
Abstract
Female adnexal tumor of probable Wolffian origin (FATWO) is a rare tumor arising from the remnants of the mesonephric duct and often presents with insidious symptoms. Limited information is available regarding the ultrasonographic characteristics of a FATWO tumor. We present the case of a woman in her mid-40s, G2, P2, with a FATWO tumor while focusing on the ultrasonographic characteristics.
Female adnexal tumor of probable Wolffian origin (FATWO) was first described in 1973 by Kariminejad and Scully and is a tumor primarily occurring in the broad ligament but can occur anywhere along the path of Wolffian (mesonephric) duct regression.1,2 The Wolffian duct regresses by the third embryonic month, but remnants can occur along the path of regression, including in the broad ligament, fallopian tube, ovarian hilum, peritoneum, or the mesosalpinx.3,4 Presenting symptoms of FATWO include abdominal pain or urinary symptoms caused by anatomical protrusion of the mass onto the bladder. 5 The following case presents the ultrasonographic characteristics of this rare adnexal tumor.
Case Report
A white woman in her mid-40s, gravida 2, para 2, presented to her gynecologist’s office with pelvic pain for two months. Her gynecologic history was remarkable for a previously diagnosed subserosal uterine fibroid and use of a Mirena (Bayer, Levenkusen, Germany) intrauterine device (IUD) for contraception. Physical examination revealed a soft, nontender abdomen without the presence of ascites or palpable masses. Pelvic examination was notable for the IUD string extruding from the cervix, a normal-appearing vagina and cervix, and an unremarkable uterus and ovaries on bimanual examination. The patient was referred for pelvic ultrasonography secondary to a known fibroid and new-onset pelvic pain.
Two-dimensional (2D) and three-dimensional (3D) ultrasonography was performed with a Voluson 730 Expert system (GE Healthcare, Milwaukee, Wisconsin) with a 5- to 9-MHz broadband transvaginal probe. The uterus appeared normal with the IUD properly located within the endometrial cavity. The ovaries were not enlarged and contained small follicles. A previously diagnosed subserosal myoma measuring 10 × 13 × 13 mm was visualized. A complex solid and cystic mass was visualized in the right adnexa next to the right ovary and measured 33 × 36 × 25 mm (Figure 1). Independent movement of the mass and ovary was visualized when gentle pressure was applied with the endovaginal probe. The mass had a mixed echogenic pattern with scattered echogenic foci and no acoustic shadowing (Figure 2). Color Doppler was used to evaluate vascular flow, and it demonstrated minimal flow throughout the mass (Figure 3). The 3D volume data sets were used to produce a rendered coronal image of the mass. The mass appeared to be connected to the uterine corpus by a small pedicle (Figure 4). Based on the ultrasound images, a pedunculated fibroid was suspected.
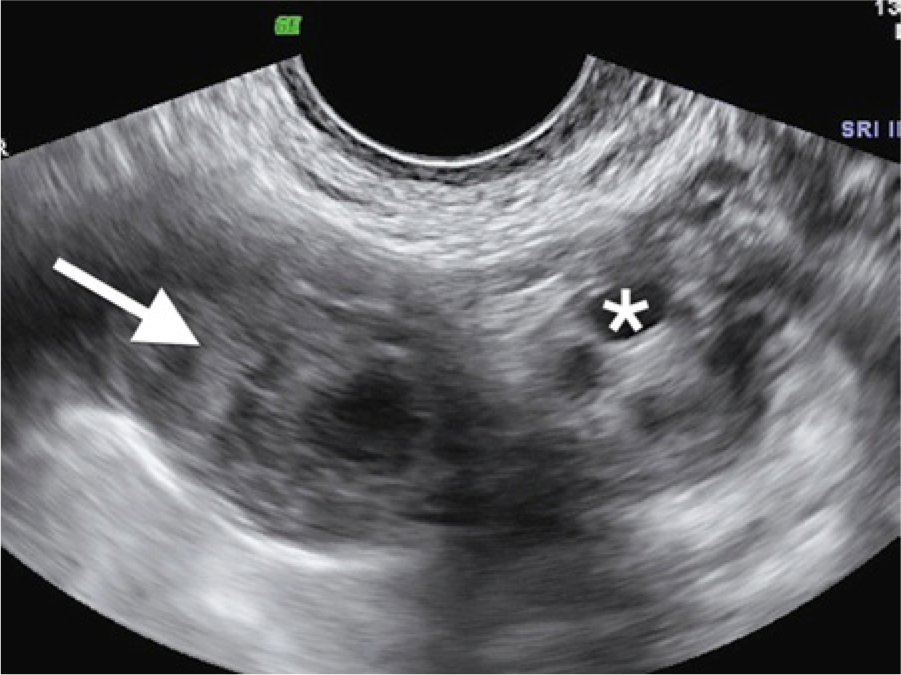
A complex right adnexal mass (arrow) is seen adjacent to the right ovary (*). Small follicles can be seen in the right ovary.
