed prior to work exposure in order to obtain baseline data. Ten subsequent sonograms were completed on each subject during the working phase of the study to capture any longitudinal physiologic changes. These sonograms were completed every other week for the 20-week working phase, yielding 10 working phase scans. Two additional sonograms were completed post-work exposure, referred to as the recovery stage of the study.
Illustration of the task apparatus used for the subjects to perform a squeezing task during the working phase of the study to attempt to induce median mononeuropathy (MMN).
A previously reported MSK sonography protocol was refined and replicated to evaluate perfusion of the median nerve quantitatively using spectral Doppler.12,13 Three sonographers used a GE Logiq i hand-carried unit (HCU; GE Healthcare, Milwaukee, Wisconsin) to scan the subjects, using a 12.0 MHz linear probe, with a bandwidth of 7 to 12 MHz. For all studies, a 12.0 MHz probe frequency was selected. Time gain compensation controls were aligned vertically and centered, and tissue harmonics and wide aperture (CrossBeam®) imaging features were also used. Technical factors standardized for the gray-scale image were frequency (12 MHz), power output (100%), and B-mode gain (66). Each wrist was scanned in the longitudinal plane to obtain an optimal view of the median nerve. Power and spectral Doppler was applied to the gray-scale image and optimized using a standardized set of technical settings (Figure 2). Multiple tracings were obtained for each subject during each scan at a variety of locations within the median nerve throughout the carpal tunnel. Boundaries of the carpal tunnel were defined by the anatomical landmark of the most distal portion of the radius. Proximal to this location was defined as the carpal tunnel inlet, and distal to the landmark was defined as the carpal tunnel outlet. Spectral Doppler tracings were obtained at sites identified as having flow displayed by the power Doppler image. Because of the very small size of the intraneural vasculature and the inability to determine the precise direction in which the blood vessels were traveling, no angle correction was applied when obtaining the spectral Doppler tracings. 4 To determine if compression was taking place due to the inflammation of the median nerve throughout the MMN disease progression, transverse gray-scale images were also acquired to evaluate the cross-sectional area of the median nerve longitudinally. 2 Weekly quality control measurements were performed with the transducer and a tissue mimicking phantom throughout the study to monitor and document the reliability and reproducibility of equipment performance.
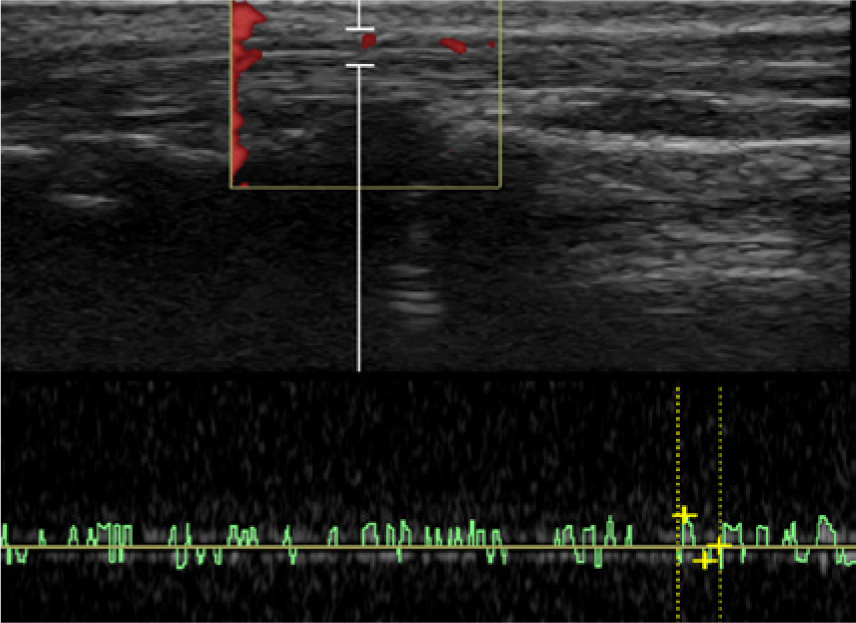
Longitudinal view of the median nerve using power and spectral Doppler showing arterial flow within the nerve.
