
Abstract
Transperineal sonography is a diagnostic tool for imaging the pelvic floor and lower pelvis. Because of the higher spatial resolution of pelvic sonography compared with other cross-sectional imaging techniques, transperineal sonography can provide detailed visualization of the lower pelvic organs, including the urethra, vagina, and anorectum. This case report describes the use of transperineal sonography for evaluation of an indeterminate lower pelvic process seen on computed tomography in a 53-year-old woman with progressive pelvic pain, dysuria, and dyspareunia. Because of severe dyspareunia, the patient declined transvaginal sonography. Transperineal sonography provided diagnostic imaging of the anal mass causing these symptoms.
Transperineal sonography is a diagnostic imaging tool used to evaluate the pelvic floor and lower pelvis.1,2 This approach allows visualization of the urethra, vagina, anorectum, lower uterus, and base of the bladder without insertion of a vaginal or rectal transducer. Indications for transperineal sonography include perineal pain, perineal trauma, vaginal or anorectal obstruction, lower pelvic tumors, abnormal urination or defecation, and pelvic floor dysfunction. 1 This sonographic approach is also useful for image-guided lower pelvic procedures, evaluation of perianal disease in patients with Crohn’s disease, assessment of anal sphincter integrity, and assessment of cervical length and fetal head position during pregnancy.1,3–6 Adequate visualization of the muscles of the male pelvic floor with transperineal sonography has been reported. 7 Evaluation of congenital abnormalities of the lower urinary, gynecologic, and intestinal systems has been reported in pediatric patients.8,9 When internal sonography is contraindicated, such as for patients who have undergone recent perineal or pelvic surgery, patients with dyspareunia or vaginal pain, pregnant patients with suspected ruptured membranes, or patients with vaginal obstruction, transperineal imaging may be a useful alternative. This technique may also be useful when computed tomography (CT) or magnetic resonance (MRI) imaging is contraindicated, nondiagnostic, or indeterminate. Transperineal sonography also provides higher spatial resolution than CT or MRI. 10
Case Report
A 53-year-old premenopausal woman with a history of nephrolithiasis, hypothyroidism, scoliosis, and ulcerative colitis diagnosed in childhood presented to an outside institution with 2 months of progressive pelvic pain. The patient was status post total colectomy 24 years prior to presentation with a J-pouch ileoanal anastomosis complicated by recurrent inflammation of the J-pouch. Recent symptoms began with dyspareunia, followed by pain with sitting, dysuria, dyschezia, and pain radiating down the right leg with movement. The patient denied vaginal bleeding or rectal bleeding at the time of presentation. The patient was afebrile without leukocytosis. The pelvic examination was limited because of severe pain. At the outside institution, a CT was performed, which demonstrated abnormal soft-tissue density along the anterior wall of the intestinal J-pouch, irregularity of the wall of the J-pouch, and obliteration of the fat planes between the vagina and the J-pouch. The differential diagnosis included inflammation of the J-pouch and tumor. The patient was transferred to a tertiary care center and admitted for further evaluation and management.
Upon admission, further imaging was requested because of the nonspecific appearance of the pelvic abnormality on CT. MRI was deferred because of the presence of spinal hardware (status post T6-L1 spinal rod placement for scoliosis). The patient was transferred to the sonography department for an internal pelvic sonogram, which was deferred by the patient because of severe vaginal pain. After review of the CT (Figure 1) and discussion with the patient and clinical team, a transperineal sonogram was performed to assess the inferior pelvic abnormality. Because of urinary frequency, the patient voided immediately prior to the examination.