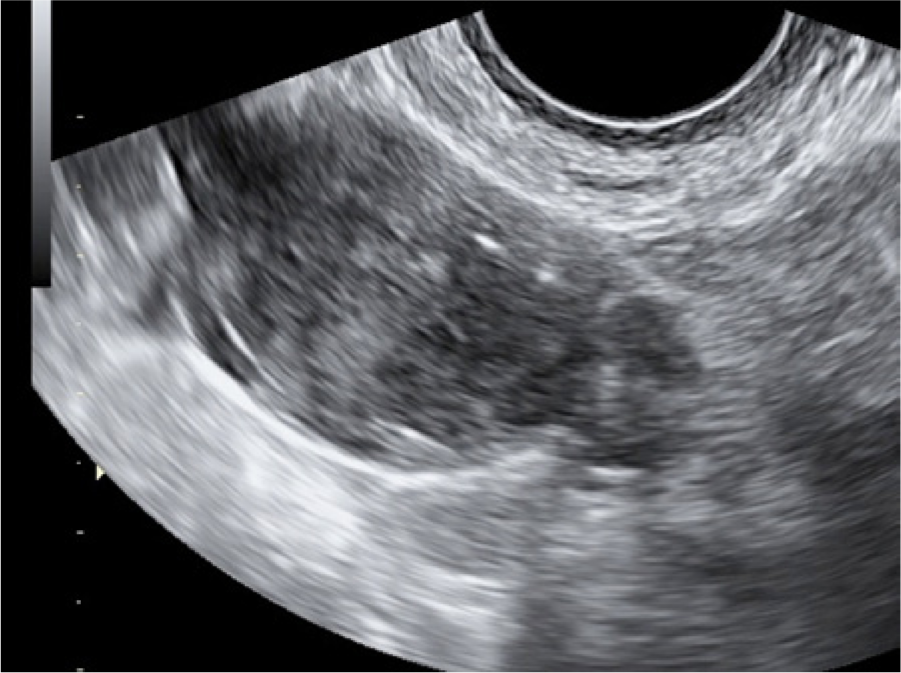
The right adnexal mass demonstrates a mixed echogenic pattern with scattered echogenic foci. There is no evidence of acoustic shadowing.
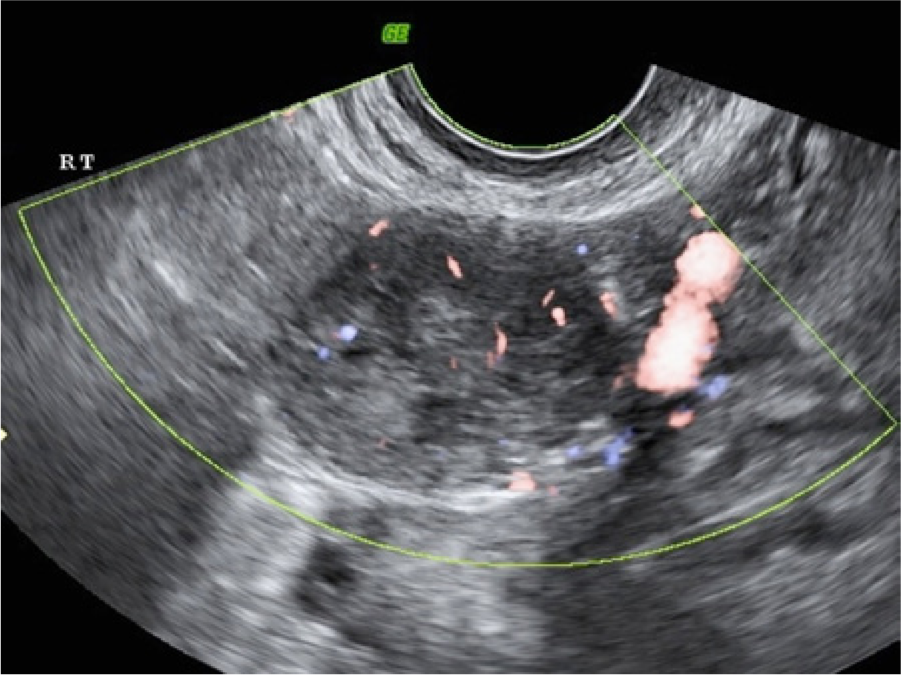
Color Doppler evaluation shows minimal vascularization throughout the mass.