Image Analysis
All spectral Doppler waveforms were analyzed retrospectively by two credentialed sonographers. The research sonographers were blinded to the subject as well as the time point in the study in which images were obtained. All image and waveform analyses were completed on the same GE Logiq i HCU that was used to collect the data. Strict inclusion criteria were developed and applied to both the power Doppler image portion and spectral Doppler tracings in order for these data points to be included in the study 4 :
Must have at least three cardiac cycles in the spectral tracing
Must have the spectral Doppler gate positioned within the median nerve
Must have a power Doppler pixel in the gate
Must not be using angle correction
Must have an optimized gray-scale image
Must have more signal than noise in the spectral tracing
The PSV and end diastolic velocity (EDV), as determined from the automatic trace function present on the HCU software, were then recorded for each waveform in order to meet the inclusion criteria. The autotrace function of the ultrasound unit was used to differentiate between arterial signals and noise artifacts on the spectral Doppler to provide a standard and strict criterion as to the inclusion or exclusion of waveforms.
Data Analysis
The number of total waveforms and means of the PSVs at both anatomical locations were calculated for waveforms meeting the inclusion criteria. The mean PSV and the maximum PSV were retained for each subject at the proximal portion of the carpal tunnel. The maximum PSVs of the median nerve gathered in the left (working) and right (nonworking) wrists were trended longitudinally to give a qualitative representation of the data throughout the working stages of the study. Similarly, the mean PSVs recorded in the proximal portion of the median nerve were trended longitudinally in an