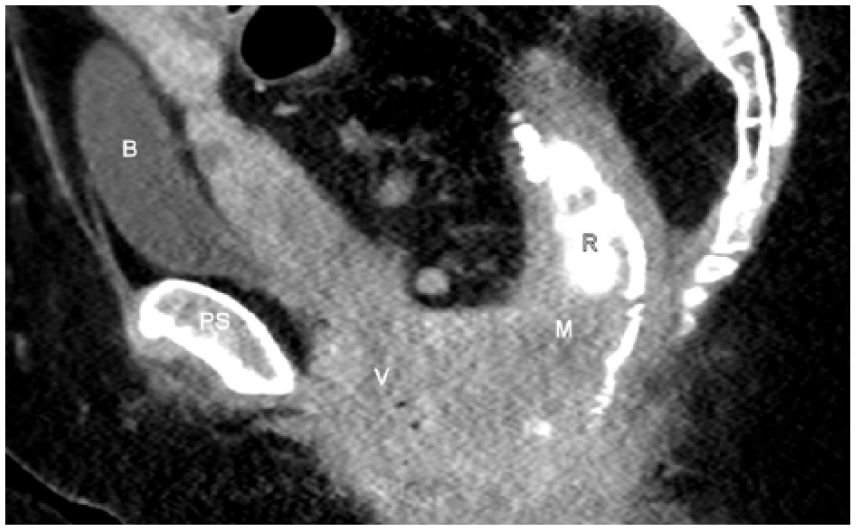
Sagittal computed tomography (CT) image of the pelvis demonstrates abnormal soft tissue (M) between the vagina (V) and rectum (R) with narrowing and irregularity of the rectal lumen (enhanced by oral enteric contrast administration). Prospective CT interpretation was infection or mass. PS, pubic symphysis; B, bladder.
The sonographic examination was performed with a GE Logic E9 (GE Healthcare, Milwaukee, WI) using a C 1-5 MHz curved linear array transducer for the transabdominal portion and a 9-MHz linear array transducer for the transperineal portion. For the transperineal examination, the transducer was covered with a probe cover. Acoustic gel was used underneath the probe cover as well as outside the cover to eliminate any air between the transducer and the perineum. Gray-scale images were acquired with a frequency of 8.4 MHz, overall gain of 48, depth of 10 cm, dynamic range of 63, and acoustic output of 100%. Color Doppler images were acquired with pulse repetition frequency 1.1 and wall filter 119.
The transabdominal study demonstrated an enlarged heterogeneous uterus with subcentimeter myometrial cysts, consistent with adenomyosis, and bilateral small simple ovarian cysts. The area of concern between the vagina and intestinal pouch could not be seen transabdominally.
Transperineal imaging in the sagittal plane (Figure 2a) demonstrated a 5.0 x 4.1 x 3.1 cm solid well-circumscribed mildly echogenic mass with internal vascularity (Figure 2b), located between the vagina and the distal intestine. The origin of the mass (vaginal versus intestinal) was indeterminate sonographically.