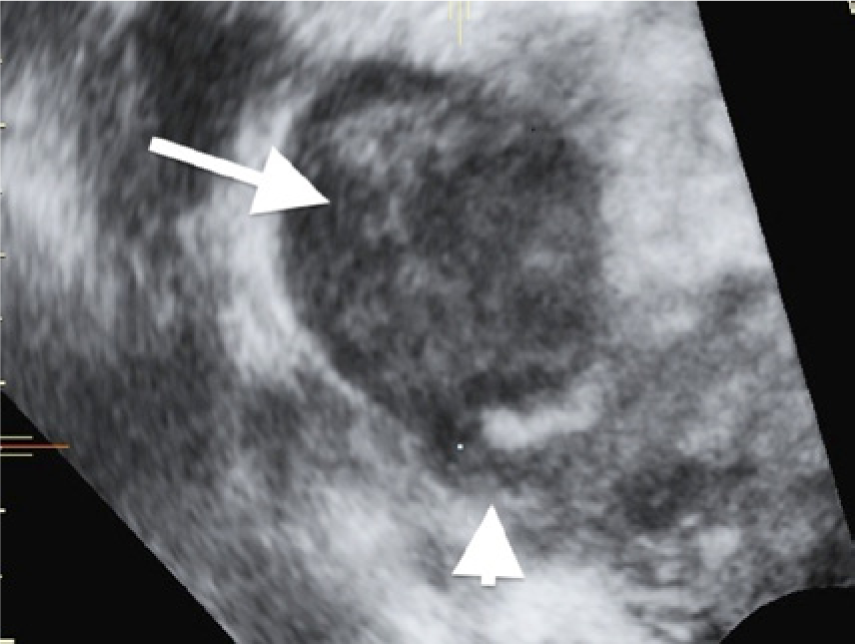
Rendered coronal image of the right adnexal mass. The mass (arrow) appears to be connected to the uterus by a small pedicle (arrowhead).
The patient was counseled on several treatment options, including expectant, surgical, or medical management. Given her ongoing pelvic pain and absent desire for future fertility, she chose to pursue surgical management. At the time of surgery, the right ovary and tube appeared normal. A spherical mass measuring 3.5 cm in diameter with a thin connection to the right fallopian tube was present within the mesosalpinx. The mass was entirely separate from the right ovary. There was no identifiable connection to the uterus. The mass was excised and sent for frozen pathologic evaluation. A total abdominal hysterectomy and bilateral salpingo-oophorectomy was performed. Upon completion of the hysterectomy, the frozen pathologic results returned and were consistent with a granulosa cell tumor. Thus, a gynecologic oncologist was consulted and surgical staging was performed.
Final histologic sections from the right adnexal mass demonstrated a cellular tumor composed of round to oval-shaped cells arranged in trabeculae and small glands. Immunohistochemical staining performed on the tumor tissue was weakly positive for inhibin; negative for the cell surface enzyme CD10, chromogranin, epithelial membrane antigen (EMA), and cytokeratin 7 (CK7); and positive for reticulin, vimentin, cytokeratin CAM 5.2, and calretinin. Immunohistochemical staining results were consistent with a FATWO. The patient was instructed to follow up with gynecologic oncology for clinical surveillance.
Discussion
Differential diagnosis of a FATWO includes granulosa cell tumor, Sertoli-Leydig tumor, endometrial adenocarcinoma, clear cell carcinoma, and pedunculated myoma.1,2,6 Macroscopically, FATWO appears as a pale yellow mass with both solid and cystic components and may have areas of hemorrhage or necrosis. 5 Microscopically, FATWOs contain well-differentiated epithelial cells forming sieve-like cystic patterns that are tightly arranged, contain few mitotic figures, and have a thick basal lamina.5–7 Immunohistochemically, FATWOs stain positive for pan-cytokeratin, CAM 5.2, CK7, and vimentin. 5 There are conflicting data regarding reactivity for inhibin. Different studies report positive, focally positive, and negative staining for inhibin.1,4,6 Thus, immunohistochemistry does not have a central role in FATWO diagnosis. 2
There is little published literature on the ultrasonographic features of a FATWO. The tumor often appears as a complex mass with both solid and cystic components. Acoustic shadowing has been reported; however, shadowing was not present in our case. A connection to the fallopian tube may be identified.2,3,5,8 FATWO may be misidentified by sonography as a pedunculated leiomyoma. Blood flow in the tumor demonstrated by color Doppler is variable; some tumors appear highly vascularized, and others have little or no discernible vascular flow. 2 FATWOs most commonly occur in the broad ligament but can occur anywhere along the remnants of the mesonephric duct.1,2 A FATWO should be considered if a complex solid and cystic mass separate from the ovary is visualized in the paravaginal, paraovarian, or retroperitoneal regions on sonography.
FATWOs are generally regarded as benign lesions, but 10% can recur or metastasize.1,5,6,9 Therefore, they are often referred to as tumors of low malignant potential. 5 When FATWOs recur or metastasize, they are generally found in the broad ligament but have been reported in the hepatic and pulmonary systems. 5 Sivridis et al 10 published criteria to distinguish malignant from benign FATWO lesions. Lesions should be considered malignant if the size is >100 mm and they are hypercellular, contain capsular invasion, or have evident capsule rupture with obvious metastasis. There is limited evidence on the efficacy of chemoradiation in the treatment of malignant and recurrent FATWOs. Multiple chemotherapy and radiation regimens are used given the paucity of evidence.6,9 Clinical follow-up is recommended every six months for the first two years and then annually thereafter.
Conclusion
FATWO is an uncommon tumor that appears as a complex mass on transvaginal ultrasound. Key ultrasonographic characteristics include a mixed echogenic pattern with both solid and cystic components. This tumor can also be demonstrated to be separate from other adnexal structures, including the ovaries. When a FATWO is suspected, the patient should be referred to a gynecologic oncology specialist for surgical management and clinical surveillance secondary to the malignant potential of this neoplasm.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.