attempt to observe patterns in the data throughout the different stages of the study. These data were further broken down into graphs trending the maximum PSVs for the two cohorts of the study (years 1 and 2) and for each individual subject.
Results
Inclusion of Waveforms
Overall, 1445 waveforms were collected from the 14 macaca fascicularis subjects. Of these, 812 failed based on the exclusion criteria, yielding a total of 633 waveforms that were considered valid for analysis. There were 235 duplicate dated waveforms that were removed, along with 3 others because of missing key data points, leaving a total number of 395 waveforms suitable for analysis. This total included waveforms from both anatomical locations (Figure 3). Each waveform had the ability to be excluded from the study based on more than one error located within the image, so that the sum of the individual exclusions is greater than the total number of waveforms excluded.
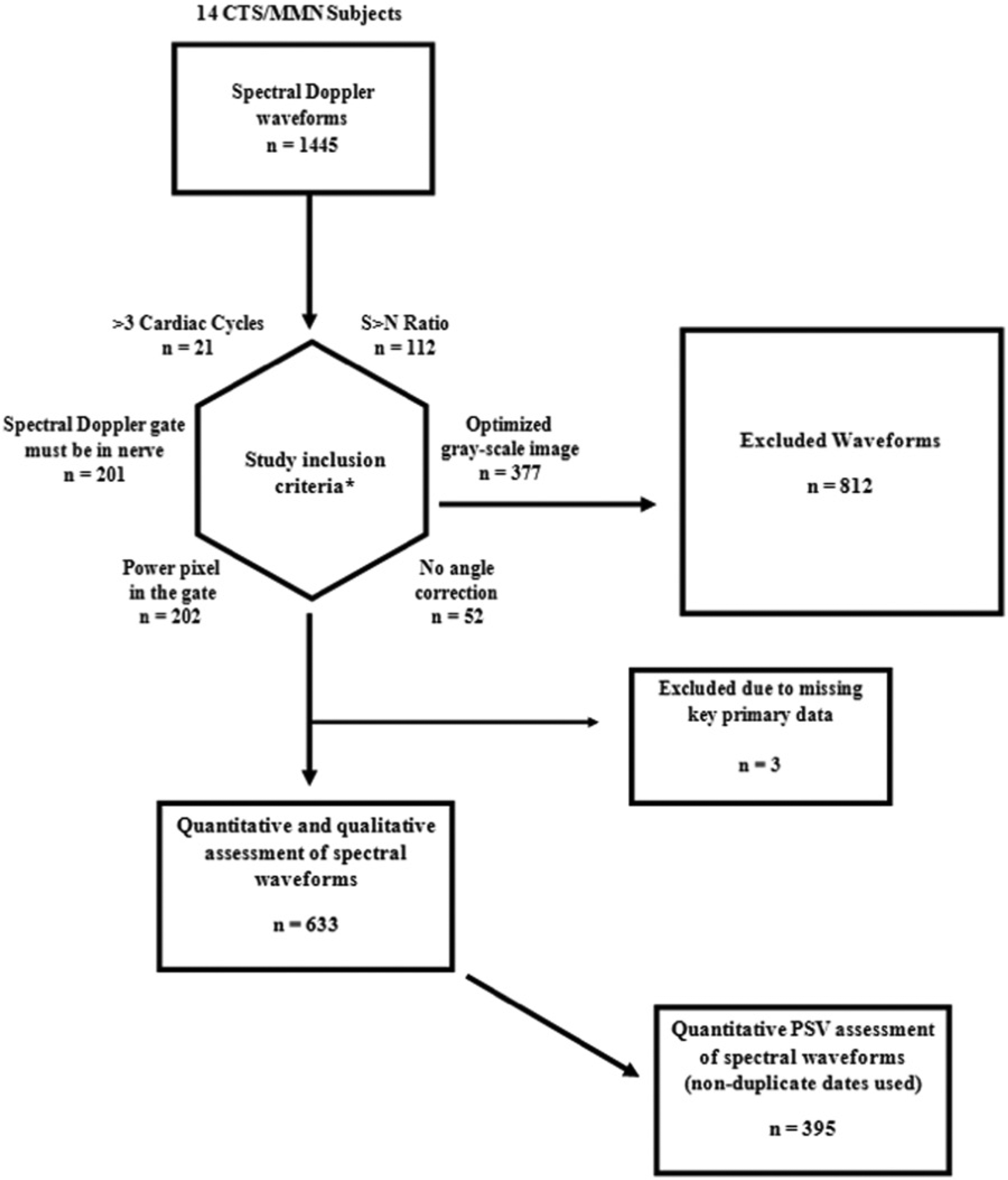
Inclusion/exclusion flowchart for assessment of Doppler waveform morphology and quantitative data points. *Criteria are not mutually exclusive, with some waveforms failing multiple criteria; numbers following each criterion indicate the count of waveforms that did not meet that individual inclusion criterion.
Descriptive Results of Waveforms
The PSVs were collected and tables of descriptive data created for both the working and nonworking arm of the subjects. Subjective analysis of the collective data was more readily appreciated by constructing longitudinal trend graphs that depicted the maximum PSV collected over the length of the study for the nonworking wrist (Figure 4) and the working wrist (Figure 5). The mean PSVs were analyzed for each subject at the anatomical location of the proximal carpal tunnel. These data points were trended longitudinally for the nonworking and working wrists of each individual subject in an identical manner to that of the maximum PSV (Figures 6 and 7, respectively).