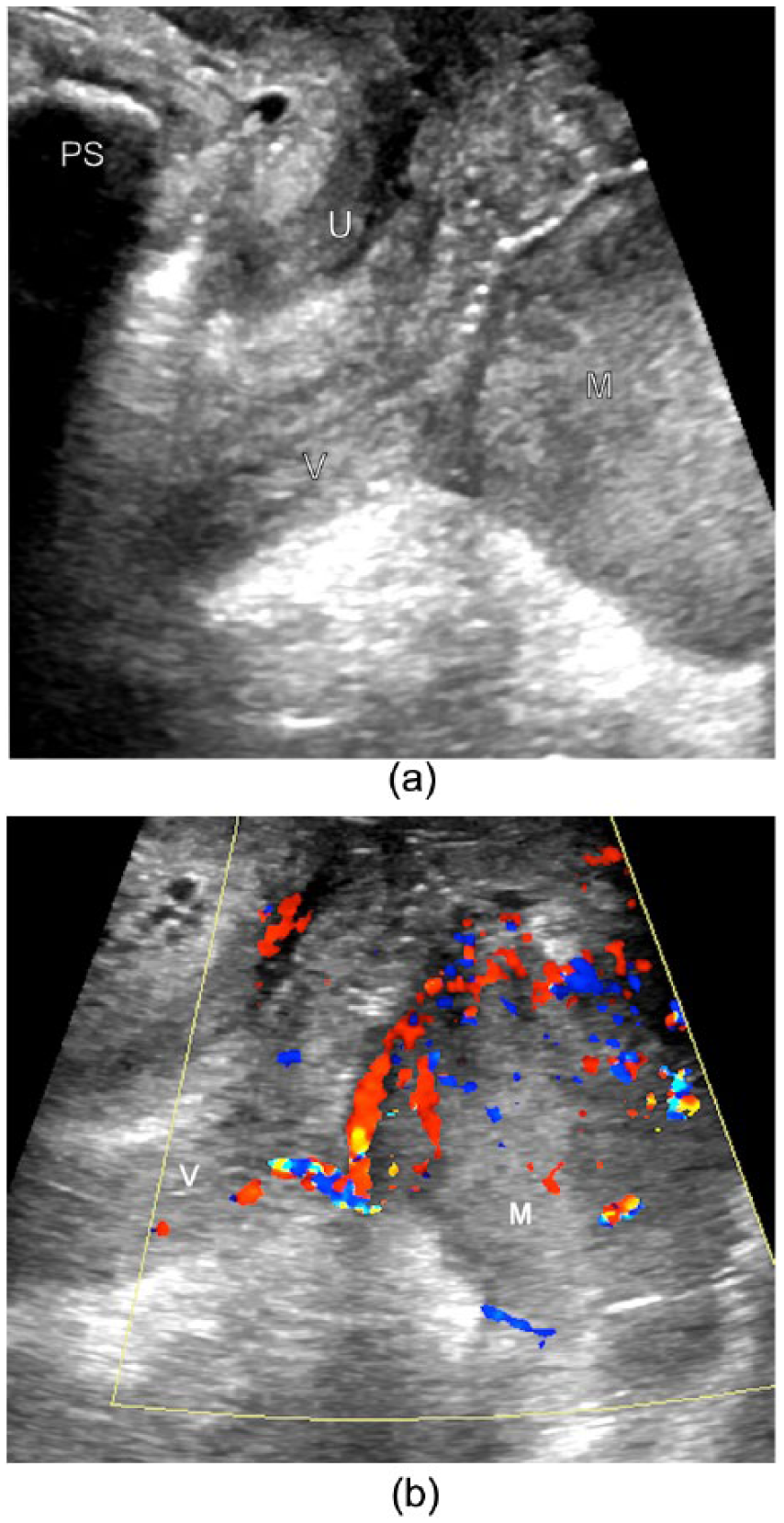
Sagittal transperineal gray-scale (a) and color Doppler (b) sonography images of the lower pelvis demonstrate a mildly echogenic mass (M) posterior to the vagina (V) with blood flow to the mass. PS, pubic symphysis; U, urethra.
MRI was initially deferred because of concern about the safety of the metallic spinal hardware but was subsequently performed after confirming that MRI would be safe. The MRI demonstrated a 5- to 6-cm mass involving the J-pouch, the internal and external anal sphincters, and the mesorectal fascia (Figure 3). Prospective interpretation reported the mass as arising from the J-pouch. No cervical involvement was demonstrated. Five enlarged mesorectal lymph nodes and several pelvic sidewall lymph nodes were seen. A subsequent nuclear medicine positron emission tomography (PET)–CT demonstrated abnormal uptake in the pelvic mass and pelvic lymph nodes, as well as heterogeneous osseous uptake, suggestive of lymph node and marrow metastases. Review of the pelvic MRI did not demonstrate any evidence of marrow involvement.
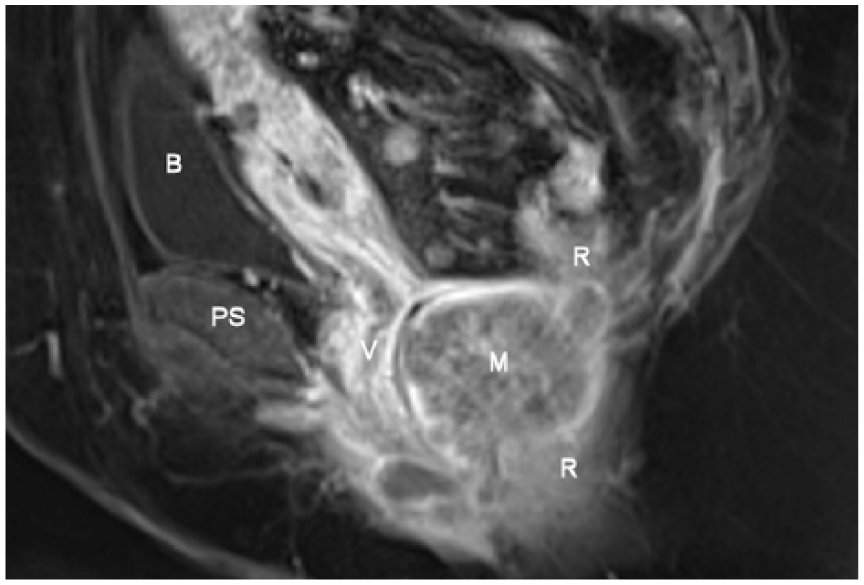
Sagittal T1-weighted fat-saturated magnetic resonance image of the pelvis, acquired after administration of intravenous contrast, demonstrates a mass (M) posterior to the vagina (V) and inseparable from the rectum (R). PS, pubic symphysis; B, bladder.