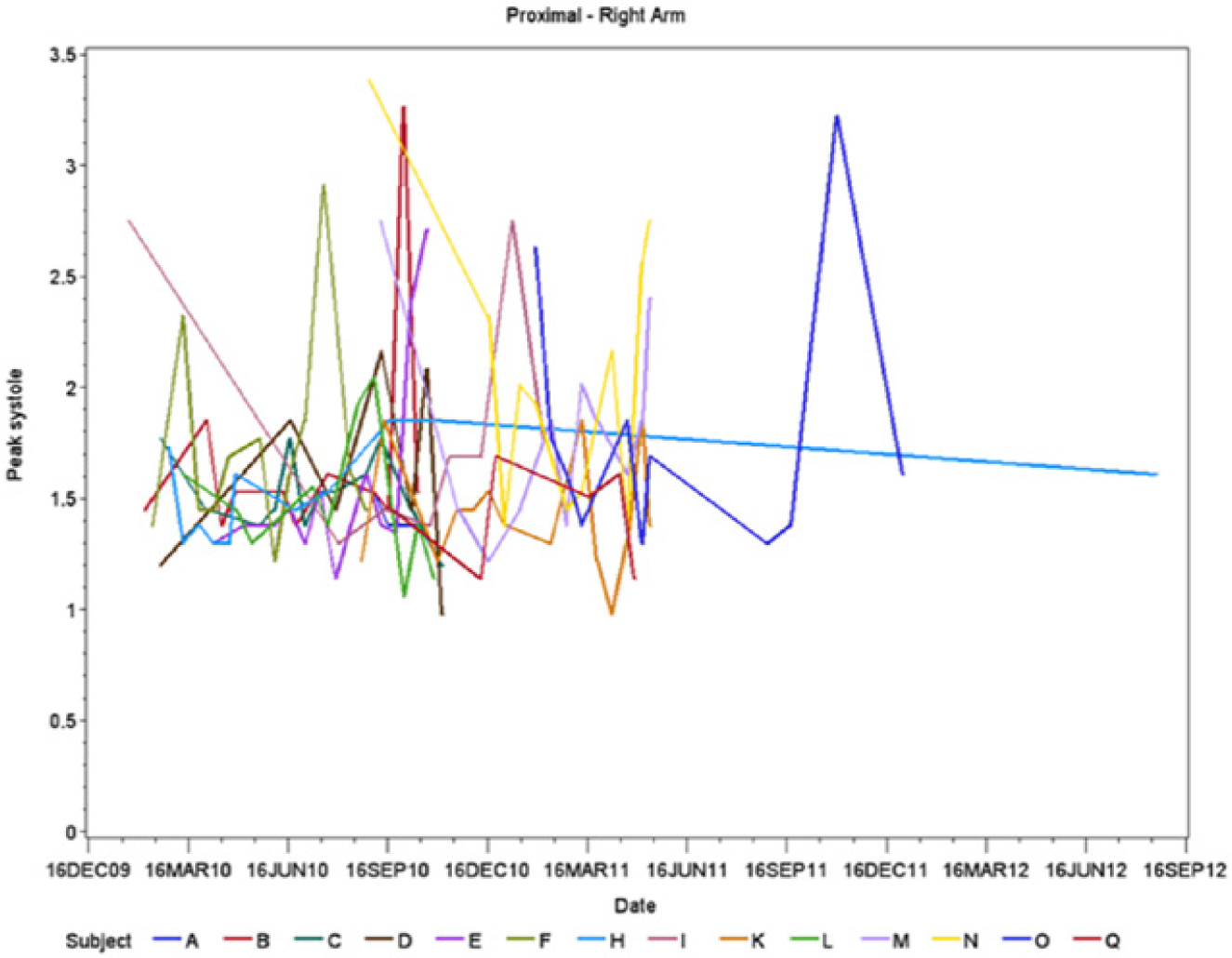
Trend graph of data points representing maximum peak systolic velocities (PSVs) of individual subjects gathered from the proximal portion of the right (nonworking) wrist.
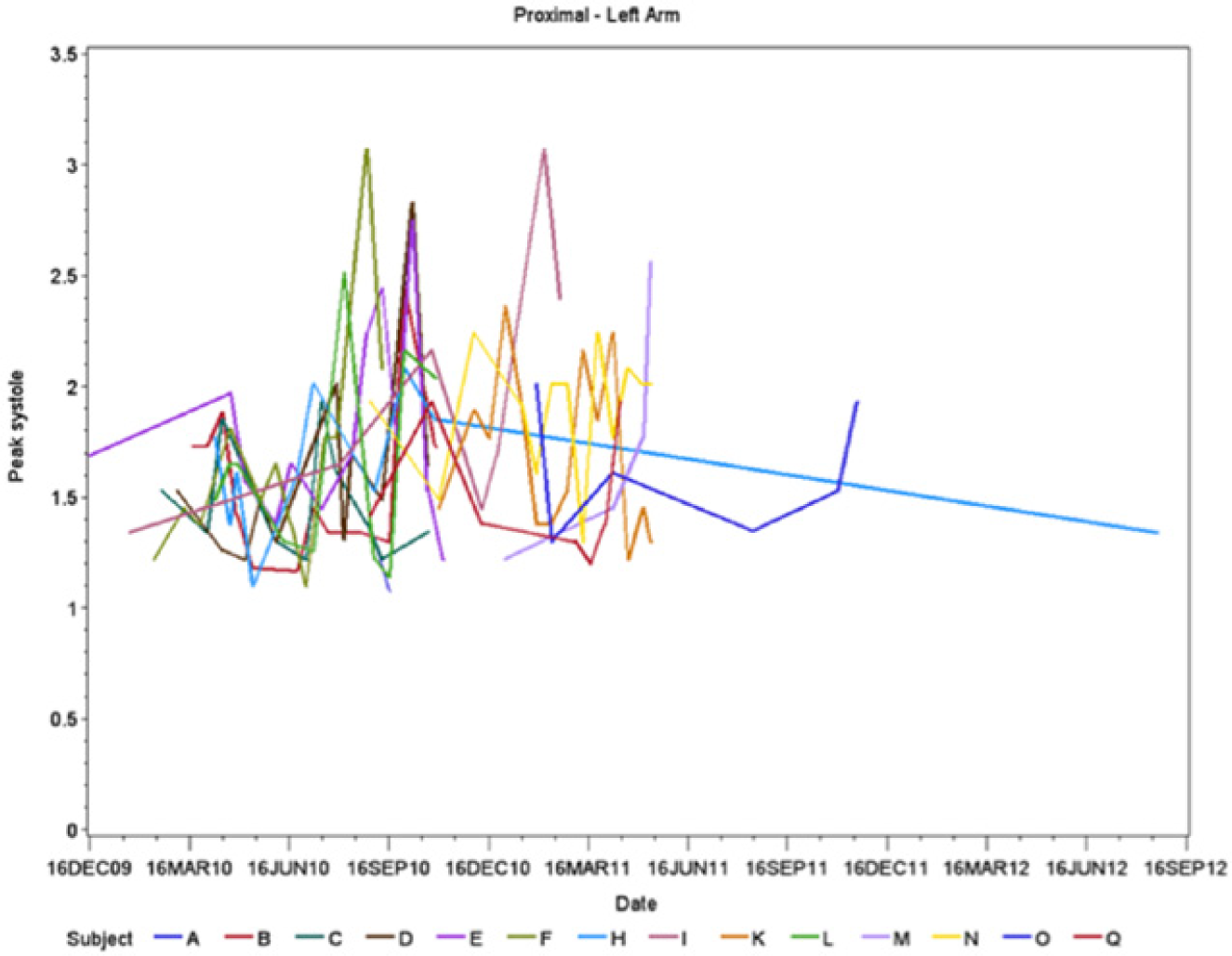
Trend graph of data points representing maximum peak systolic velocities (PSVs) of individual subjects gathered from the proximal portion of the left (working) wrist.
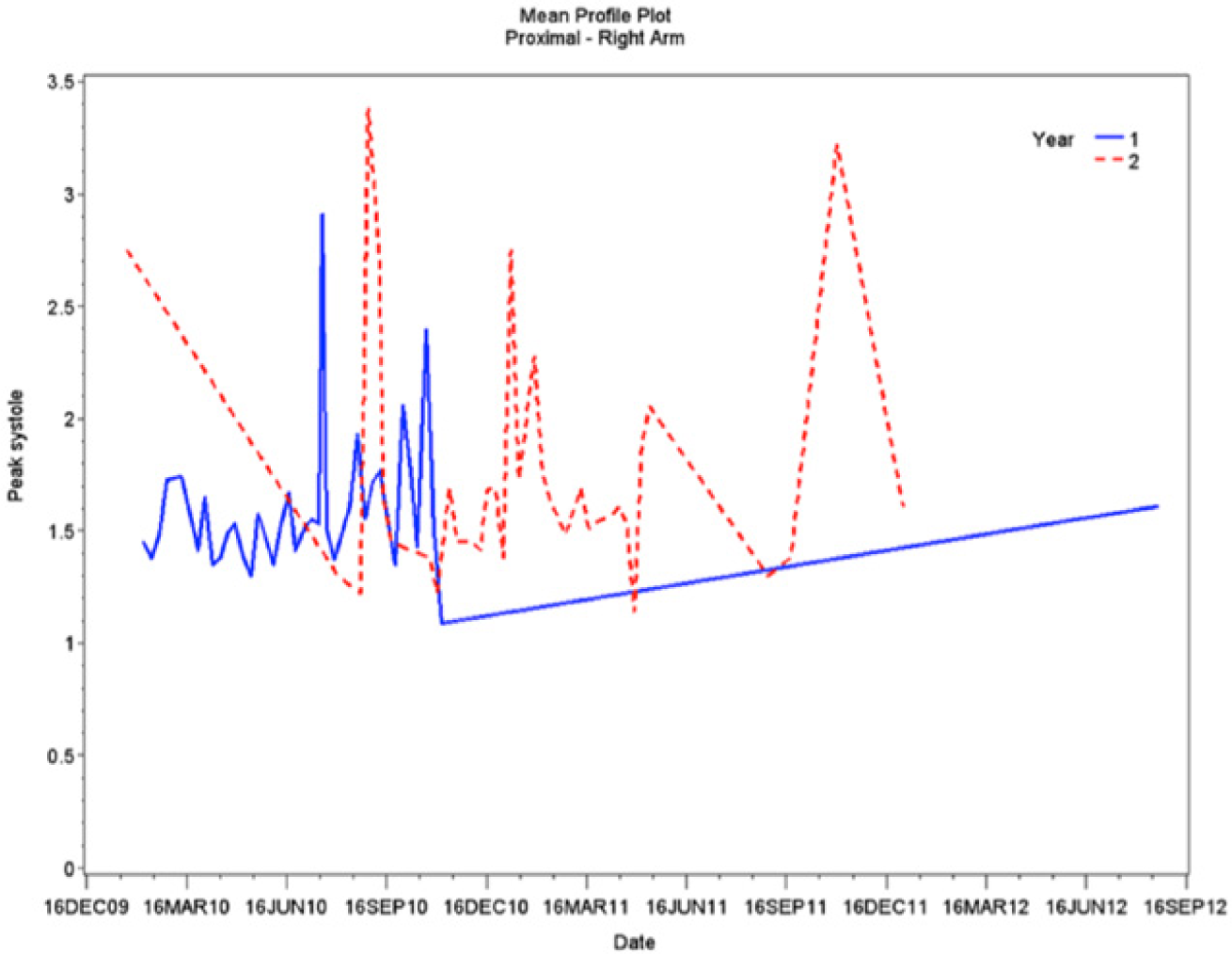
Trend graph of data points representing the mean peak systolic velocities (PSVs) gathered from the proximal portion of the right (nonworking) wrist.
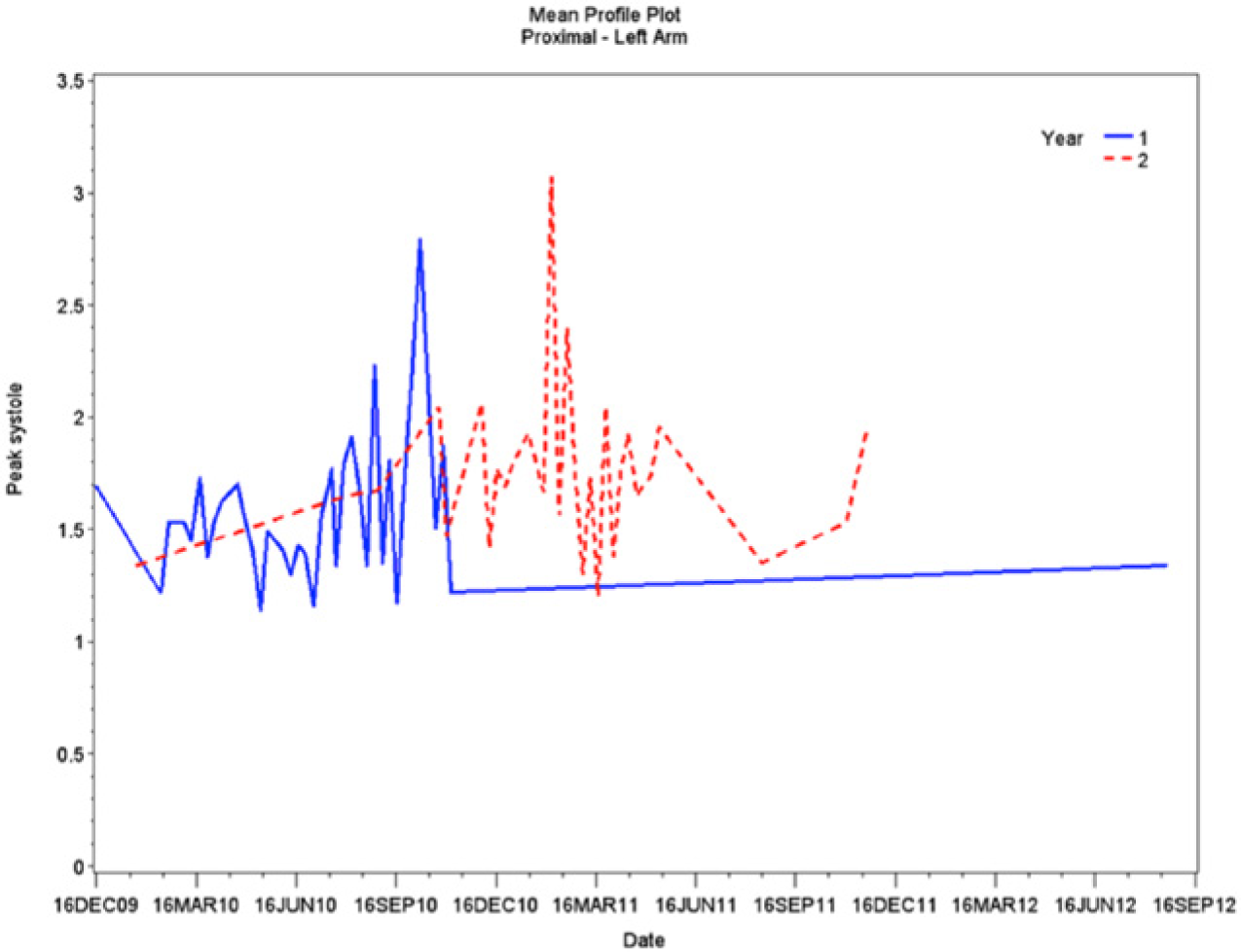
Trend graph of data points representing the mean peak systolic velocities (PSVs) gathered from the proximal portion of the left (working) wrist.
Discussion
This is the first study to analyze arterial spectral Doppler waveforms from the median nerve, in order to gather information on MMN longitudinally, by gathering quantitative data depicting the blood flow with the microvasculature of the median nerve. This study was devised to determine the utility of this application of sonography. Since the cohorts of subjects participated in different phases throughout the study (baseline, working, and recovery), this represented a unique opportunity to examine the development of this disorder. The decision was made to investigate only the proximal portion of the median nerve within the carpal tunnel based on the pathophysiology of MMN. The median nerve has been described with swelling in the segment of the nerve just proximal to the site of compression. 14 Because of the hyperemic response associated with the inflammation process, this proximal segment of the nerve was deemed most likely to demonstrate the greatest change in intraneural blood flow activity and this site was regarded as most appropriate for investigation with spectral Doppler.
Theoretically, the baseline scans, completed before the subjects began the repetitive working phase of the study, should have displayed consistency throughout subsequent biweekly scans. Once the working phase began, the goal was to increase the risk of acute physiologic changes to the median nerve. As repetitive wrist movements occur, the inflammatory response of the median nerve begins. Subsequently, the enlarged nerve experiences microtrauma due to the repetitive movement through a restricted space within the carpal tunnel. 4 This microtrauma and swelling create the hypervascularity of the median nerve that was the basis of the expected rise in PSVs during the working phase. This was not in fact documented with the data collected during this study. Similarly, corresponding qualitative changes were expected in the trended data, which reflected the subjects’ completion of work exposure and recovery. Throughout the working stage, this risk of injury to the median nerve increased as the subject completed a repetitive squeezing task. Once the recovery phase began, the subjects’ risk was reduced and the constant irritation of the nerve was ameliorated. However, due to the microvasculature damage that may have occurred, resulting chronic changes could have developed. Unlike the acute phase, this is characterized by ischemia and scarring of the median nerve, which can impair sensory and motor abilities.15-17 Given our understanding of this pathophysiology, a drop in PSVs to approximately equal to or below the original baseline values was expected. However, like the transition from the baseline to working stage of the study, no detectable differences in peak systolic values could be demonstrated qualitatively.
These results are consistent with the study conducted by Evans et al in which power and spectral Doppler was used to evaluate median nerve behavior in a group of working general and vascular sonographers. 17 Data were collected the first week of the study in a prescanning MSK examination and then 5 weeks later in a postscanning MSK examination. This study presented a limited data set, though change scores of the average peak systolic values recorded within the median nerve were able to be carried out, which resulted in very little difference between the pre- and postscanning examinations. This result of MSK sonography lacking the sensitivity to detect any reasonable microvasculature change is consistent with the data generated in the current study, as no discernible pattern could be distinguished. Ghasemi-Esfe et al reported similar results of indeterminate data while analyzing intraneural vascularity. 18 Patients with a certain diagnosis of CTS were evaluated using a multivariate approach to analyze potential risk factors discovered in the MSK wrist sonogram. These factors were analyzed along with the nerve conduction data of the patient inflicted with CTS, and again, spectral Doppler was not sensitive enough to be used as a single discriminator of CTS.