Pouchoscopy was performed with biopsy of the mass. Histologic diagnosis was high-grade squamous dysplasia, p16 positive, concerning for anal carcinoma, likely extending caudally to involve the J-pouch. A subsequent endoscopy with repeat biopsy demonstrated well-differentiated squamous cell carcinoma. Final diagnosis was anal carcinoma, stage IIIB. Because of the extent of the tumor, surgery could not be performed. Therefore, the patient was treated with chemoradiation. One year posttreatment, the patient was disease free by PET-CT and anoscopy.
Discussion
This case highlights the utility of transperineal sonography in evaluating the ileoanal pouch in patients with perineal symptoms. Transperineal sonography was performed because internal imaging was contraindicated for this patient. The field of view offered by transperineal imaging was optimal for this patient because of the low position of the tumor.
Transperineal sonography can be performed with a curvilinear, linear, or transvaginal transducer. A probe cover with gel both inside and outside the cover helps reduce air between the probe and the perineum and reduce risk of transmission of infection. In this case, a 9-MHz transducer was used, but both higher- and lower-frequency probes can be used for transperineal sonography. A transvaginal probe with 3D imaging capabilities can be used for 3D imaging of the perineum and pelvic floor with a transperineal approach.
For transperineal imaging, the patient is typically in the lithotomy position. With a linear or curvilinear transducer, the transducer is placed over the perineum at the vaginal introitus in the sagittal plane. For female patients, the urethra will be visualized anteriorly and the rectum posteriorly with the vagina in between (Figure 4). Air is often seen in the vagina, which insinuates in small amounts between the folds of the redundant vaginal mucosa. Air is also often seen in the rectum, usually in larger amounts. For male patients, the urethra will be visualized anteriorly with the rectum posteriorly. The pubic symphysis, with posterior shadowing due to ossified bone, is seen anterior to the urethra in male and female patients (Figure 4). Depth can be adjusted as needed for visualization of the distal urethra, vagina, or rectum close to the perineal scanning surface or for visualization of deeper structures, such as the bladder base or cervix. For imaging of the cervix in a pregnant patient, scanning with an empty bladder is recommended. 6 With a transvaginal transducer, the transducer should be placed at the vaginal introitus. Transperineal images can also be obtained at the end of a transvaginal pelvic examination during removal of the transvaginal transducer. Limitations of transperineal sonography include shadowing from rectal gas and limited penetration depth.