Despite the unsuccessful results of the current study, using nerve hypervascularity as a diagnostic tool to aid in the diagnosis of CTS still appears to hold some promise but needs further investigation. In a study conducted by Mallouhi et al, a MSK sonogram was completed on 206 wrists among patients reporting symptoms of CTS. 19 Factors such as nerve appearance, edema, and the presence of nerve hypervascularity were examined simultaneously. The study demonstrated that when compared with nerve conduction studies, nerve hypervascularization had the highest accuracy over all other sonographic measures. This study differed from the current research in the method by which hypervascularity was determined. Mallouhi et al captured only color Doppler signals as a means of determining the presence of a hyperemic nerve. These color Doppler signals were characterized by the presence of any intraneural structures not related to the persistent median artery, and this increased nerve vascularity was reported statistically in a 2-point nominal fashion: present or absent. This method of determining hypervascularity was nearly duplicated in a more recent study by Rahmani et al in which any intraneural vascularity demonstrating pulsatile blood flow was considered as hypervascularity of the median nerve. 20 A limitation of all of these studies is that representative velocities are more accurately captured through the use of angle correction within the spectral Doppler gate. Therefore, any future replication study would advocate the use of angle correction.
Throughout the current study, it became apparent that with the proper technical settings, intraneural vascularity was present within the median nerve during every sonogram performed. Adopting this methodology in the current study for determining median nerve hypervascularization, however, would not have possessed adequate sensitivity. This underscores the need to further investigate the use of spectral Doppler analysis for quantifying intraneural vascularity. An innovative approach to assessing nerve vascularity that may alleviate the problem of diminished sensitivity would be to amplify the intraneural waveforms as recorded by spectral Doppler through the use of contrast-enhanced ultrasound. By injecting a microbubble-based contrast agent, detection of low-volume blood flow can be improved significantly by increasing the signal-to-noise ratio.21,22
Limitations
This preclinical study would have increased the data collected and statistical rigor by the addition of more subjects in the experimental cohort. A replication of this study would require that a direct measure of the force during the repetitive squeeze task be recorded and this would have made the present study more robust, as the work effort could have been quantified. This would have ensured that the repetitive squeezing task was truly being completed by the subjects, ruling out any threats to the validity of the model. Statistically, while comparing the left (working wrist) with the right (nonworking wrist), the nonworking wrist would ideally be used as the control variable, allowing an intra-subject comparison to be made. However, caution should be exercised when a subject serves as his or her own control due to the changes within the median nerve that could be attributed to other underlying medical conditions such as pregnancy or diabetes. These confounding variables could readily cause unilateral manipulation not to be the exclusive variable causing median nerve changes.
Conclusion
This study provides low-level evidence that the use of spectral Doppler to accurately detect longitudinal changes in vascularity within the median nerve may be diagnostically inadequate. As the subjects moved through the working and nonworking stages of the study, spectral Doppler waveform analysis alone proved to lack the level of sensitivity needed to detect physiologic changes within the nerve. This outcome, although inconclusive when it comes to detecting changes in median nerve vascularity, does suggest the need for this method to be analyzed in conjunction with other sonographic features and provocative testing. Cross-sectional area, nerve echogenicity, and color and/or power Doppler signal counts have all demonstrated validity and the ability to provide useful data in previous studies in the diagnosis of CTS. The investigation of sonographic features being used as a diagnostic adjunct should not be abandoned, and a longitudinal study combining all of these factors and analytically comparing the changes observed would appear to be the next logical step.
To quantitatively examine the hypervascularity of the median nerve, the use of a contrast agent to amplify the spectral Doppler signal returning from the microvasculature in the nerve will likely prove beneficial. 21 It is hoped that these waveforms, with strong signal-to-noise ratios, would possess the sensitivity to demonstrate a detectable difference as the progression of MMN occurs. It would be further possible to compare these contrast-enhanced Doppler waveforms to T2 weighted magnetic resonance imaging MSK scans. As set forth by the American College of Radiology Appropriateness Criteria, magnetic resonance is the imaging gold standard for diagnosing acute wrist pain. Therefore, a direct comparison between intraneural vascular intensity, collected through the use of MSK ultrasound, and median nerve signal-to-noise ratio, collected through the use of magnetic resonance imaging, would be appropriate. 23
Footnotes
Acknowledgements
The authors thank John A. Buford, PhD, for the use of his lab and support in conducting this preclinical study. His expertise in animal training and measuring work effort is greatly appreciated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was made possible by a grant from the National Institute of Occupational Safety and Health R21 OH009907-02 and the ASRT Foundation.