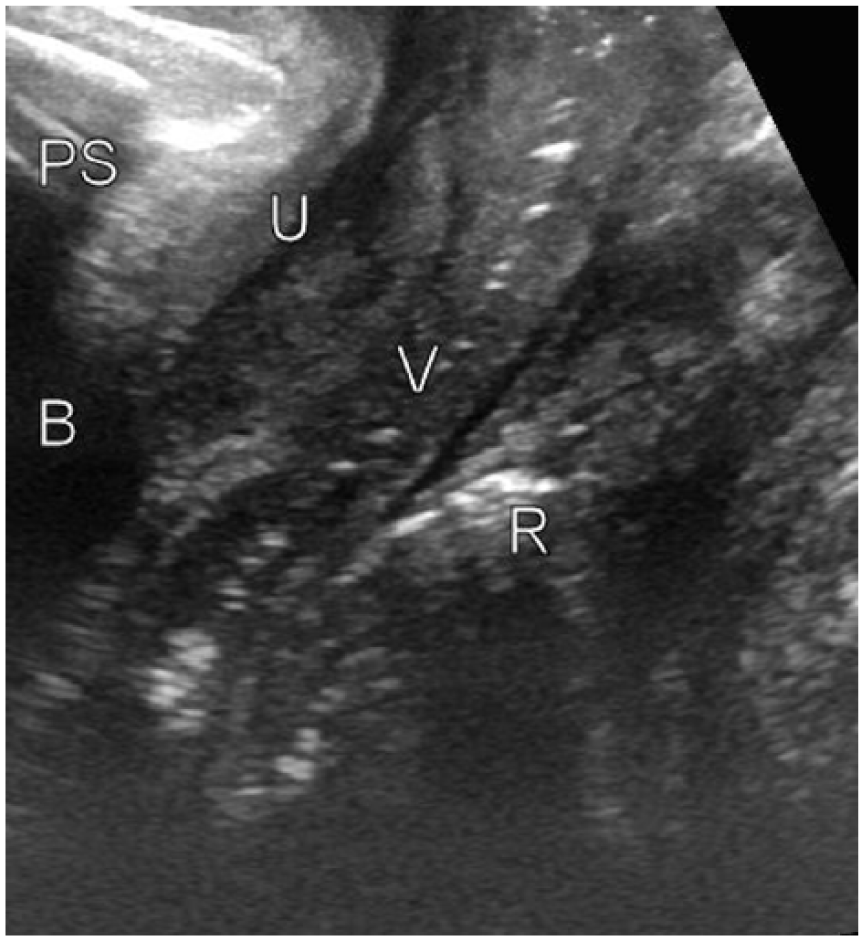
Sagittal transperineal gray-scale sonographic image of a normal female patient. U, urethra; B, bladder; V, vagina; R, rectum; PS, pubic symphysis.
Three-dimensional sonography has been shown to improve diagnostic utility of transperineal sonography for evaluation of the distal intestine.11,12 Because of our patient’s pain, the duration of the examination was limited. Initial transducer choice did not include three-dimensional sonographic capabilities, and the patient was not amenable to further imaging after the initial images were obtained. However, three-dimensional sonography may have been helpful in determining the organ of origin of the visualized mass, which was indeterminate on our study and better demonstrated on subsequent MRI.
About 30% of patients with ulcerative colitis undergo colectomy after unsuccessful medical management or the development of colonic neoplasia. 13 Up to 15 years after colectomy, the incidence of pouch neoplasia is less than 1% and up to 25 years is less than 4%. 14 Squamous cell carcinoma of the ileoanal pouch is extremely rare. Two cases of squamous cell carcinoma of the ileal pouch in patients with history of total colectomy have been reported.15 –17 An additional 6 cases of squamous cell carcinoma arising from the anus in patients with ileoanal pouch have been reported. 17 The prognosis is poor, but treatments are evolving. Treatment options include surgical resection of the pouch and radiation or chemoradiation therapy. 17 Radiation therapy was formerly thought to be contraindicated because of the risk of damaging the fragile mucosa of the pouch. However, a case of successful treatment with chemoradiation without surgery was recently reported. 17 The case study patient was successfully treated with chemoradiation without surgery, which preserved the ileoanal pouch.
This case highlights the utility of transperineal sonography in evaluation of the ileoanal pouch in patients with perineal symptoms. Although internal imaging was contraindicated for this patient, the field of view offered by transperineal sonography was adequate and possibly superior to internal imaging for this patient. Knowledge of the availability of, indications for, and technique of performing transperineal sonography is important for sonographers performing pelvic sonography who may be able to offer this alternative to transvaginal/transrectal sonography and more expensive cross-sectional imaging in the appropriate clinical settings.
Conclusion
Transperineal sonography is a useful imaging tool for evaluating the pelvic floor and lower pelvis. This scanning technique offers an alternative to internal imaging for patients with contraindications to transvaginal and transrectal imaging who have lower pelvic and perineal pathology. The higher spatial resolution offers an advantage over more expensive cross-sectional imaging techniques, such as CT and MRI. The field of view offers visualization of the urethra, bladder base, vagina, lower uterus, distal intestine, and pelvic floor. For this patient with perineal pain, when internal imaging was not clinical feasible, transperineal sonography provided the diagnosis of a distal intestinal mass. Knowledge of the availability of and scanning techniques for transperineal sonography is important in order to be able to offer this useful imaging tool when clinically indicated.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.